
In today’s post, we seek to:
- Understand what artificial intelligence (AI) is
- Generate a basic understanding of how AI works
- Review applications of AI in the Emergency Department (ED):
- Patient care
- Predictive Analytics
- ED Operations
Intelligence
Intelligence represents the ability to perceive information, retain it as knowledge, and apply it towards adaptive behaviours within an environment or context.
Evolution of Artificial Intelligence
Artificial intelligence is not new, the beginnings of AI started as computer programs that began to incorporate sensors to provide information about their environment. A great example of this is the RoombaTM: a sensor provides information to the vacuum, enabling it to navigate a room differently (and uniquely) than if it were programmed to clean a standard room.
Over time, the evolution of AI has led to less human involvement. The 1950s introduced neural networks, so named due to their structural resemblance to the human brain. The system follows similar logic to that of the biological mantra ‘neurons that fire together, wire together.’
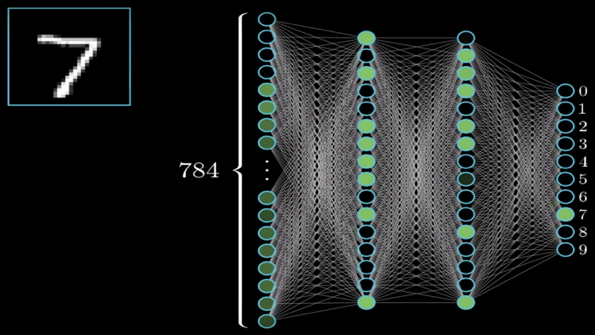
The above photo is an example of the classic ‘number identification’ neural network. The system uses the colour of the pixel as an input (28 x 28 pixels = 784) and then gives an output as an integer, from 0 – 9. The math in the middle is where the ‘learning’ happens. To simplify the math: the model takes a guess and assigns a cost penalty for how wrong it is. It then keeps guessing until it’s able to minimize the cost penalty, getting more and more accurate with each guess. Eventually, after taking enough guesses, the model has been ‘trained’ to accurately guess numbers it has never seen before. The number of guesses required varies by the complexity of the task and the degree of accuracy desired.
Modern Day Medical Uses of Artificial Intelligence
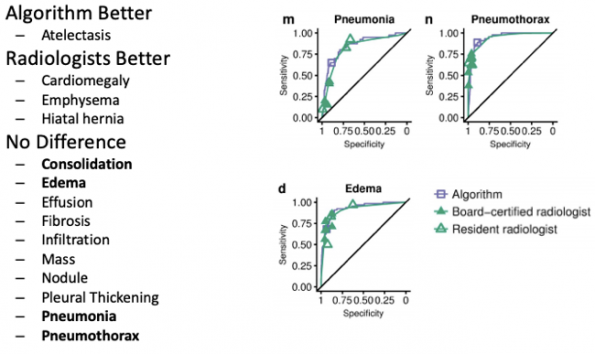
A group in Stanford [1] developed an algorithm which analyses AP and PA chest radiographs. The model was trained on 112,000 radiographs to develop it. The final model was then tested against 9 radiologists at different institutions for their ability to diagnose 14 pathologies. The results show that, for most pathologies, there was no difference in their abilities. Notably, in the comparison group, 420 images were reviewed in 4 hours by the radiologists, but only 90 seconds by the computer algorithm.
Similar models have been designed for non-contrast head CT scans. Researchers in India trained a model against 313,000 CT head scans to detect various intra- and extra-axial bleeds, fractures, midline shift, and mass effect [2]. The model was compared to three staff radiologists. The model’s performance had an area under the curve (AUC) of 0.96 for bleeds, 0.92 for fractures, and 0.93 for mass.
Similar models have been developed for ECGs [3], echocardiograms [4], and skin lesions [5].
Big Data in the ED
Predictive Analytics
In the age of Electronic Medical Records (EMRs) and digital computing systems, hordes of data exist which are being used to detect patterns and make predictions about likely future clinical situations. Researchers at St. Michael’s Hospital in Toronto have developed an algorithm that can predict the daily census in the ED every 6 hours for 3 days into the future within 5% accuracy [6]. The model factors in historical trends in patient volume, day of the week, relationships to major holidays, and even temperature and climate.
Machine learning algorithms stand to change the way precious departmental resources are triaged [7]. Models use a patient’s age, sex, arrival mode, chief complaint, vitals, and past medical history to predict hospitalization, emergency surgery, ICU admission, and even mortality. This tool has the potential to help differentiate a rather heterogeneous population that often exists within the current triage ‘categories,’ whether you use the Canadian Triage Acuity Scale (CTAS), the Emergency Severity Index (ESI), and the Manchester Triage System; all five-level scales.
Simulation
Hospital-wide databases often collect timestamp data for many important events that happen as patients flow through the ED. This data is perfect for use in Discrete Event Simulation (DES). DES is a technique used in industrial engineering whereby a computer model (in this case of an ED) is made to replicate the current state. Resources such as physicians, nurses, clerks, and stretchers are incorporated alongside process maps for all relevant patient activities; triage, registration, RN and MD assessments, work-up, and disposition. After validation against real timestamped data, the simulation can be run with changes to demonstrate the impact quantitatively. Simulation allows us to understand a complex system and how manipulation of each part affects others: sometimes knowingly or unknowingly. This has implications in QI initiatives to optimize staff schedules and bed vs. chair space.
Simulation has been used in ED administration before. A hospital in Moncton, NB used simulation to decide between adding an additional MD, RN, or treatment room to see how best to decrease wait times in their ED [8]. A group at the University of Virginia Medical Centre ED used simulation to optimize their MD schedule to minimize wait times [9]. Further uses include analyzing reasons for offload delay [10]. The power of simulation in a system as complex as the ED is impressive. Not only does quantification of crowding and flow metrics give weight to decisions, but timely and disruptive trials can be tested on a computer before implemented in the ED.
The Future
Artificial intelligence is a booming field right now. It is only a matter of time before it revolutionizes the way we practice medicine.
As algorithms get more complex and more accurate, they will be able to outperform humans, and our workflows will need to be augmented. Algorithms are already being developed to expand utility in radiology and dermatology. Some models are outperforming surgeons in procedural skills in controlled settings. It is only a matter of time before computers are suggesting diagnoses, treatment plans, and prognosticating better than physicians due to their superior ability to quickly scan large volumes of data (i.e. a patient’s entire chart).
We need to start thinking about incorporating this into our existing care and training systems, as significant parts of physician workflow will be replaced in the future. We should view this as an exciting opportunity to incorporate a powerful technology into our ability to care for patients and not push back out of fear of computers replacing us all.
References
[1] Rajpurkar, P., Irvin, J., Ball, R., Zhu, K., Yang, B., Mehta, H., . . . Lungren, M. (2018). Deep learning for chest radiograph diagnosis: A retrospective comparison of the CheXNeXt algorithm to practicing radiologists. PLOS Medicine, 15(11), e1002686.
[2] Chilamkurthy, S., Ghosh, R., Tanamala, S., Biviji, M., Campeau, N., Venugopal, V., . . . Warier, P. (2018, December 1). Development and Validation of Deep Learning Algorithms for Detection of Critical Findings in Head CT Scans. The Lancet, 392(10162), 2388-2396.
[3] Hannun, A.Y., Rajpurkar, P., Haghpanahi, M., Tison, G.H., Bourn, C., Turakhia, M.P., Ng, A.Y. (2019). Cardiologist-level arrhythmia detection and classification in ambulatory electrocardiograms using a deep neural network. Nature Medicine, 25, 65-69.
[4] Madani, A., Arnaout, R., Mofrad, M., Arnaout, R. (2018). Fast and accurate view classification of echocardiograms using deep learning. Digital Medicine, 1, 6.
[5] Esteva, A., Kuprel, B., Novoa, R.A., Ko, J., Swetter, S.M., Blau, H.M., Thrun, S. (2017). Dermatologist-level classification of skin cancer with deep neural networks. Nature, 542, 115-118.
[6] Shah, S., Murray, J., Mamdani, M., & Vaillancourt, S. (2019). The Impact of Snowfall on Patient Attendance at an Urban Academic Emergency Department. Canadian Association of Emergency Physicians(p. 1). Halifax: Canadian Association of Emergency Physicians.
[7]Levin, S., Toerper, M., Hamrock, E., Hinson, J., Barnes, S., Gardner, H., . . . Kelen, G. (2018). Machine-Learning-Based Electronic Triage More Accurately Differentiates Patients With Respect to Clinical Outcomes Compared With the Emergency Severity Index. Annals of Emergency Medicine, 71(5), 565-574.
[8] Duguay, C., Chetouane, F. (2007). Modeling and Improving Emergency Department Systems using Discrete Event Simulation. Simulation, 83(4), 311-320.
[9]Rossetti, M., Trzeinski, G., & Syverud, S. (1999). Emergency Department Simulation and Determination of Optimal Attending Physician Staffing Schedules. Simulation – A Bridge to the Future.2, pp. 1532-1540. 1999 Winter Simulation Conference Proceedings.
[10] Laan, C.M., Vanberkel, P.T., Boucherie, R.J., Carter, A.J.E. (2016). Offload zone patient selection criteria to reduce ambulance offload delay. Operations Research for Health Care, 11, 13-19.


Trackbacks/Pingbacks