

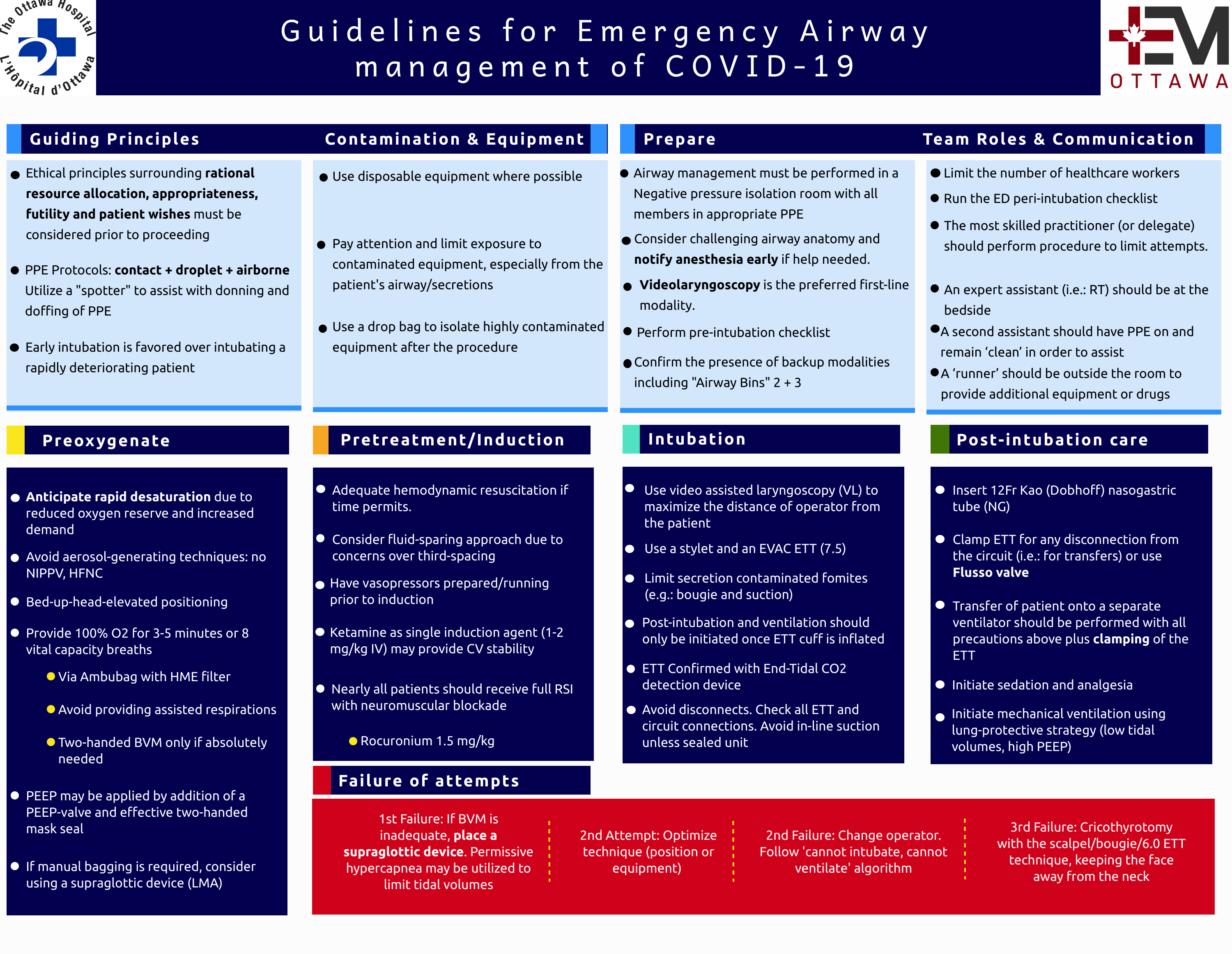
Guiding Principles
- Suspected SARS-COV-2 patients showing signs of hypoxemic respiratory failure should be intubated proactively, as early as possible. Signs may include FiO2 requirement > 50%, clinical signs of respiratory fatigue despite supplemental oxygen, or hemodynamic instability. Do not wait for rapid deterioration to act!
- Such unstable respiratory failure patients in the ED – whether under the care of Emergency or “Inpatient” services – should be managed by the most experienced and immediately available physician, typically the Emergency Physician on duty. In cases where “consulted”/admitted patients can be maintained in a stable state without intubation, rapid access ICU team consultation and transfer to ICU is encouraged.
- Ethical principles surrounding rational resource allocation, appropriateness/futility, and patient wishes must be considered prior to proceeding. Future guidelines are in development to aid in appropriate patient selection.
- From an oxygenation perspective:
- First line therapy for COVID-19 suspected/confirmed is the use of oxygen by nasal prongs up to a maximum of 6L/minute
- If patient remains hypoxemic on 6 LPM oxygen by nasal prongs, proceed to administration of non-rebreather mask with filter at flow rates of up to 20 LPM.
- If patient remains hypoxemic and/or dyspneic on non-rebreather mask then patient should be transferred to a negative-pressure room, private room with door closed or a COVID cohorted ward, with healthcare workers adopting full airborne/droplet/contact PPE prior to room entry and at that point high-flow nasal oxygen (HFNO- Maxtec/Airvo/Nasal moustache >6L/min) therapy and/or non-invasive ventilation (NIV – including BiPAP and/or CPAP) can be commenced
- For COVID-19 suspected and/or confirmed patients refractory to nasal prong therapy, high-flow nasal oxygen (HFNO) therapy should be considered ahead of non-invasive ventilation (NIV)
- Important note: if aerosol-generating procedures are unavoidable, they must be performed in a negative pressure room (AIIR) or a designated, cohorted area where all staff are in Contact+Droplet+Airborne PPE.
- Keep both the number of people and the duration of exposure to a minimum.
- Wear the correct PPE: Contact+Droplet+Airborne. DON and DOFF under supervision with cross-checks.
- Verbalize clear plans and use checklists (Appendices A & B) whenever possible.
- Optimize post-intubation care with analgesia, sedation, and lung-protective ventilation.
System Preparations
Airway bundles
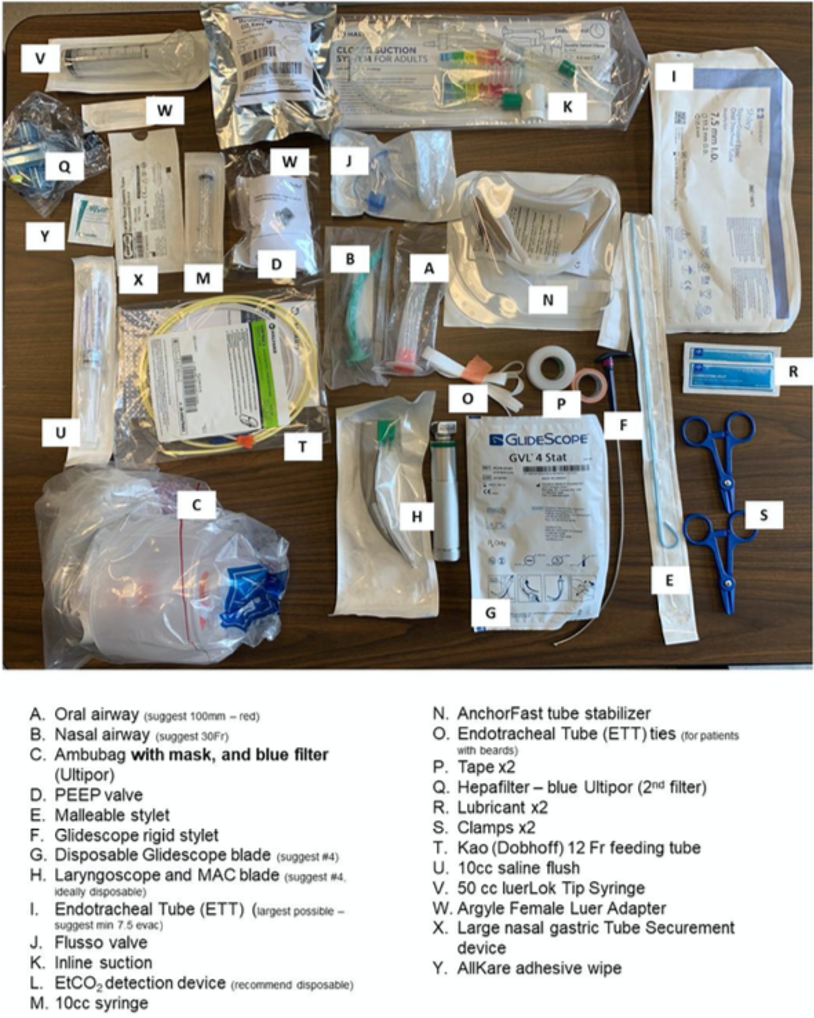
The Emergency Departments have been stocked with standardized intubation equipment bins. These bins will be maintained by the RT’s and are harmonized with ICU to streamline the stocking and checking process.
Bin #1: everything needed for preoxygenation (filtered BVM with PEEP, OPA/NPA), intubation (prefer glidescope), and setting up the vent circuit. There’s a disposable direct laryngoscope in there as well – just in case. Also a feeding tube to be inserted post-intubation. This bin will be brought into the AIIR for every intubation.
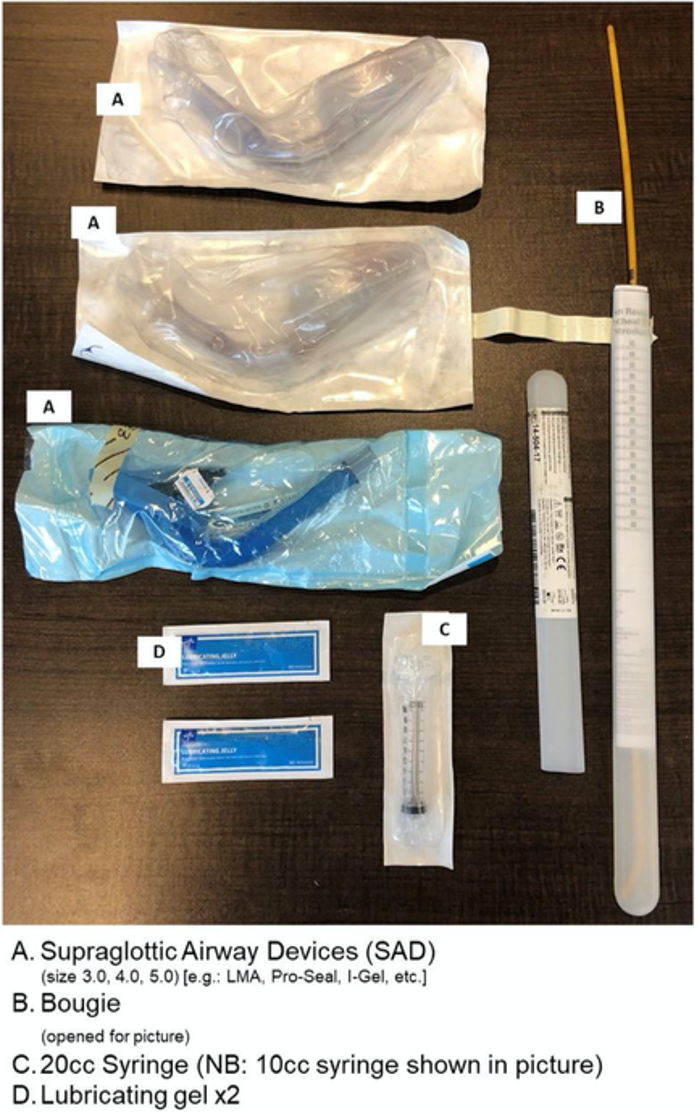
Bin #2: Rescue Plan A – iGel LMA’s and a Bougie. To be kept in the AIIR anteroom.
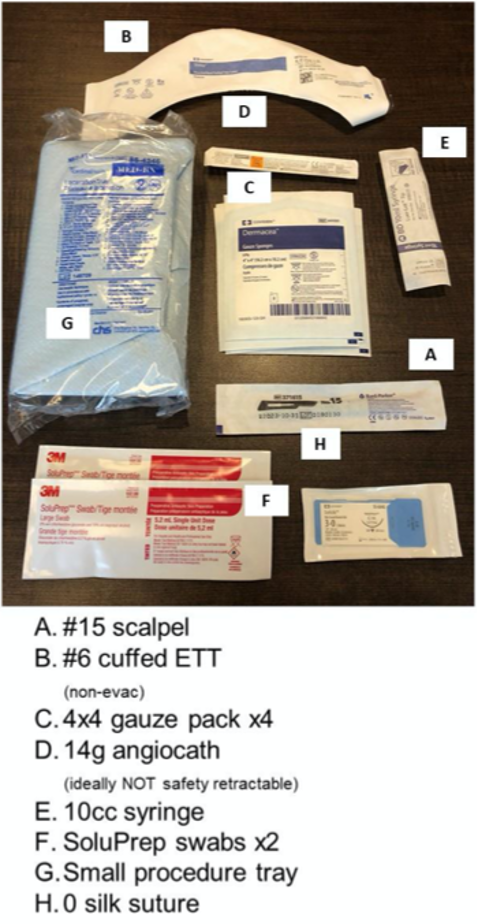
Bin #3: Can’t intubate, Can’t oxygenate: Surgical cric equipment. To be kept clean, outside the AIIR anteroom.
“Grab and go” medication bundles:
- IV start bundle: tourniquet, 18 & 20G angiocath, chlorhexidine swab, opsite, tape, gauze, blood vials, 1L normal saline, IV tubing
- RSI bundle: Propofol 200mg (1 vial), Rocuronium 150mg (3 vials).
Ketamine 100mg stored separately in ADC. - Phenylephrine bundle
- Norepinephrine bundle
- Post-intubation sedation bundle
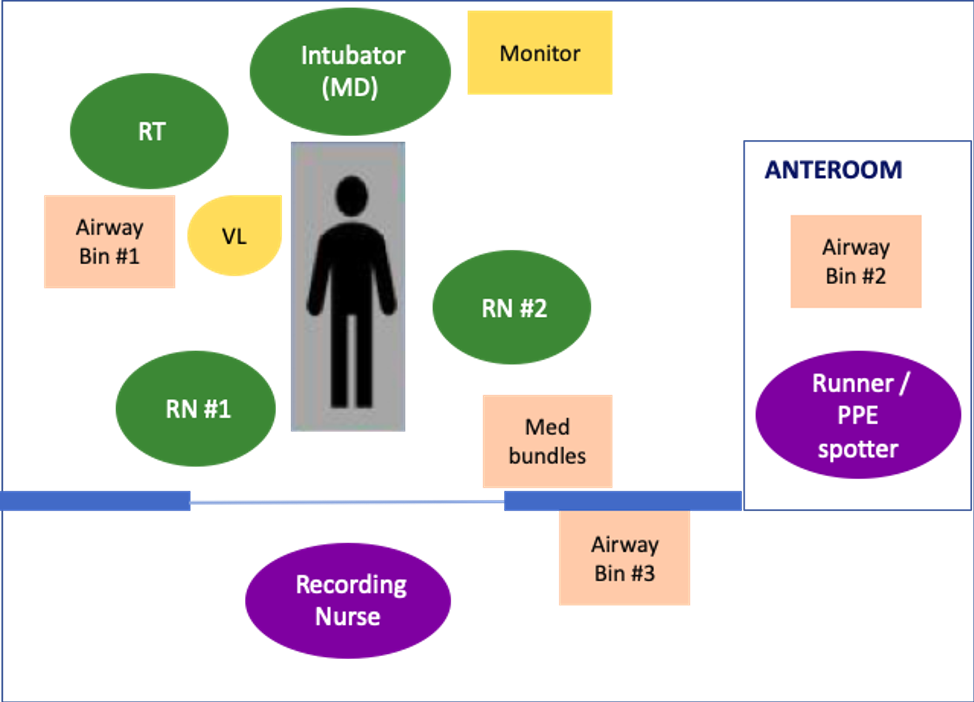
Team Organization for intubation
- Limit the number of healthcare workers in the room.
- Discuss the airway plan and use a cognitive aid/airway checklist
- The most skilled practitioner (or delegate) should perform the procedure to limit attempts.
- An expert assistant, such as a respiratory therapist, anesthesia assistant, or a healthcare provider familiar with equipment and drugs, should also be present.
- A second assistant should have PPE on and remain ‘clean’ in order to pass additional unanticipated equipment and assist.
- A ‘runner’ role (second MD, resident, nurse, etc) should be assigned outside the room to provide additional equipment or drugs to the ‘clean’ assist in PPE.
Recommended operating procedures for intubation
Prepare
- Confirm Patient Goals of Care and Appropriateness align with intubation, prior to proceeding.
- Airway management must be performed in a Negative pressure isolation room.
- Mandatory enhanced PPE (N95 respirator / “Airborne + Droplet + Contact” precautions) for all team members. Fit testing must be up to date.
- Most skilled intubator (no junior residents) should perform the procedure.
- Consider challenging airway anatomy and notify anesthesia early if help needed.
- Videolaryngoscopy is the preferred first-line modality.
- Perform pre-intubation checklist.
- Confirm the presence of backup modalities including “Rescue Airway Pack” (cric & LMA).
Preoxygenate
- Anticipate rapid desaturation due to reduced oxygen reserve and increased demand.
- Avoid aerosol-generating techniques: no NIPPV, no HFNC.
- Bed-up-head-elevated positioning.
- Provide 100% O2 for 3-5 minutes or 8 vital capacity breaths.
- Preferably via Ambubag with HME (“heat-moisture exchanger”, aka. Hydrophobic, HEPA) filter interposed with mask.
These are the “standard” vent filters stocked in the ED. - A limited number of HiOx masks are also available for consideration.
- Avoid providing assisted respirations.
- Two-handed BVM only if absolutely needed.
- Preferably via Ambubag with HME (“heat-moisture exchanger”, aka. Hydrophobic, HEPA) filter interposed with mask.
- PEEP (positive end expiratory pressure) may be applied by addition of a PEEP valve and effective two-hand mask seal.
- If manual bagging is required, consider use of supraglottic device (LMA).
Pretreatment
- Adequate hemodynamic resuscitation if time permits. Consider fluid-sparing approach due to concerns for third-spacing.
- Consider having vasopressors prepared +/- running (norepinephrine 5-35 mcg/min) prior to induction – particularly for patients with hypotension, signs of impaired perfusion, or elevated shock index (HR÷sBP > 1).
Paralysis with induction
- Nearly all patients should receive full RSI with neuromuscular blockade to optimize chance of first-pass success.
- Rocuronium @1.5 mg/kg may be favoured to prevent bucking/coughing post-intubation.
Intubation
- Should be preferentially performed with Videolaryngoscopy (Glidescope).
- Use a styletted EVAC ETT (suggest size 7.5 standard).
- If manual ventilation is required, small tidal volumes/permissive hypercapnea is recommended.
- Failed attempt: rescue with LMA placement, call for help, optimize technique.
- In the setting of can’t intubate/can’t oxygenate situations, perform scalpel-bougie cricothyrotomy.
- Ensure HME filter interposed between ETT and circuit.
- Post-intubation ventilation should only be initiated once balloon has been inflated.
- ETT should be confirmed with Colorimetric or Continuous Waveform End-Tidal CO2. Avoid auscultation.
- Avoid disconnects. Check all ETT and circuit connections. Avoid in-line suction unless sealed unit.
Post intubation care
- Insert 12Fr Kao (Dobhoff) nasogastric tube.
- Clamp ETT for any disconnection from the circuit such as transfers, or use Flusso valve.
- Transfer of patient onto a separate ventilator should be performed with all precautions listed above plus clamping of the endotracheal tube.
- Initiation of sedation and analgesia
- Initiate mechanical ventilation using Lung Protective strategy


Hey George, can you tell me where you got your bins for intubation?
Thanks!
Rob Daloise, MD, CCFP-EM
Assistant Clinical Professor
Emergency Medicine
UofA