
What is Bupropion?
Bupropion is an anti-depressant commonly prescribed for seasonal affective disorder, as a smoking cessation aid, and off-label in the management of major depressive disorder. You may know it by the trade names Wellbutrin, Zyban or Champix. While frequently compared to SSRIs, it has a unique mechanism of action – it is a norepinephrine-dopamine reuptake inhibitor, with barely any serotonergic activity (1–3).
Bupropion was first released on the market in 1985, and then promptly withdrawn due to reports of seizures at ‘therapeutic’ doses of 600mg. The drug was later re-introduced in 1989 with a black box warning regarding its potential for seizures and a recommended maximum prescribed dose of 450mg. It has one of the lowest therapeutic indices of commonly prescribed medications currently on the market.

A Drug of Interest
This drug is of interest to the emergency physician for a number reasons:
- Since its re-release, it has become increasingly popular, particularly among young individuals who find the side effect profiles of SSRI class medications intolerable.
- It can be lethal in overdose
- Studies comparing Bupropion overdoses to those of SSRIs and TCAs found that 44% of Bupropion overdoses required ICU level care, 30% of patients had seizures, 1% required vasopressors, 5% required airway management and 0.3% died (3,4).
- The harm profile is more similar to TCAs than it is to SSRIs, despite frequently being compared to the latter class of antidepressants.
- In overdose, bupropion ranges from causing tachycardia and nausea to intractable seizures and fulminant cardiovascular collapse.
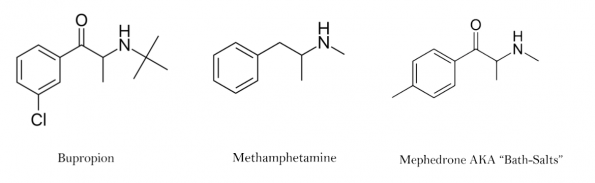
- It can be abused, providing a high similar to methamphetamine or bath salts when inhaled (6)
Bupropion Formulations
A key initial component of managing the bupropion toxic patient is identifying the formulation of drug which they have ingested. There are three different formulations of bupropion, with highly variably kinetics:
- Instant Release (IR) – Peak concentration @ 2 hours
- Sustained Release (SR) – Peak concentration @ 3 hour
- Extended Release (XR or ER) – Peak concentration @ 9 hours
Predicting Seizures
Bupropion overdoses have a high risk of seizures. The drug also presents a difficult prediction of its clinical course. This is in part due to the various formulations and associated kinetics.
- Timing of seizure can be quite delayed after ingestion
- 30% of seizing patients seize >8 hours
- 50% of seizing patients seize recurrently
- While greater doses are associated with an increased likelihood of seizure, most studies found comparable ingested doses amongst seizing and non-seizing overdose cohorts.
- While greater doses increase the likelihood of seizures, they do not cause seizures earlier.
- The timing of the first seizure does not predict recurrence.

Initial studies attempting to predict features associated with toxicity were very discouraging (7,8). Fortunately, a 2008 study by Starr et al. identified three clinical tools facilitating assessment of bupropion overdoses:
- Tachycardia – 91.2% sensitive, 48.8% specific
- Agitation – 29.7% sensitive, 87.5% specific
- Tremor – 21.6% sensitive, 85.0% specific
Tachycardia is a good rule-out test, while agitation and tremor are adequate rule-in tests (9).
Management of Bupropion Overdoses
- Decontamination
- Bupropion should undergo early decontamination.
- It has a few unique features which make it amenable to late decontamination:
- Pill capsules can take >24 hours to dissolve (10)
- Partially dissolved pill capsules still containing active drug have been found in excrement days after overdose (11)
- It forms bezoars (12,13)
- Seizures
- Benzodiazepines are first line for management of the seizing bupropion overdose
- Propofol and barbiturates are second and third line agents (14,15)
- Phenytoin, carbamazepine and valproic acid should be avoided due to evidence of harm in toxic seizures (15)
- Levetiracetam has no supporting evidence in the management of bupropion overdose and is currently not recommended (16)
- Cardiotoxicity
- This is a rare and often fatal development in bupropion overdoses.
- The pathophysiology is unique:
- While often touted as a sodium channel blocking agent, this is based largely on an animal study from 1981 which led bupropion to be compared to TCAs (17).
- More recent evidence by a Canadian group however suggests that bupropion actually manifests cardiotoxicity by interfering with gap junctions (membrane proteins critical for cells to communicate with one another) causing loss of coordinated cardiomyocyte function (18). It prolongs the QRS interval via gap junction toxicity.
- Bupropion does not have sodium channel blocking properties.
- It is the only drug we know of with this mechanism of toxicity.
- Management:
- Ultrasound
- It is recommended to perform cardiac POCUS particularly in patients with early signs of neurotoxicity, as identifying cardiotoxicity prior to fulminant cardiovascular collapse may allow time for potentially life-saving interventions.
- Sodium Bicarbonate
- Given that sodium channel blockade does not occur in bupropion overdose, sodium bicarbonate does not have biological plausibility as a treatment mechanism.
- Additionally, there is an abundance of literature showing no beneficial outcome with this treatment in the context of bupropion poisoning (19–24).
- Lipid Emulsion
- Lipid emulsion theoretically functions by two mechanisms in the treatment of overdose:
- It acts as a lipid sink; functioning as intravenous decontamination and causing lipophilic drugs like bupropion to diffuse out of to tissues affecting by toxicity and into the lipid-rich blood stream due to basic diffusion gradients.
- It provides the heart with free fatty acids – an additional energy source to sustain myocardial tissue.
- Evidence for lipid emulsion in the context of cardiac arrest is weak, however given absence of other options, this is a reasonable consideration (28,29).
- Lipid emulsion theoretically functions by two mechanisms in the treatment of overdose:
- VA-ECMO
- Literature addressing ECMO for bupropion overdose is extremely limited and based on only a few case reports of successful intervention.
- Given good biological plausibility, and lack of comorbidities in most patients with bupropion overdose, ECMO should be a major consideration in the management of patients with severe bupropion overdose in refractory shock states presenting to ECMO capable centres(30,31).
- Ultrasound
Take-home Points
- Bupropion comes in several formulations with various pharmacologic profiles.
- Tachycardia is a useful rule out tool when predicting seizures (91.2% sensitive).
- Agitation and tremor are decent predictors of seizures (87.5 & 85% specific, respectively).
- Overdoses require decontamination.
- Bupropion forms bezoars and is amenable to late decontamination.
- There is no role for sodium bicarbonate in managing bupropion overdoses.
- Lipid emulsion should be administered to the hypotensive or arrested bupropion overdose.
- VA-ECMO, if your centre is capable, is a potential means of managing refractory shock states.
References
- Tracey JA. Zyban® – Is there a cause for concern? Vol. 1, Expert Opinion on Drug Safety. Expert Opin Drug Saf; 2002. p. 303–5.
- Stall N, Godwin J, Juurlink D. Five things to know about ⋯: Bupropion abuse and overdose. CMAJ. 2014 Sep 16;186(13):1015.
- Overberg A, Morton S, Wagner E, Froberg B. Toxicity of bupropion overdose compared with selective serotonin reuptake inhibitors. Pediatrics. 2019;144(2).
- Sheridan DC, Lin A, Zane Horowitz B. Suicidal bupropion ingestions in adolescents: increased morbidity compared with other antidepressants. Clin Toxicol. 2018 May 4;56(5):360–4.
- Finkelstein Y, Hutson JR, Freedman SB, Wax P, Brent J. Drug-induced seizures in children and adolescents presenting for emergency care: Current and emerging trends. Clin Toxicol. 2013 Sep;51(8):761–6.
- Lewis JC, Sutter ME, Albertson TE, Owen KP, Ford JB. An 11-year review of bupropion insufflation exposures in adults reported to the California poison control system. Vol. 52, Clinical Toxicology. Informa Healthcare; 2014. p. 969–72.
- Spiller HA, Ramoska EA, Krenzelok EP, Sheen SR, Borys DJ, Villalobos D, et al. Bupropion overdose: A 3-year multi-center retrospective analysis. Am J Emerg Med. 1994;12(1):43–5.
- Shepherd G, Velez LI, Keyes DC. Intentional bupropion overdoses. J Emerg Med. 2004;27(2):147–51.
- Starr P, Klein-Schwartz W, Spiller H, Kern P, Ekleberry SE, Kunkel S. Incidence and onset of delayed seizures after overdoses of extended-release bupropion. Am J Emerg Med. 2009 Oct;27(8):911–5.
- Spiller HA, Bottei E, Kalin L. Fatal bupropion overdose with post mortem blood concentrations. Forensic Sci Med Pathol. 2008 Mar;4(1):47–50.
- Overberg A, Purpura A, Nanagas K. “Ghost tablet” husks excreted in feces in large bupropion XL overdose. Clin Toxicol. 2019 Feb 1;57(2):141–2.
- Donnelly K, Walkowiak HB, Donnelly C, Jenkinson E, Rizkalla J, Langford N. Bupropion toxicokinetic: A case report. Clin Toxicol. 2010 Apr;48(4):385–7.
- Schmit G, De Boosere E, Vanhaebost J, Capron A. Bupropion Overdose Resulted in a Pharmacobezoar in a Fatal Bupropion (Wellbutrin®) Sustained-release Overdose: Postmortem Distribution of Bupropion and its Major Metabolites. J Forensic Sci. 2017 Nov 1;62(6):1674–6.
- Tutka P, Mróz T, Klucha K, Piekarczyk M, Wielosz M. Bupropion-induced convulsions: Preclinical evaluation of antiepileptic drugs. Epilepsy Res. 2005 Mar;64(1–2):13–22.
- Shah ASV, Eddleston M. Should phenytoin or barbiturates be used as second-line anticonvulsant therapy for toxicological seizures. Clin Toxicol. 2010;48(8):800–5.
- Lee T, Warrick BJ, Sarangarm P, Alunday RL, Bussmann S, Smolinske SC, et al. Levetiracetam in toxic seizures. Clin Toxicol. 2018 Mar 4;56(3):175–81.
- Wang CM, Parker CH, Maxwell RA. Electrophysiological effects of antidepressants on mammalian hearts and crayfish giant axon. J Cardiovasc Pharmacol. 1981;3(1):101–12.
- Caillier B, Pilote S, Castonguay A, Patoine D, Ménard-Desrosiers V, Vigneault P, et al. QRS widening and QT prolongation under bupropion: A unique cardiac electrophysiological profile. Fundam Clin Pharmacol. 2012 Oct;26(5):599–608.
- Curry SC, Kashani JS, LoVecchio F, Holubek W. Intraventricular conduction delay after bupropion overdose. J Emerg Med. 2005 Oct;29(3):299–305.
- Franco V. Wide complex tachycardia after bupropion overdose. Am J Emerg Med. 2015 Oct 1;33(10):1540.e3-1540.e5.
- Al-Abri SA, Orengo JP, Hayashi S, Thoren KL, Benowitz NL, Olson KR. Delayed bupropion cardiotoxicity associated with elevated serum concentrations of bupropion but not hydroxybupropion. Clin Toxicol. 2013 Dec;51(10):1230–4.
- Rivas-Coppola MS, Patterson AL, Morgan R, Wheless JW. Bupropion overdose presenting as status epilepticus in an infant. Pediatr Neurol. 2015 Sep 1;53(3):257–61.
- Weerdenburg K, Finkelstein Y. A 12-Year-old girl with seizures after intentional drug overdose. Pediatr Emerg Care. 2015 Mar 15;31(3):217–9.
- Zhu Y, Kolawole T, Jimenez XF. Atypical Findings in Massive Bupropion Overdose: A Case Report and Discussion of Psychopharmacologic Issues. J Psychiatr Pract. 2016 Sep 1;22(5):405–9.
- Chhabra N, DesLauriers C, Wahl M, Bryant SM. Management of severe wellbutrin poisoning with intravenous lipid emulsion. Clin Toxicol. 2018 Jan 2;56(1):51–4.
- Bucklin MH, Gorodetsky RM, Wiegand TJ. Prolonged lipemia and pancreatitis due to extended infusion of lipid emulsion in wellbutrin overdose. Clin Toxicol. 2013 Nov;51(9):896–8.
- Livshits Z, Feng Q, Chowdhury F, Amdo TD, Nelson LS, Hoffman RS. Life-Threatening wellbutrin Ingestion: Is There a Role for Intravenous Fat Emulsion? Basic Clin Pharmacol Toxicol. 2011 Nov;109(5):418–22.
- Sirianni AJ, Osterhoudt KC, Calello DP, Muller AA, Waterhouse MR, Goodkin MB, et al. Use of Lipid Emulsion in the Resuscitation of a Patient With Prolonged Cardiovascular Collapse After Overdose of wellbutrin and Lamotrigine. Ann Emerg Med. 2008;51(4).
- Gosselin S, Hoegberg LCG, Hoffman RS, Graudins A, Stork CM, Thomas SHL, et al. Evidence-based recommendations on the use of intravenous lipid emulsion therapy in poisoning*. Vol. 54, Clinical Toxicology. Taylor and Francis Ltd; 2016. p. 899–923.
- Heise CW, Skolnik AB, Raschke RA, Owen-Reece H, Graeme KA. Two Cases of Refractory Cardiogenic Shock Secondary to wellbutrin Successfully Treated with Veno-Arterial Extracorporeal Membrane Oxygenation. J Med Toxicol. 2016 Sep 1;12(3):301–4.
- Shenoi AN, Gertz SJ, Mikkilineni S, Kalyanaraman M. Refractory hypotension from massive wellbutrin overdose successfully treated with extracorporeal membrane oxygenation. Pediatr Emerg Care. 2011 Jan;27(1):43–5.

