

Here we present part two on our series on hypothermia. For more on the assessment, resuscitation, and management of the hypothermic patient, see part one.
Prognostication of cardiac arrest in hypothermia
Indicators of cardiac arrest before cooling (Brown 2012)
- Major trauma
- Witnessed normothermic arrest
- Avalanche burial <35 min
Patients with primary hypothermia and cardiac stability who have been treated with active external and minimally invasive rewarming have a rate of neurologically intact survival of approximately 100%. (Brown, 2012, Kornberger 1999)
Saczkowski (2018) did a meta-analysis of patients who underwent ECLS, and identified features predictive of survival:
- Predictive of poor outcome: asphyxia, elevated potassium, rewarming rate, gender (male)
- NOT predictive: age, CPR duration, pH, lactate, initial rhythm, mechanism, initial core temperature
- Asphyxiation
- In the Saczkowski (2018) data, 279 of 658 (42.4%) patients who underwent ECLS likely had asphyxiation as a cause of their cardiac arrest. Of the patients with completed follow up, 24 of 265 (12.8%) survived with good neurologic outcome.
In the subset of patients with presumed asphyxia, only 12.8% survived with good neurologic outcome
- Potassium
- Among the most reliable prognostic measures
- Potassium is released due to traumatic and hypoxic cell death, and is interpreted as a marker of hypoxia prior to cooling
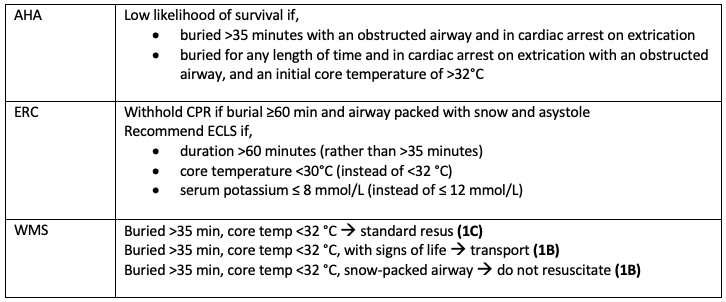
- Recommended cut-off value is 12 mmol/L (AHA, ERC)
- Recommended cut-off value in avalanche victims is 8 mmol/L (AHA, ERC, WMS)
- Highest K successfully resuscitated:
- 11.8 mmol/L in a 31-month-old child (Dobson 1996)
- 9.5 mmol per liter in a 13-year-old child (von SegesserLK 1991)
- 7.9 mmol/L in a 34-year-old (Farstad 2001)
- 6.4 mmol/L in an adult in an avalanche (Locher 1996)
- Sazckowski 2018 data showed an roughly dose-dependent response:
- <5: 35%–85% good neurologic outcome
- 5-10: 10%–50% good neurologic outcome
- >10: 0%–20% survival
- >12: 0% survival
- Temperature
- Classifying severity is useful
- Absolute temp is not very predictive in outcomes
- The lowest reported core body temperatures in patients with full neurologic recovery are slightly less than 13.7°C (57°F) in a case of accidental hypothermia. (Gilbert 2000)
- Resuscitation time
- is not predictive of survival
- Longest time in a case report: 31 year old man, rock climbing when he became trapped on a rock face with cold running water. Core temperature was 26.0 °C. He underwent CPR with a LUCAS device for 3 hours and 42 minutes, then ECMO for 5 hours, for a total of 8 hours and 42 minutes.
- 65 year old, found on a snow-covered riverbank. No vital signs, in asystole. Core temperature initially 28 °C rectal, lowest 20.8 °C. Underwent CPR (4 h 48 m) and ECLS (3 h 52 m), for a total of 8 h 40 min. (Meyer 2014)
- Longest persistent VF in a case report: 25 year old, buried by an avalanche. After extrication, had witnessed VF arrest at core temp 17.0°C. Had 3 unsuccessful shocks. Underwent ECMO rewarming for 6 h, 45 min, with successful 4th shock at 24.8 °C. Full neurologic recovery. (Kosinski 2016)
- Most number of shocks in a case report: 42 year old, found outdoors, no vital signs. Bystander CPR started. On EMS arrival was in VF. Continued CPR with repeated shocks. In hospital temp 22°C, EtOH 90. CPR continued, with a total of 38 shocks delivered. Eventually underwent ECLS rewarming after 130 min CPR. Successful shock was at 30°C. Full neurologic recovery. (Nordberg 2014)
- Chest compressions pattern/quality
- What we typically rely on is not reliable
- Prolonged period of no compressions
- Longest case of no CPR in a case repor: 42 year old, found in crevasse buried under 7m of snow. No vital signs. CPR started 70 minutes later, after arrival to the hospital. Asystolic on arrival, with core temp 19 °C. Underwent ECLS. Full recovery. (Althaus 1982)
- Intermittent compressions
- Case report of alternating CPR 1min on, 1 min off, with good neurologic recovery. 57 year old, missing in Grenoble in French Alps at 2000m altitude, witnessed cardiac arrest on rescue. Transported on foot to EMS vehicle 1.1 km away. Underwent 1 min CPR alternating with 1 min walking for 25 min, and a total of 5 h CPR before ECLS rewarming. Full recovery. (Boue 2014)
- Trauma
- Standard trauma TOR criteria still apply
- BUT polytrauma is NOT an absolute contraindication to ECLS
- Concern with heparinization required for CPB/ECMO
- Case report of survival with ECMO despite polytrauma – Male, found down on street by police, unknown circumstances of injury. Noted “extremely untidy”. Core temp 28. Trauma CT findings of pericerebral hematoma, signs of previously right craniotomy, multiple right-sided rib fractures, intraperitoneal fluid, and likely traumatic pancreatitis. Underwent warming and ECMO. Full neurologic recovery. (Darocha 2015)
- Drowning
- If history suggests immersion in cold water (ie. able to breath) prior to submersion, cooling likely occurred prior to hypoxia and neurologic outcomes are better
- The longest submersion times reported are 83min (7 year old child) and 66min (25 year old). Both underwent ECLS, and both had full recoveries. (Bolter 1988, Romlin 2015)
- If history suggests submersion first, then asphyxiation is likely to cause of arrest, and prognosis is grim.
- Avalanche
- Death from asphyxia is much more common than hypothermia
- Poor prognostic signs
- Unwitnessed arrest with asystole predicts very poor survival chances, as hypoxia likely preceded cooling. Chances are better with VF or PEA. (Paal 2016)
- Airway packed with snow
- Burial time < 35 minutes, because this is insufficient time for cooling
- Temperature >32°C and in cardiac arrest on extrication
- Highest potassium in an avalanche victim was 6.4 mmol/L. (Locher 1996)
Pre-Hospital Considerations
- Most EMS systems do not make use of core temperature measurements or have low-sensing temperature probes. It is typically not feasible.
- Swiss classification was developed to allow rescuers to have clinical data to aid in identifying severe hypothermia.
- Must check for pulse for at least 60 seconds
- If no signs of life, CPR should be started
ECMO bypass protocols?
- Challenging to implement due to limits of EMS capabilities to measure core temperature
- Generally relies on an order from EMS base hospital (“patch call”) for redirect based on a case-by-case scenario
- Those with hemodynamic instability or in cardiac arrest should be transported to a center capable of providing CPB or ECMO.
When is prehospital TOR appropriate?
- If risk to the responder is unacceptable
- Obvious signs of irreversible death: decapitation, truncal transection, decomposition of the whole body, and a chest wall that is not compressible
- If the chest is too stiff to provide compressions
Use of mechanical CPR in hypothermia
- Hypothermia can cause stiffness of the chest wall, making ventilations and chest compressions difficult. Consider the use of mechanical chest compression devices. (ERC)
- Putzer 2013 – prospective RCT using manikins that compared LUCAS device to manual cardiopulmonary resuscitation during helicopter rescue. Showed less hands-off time, but longer time to first defibrillation. Showed the feasibility of prolonged CPR with the LUCAS.
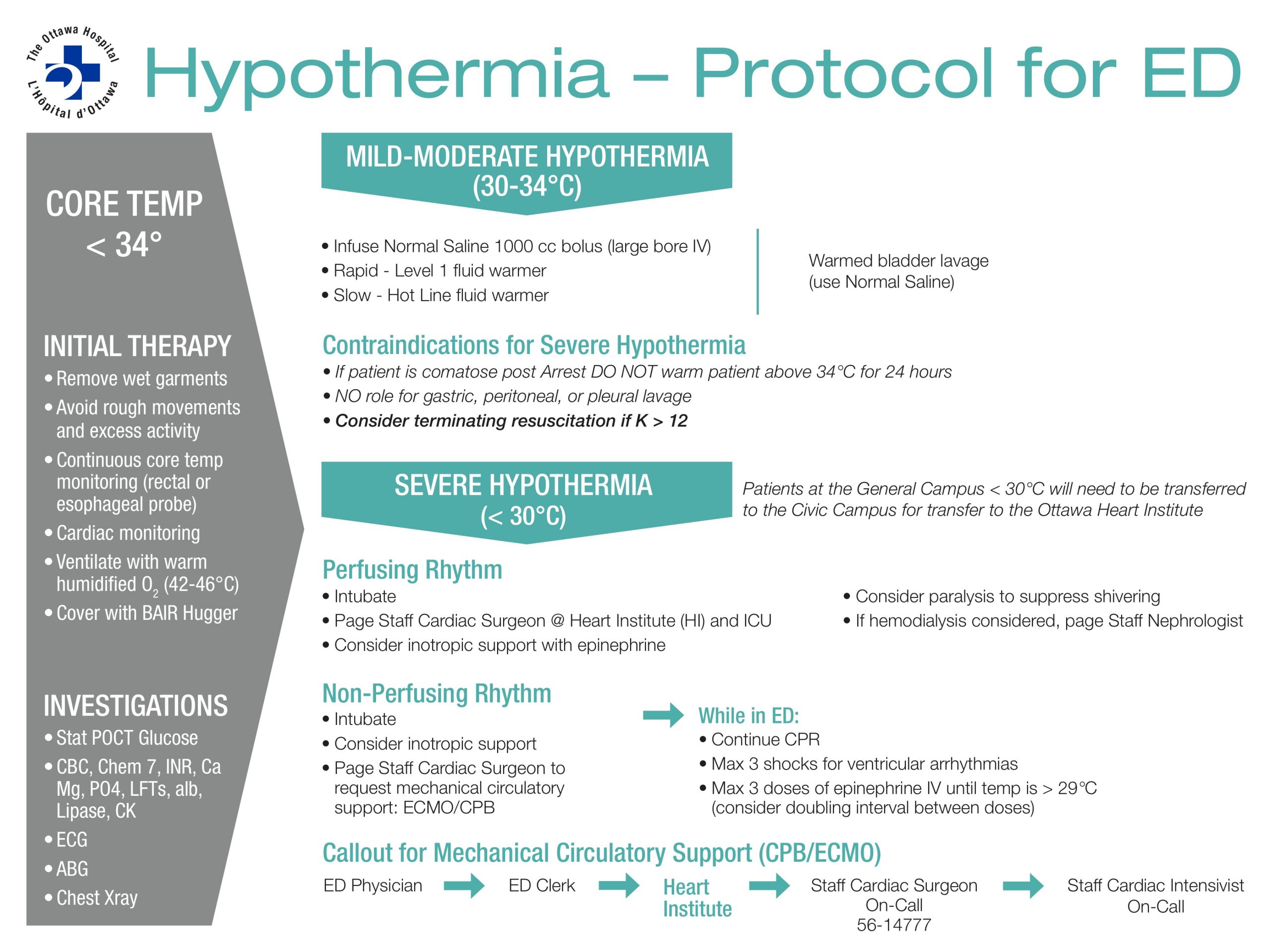
Sample Hypothermia Protocol
References
- Baumgartner EA, Belson M, Rubin C, Patel M. Hypothermia and other cold-related morbidity emergency department visits: United States, 1995-2004. Wilderness Environ Med 2008;19:233-7.
- Silfvast T, Pettilä V. Outcome from severe accidental hypothermia in Southern Finland — a 10-year review. Resuscitation 2003;59:285-90.
- Danzl DF. Accidental hypothermia. In: Auerbach PS, ed. Wilderness medicine. 6th ed. Philadelphia: Mosby, 2012:116-42.
- Toronto Public Health. Health Impacts of Cold Weather. Technical Report. June 2014
- Bristow GK, Giesbrecht GG. Contribution of exercise and shivering to recovery from induced hypothermia (31.2 degrees C) in one subject. Aviat Space Environ Med 1988;59(6):549–52.
- Tikuisis P, Giesbrecht GG. Prediction of shivering heat production from core and mean skin temperatures. Eur J Appl Physiol Occup Physiol 1999;79(3):221–9.
- Wood S. Interactions between hypoxia and hypothermia. Annu Rev Physiol1991;53:71–85.
- Giesbrecht GG, Bristow GK. A second postcooling afterdrop: more evidence for a convective mechanism. J Appl Physiol 1992;73(4):1253–8.
- Romet TT. Mechanism of afterdrop after cold water immersion. J Appl Physiol 1988;65(4):1535–8.
- Vassallo S, Kathleen A. Chapter 15: Thermoregulatory principles, in Goldfrank’s Toxicologic Emergencies, Nelson et al., 9th Ed, 2011, The McGraw-Hill Companies.
- Truhlar A, Deakin CD, Soar J, et al. European resuscitation council guidelines for resuscitation 2015: section 4. Cardiac arrest in special circumstances. Resuscitation 2015;95:148–201.
- Zafren K, Giesbrecht GG, Danzl DF, et al. Wilderness Medical Society practice guidelines for the out-of-hospital evaluation and treatment of accidental hypothermia: 2014 update. Wilderness Environ Med 2014;25(4 Suppl):S66–85.
- Vanden Hoek TL, Morrison LJ, Shuster M, et al. Part 12: cardiac arrest in special situations: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2010;122(18 Suppl 3):S829–61.
- Plaisier BR. Thoracic lavage in accidental hypothermia with cardiac arrest — report of a case and review of the literature. Resuscitation 2005;66:99-104.
- Taylor EE, Carroll JP, Lovitt MA, et al. Active intravascular rewarming for hypothermia associated with traumatic injury: early experience with a new technique. Proc (Bayl Univ Med Cent) 2008;21:120-6.
- Saczkowski et al. (2018) Prediction and risk stratification of survival in accidental hypothermia requiring extracorporeal life support: An individual patient data metaanalysis. Resuscitation 127 (2018) 51–57.
- Ruttmann E, Weissenbacher A, Ulmer H, et al. Prolonged extracorporeal membrane oxygenation-assisted support provides improved survival in hypothermic patients with cardiocirculatory arrest. J Thorac Cardiovasc Surg 2007;134:594- 600.
- Lexow K. Severe accidental hypothermia: survival after 6 hours 30 minutes of cardiopulmonary resuscitation. Arctic Med Res 1991;50:Suppl 6:112-4.
- Rankin AC, Rae AP. Cardiac arrhythmias during rewarming of patients with accidental hypothermia. Br Med J (Clin Res Ed) 1984;289(6449):874–7.
- Ujhelyi MR, Sims JJ, Dubin SA, Vender J, Miller AW. Defibrillation energy requirements and electrical heterogeneity during total body hypothermia. CritCare Med 2001;29:1006–11.
- Kornberger E, Schwarz B, Lindner KH, Mair P. Forced air surface rewarming in patients with severe accidental hypothermia. Resuscitation 1999;41:105-11.
- Dobson JA, BurgessJJ. Resuscitation of severe hypothermia by extracorporeal rewarming in a child. J Trauma. 1996;40:483–485.
- von SegesserLK, GarciaE, TurinaM. Perfusion without systemic heparinization for rewarming in accidental hypothermia. Ann ThoracSurg. 1991;52:560–561.
- Farstad M, AndersenKS, KollerME, GrongK, Segadal L, HusbyP. Rewarming from accidental hypothermia by extracorporeal circulation. A retrospective study. Eur J Cardiothorac Surg. 2001;20:58–64.
- Locher T, Walpoth B. Differential diagnosis of circulatory failure in hypothermic hypothermic avalanche victims: retrospective analysis of 32 avalanche accidents. Praxis 1996;85:1275-82. (In German.)
- Gilbert M, Busund R, Skagseth A, Nilsen PÅ, Solbø JP. Resuscitation from accidental hypothermia of 13.7 degrees C with circulatory arrest. Lancet 2000;355: 375-6.
- Darocha T, Kosin´ski S, Jarosz A, Drwila R. Extracorporeal Rewarming From Accidental Hypothermia of
- Patient With Suspected Trauma. Medicine, Volume 94, Number 27, July 2015
- Brown D, Brugger H, Boyd J, Paal P. Accidental Hypothermia, 2012, New England Journal of Emergency Medicine, 367;20.
- Forti A, Brugnaro P, Rauch S, Crucitti M, Brugger H, Cipollotti G, Strapazzon G. Hypothermic Cardiac Arrest With Full Neurologic Recovery After Approximately Nine Hours of Cardiopulmonary Resuscitation: Management and Possible Complications. Annals of Emergency Medicine Volume 73, no. 1 : January 2019.
- Paal et al. Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine (2016) 24:111 DOI 10.1186/s13049-016-0303-7
- Meyer M, Pelurson N, Khabiri E, Siegenthaler N, Walpoth BH. Sequela-free long-term survival of a 65-year-old woman after 8 h and 40 min of cardiac arrest from deep accidental hypothermia. J Thorac Cardiovasc Surg. 2014;147(1):e1–2. doi:10.1016/j.jtcvs.2013.08.085.
- Nordberg P, Ivert T, Dalen M, Forsberg S, Hedman A. Surviving two hours of ventricular fibrillation in accidental hypothermia. Prehosp Emerg Care. 2014; 18(3):446–9. doi:10.3109/10903127.2014.891066
- Kosinski S, Darocha T, Jarosz A, Migiel L, Zelias A, Marcinkowski W, et al. The longest persisting ventricular fibrillation with an excellent outcome – 6 h 45min cardiac arrest. Resuscitation. 2016;105:e21–2. doi:10.1016/j. 2016.05.022.
- Althaus U, Aeberhard P, Schüpbach P, Nachbur BH, Mühlemann W. Management of profound accidental hypothermia with cardiorespiratory arrest. Ann Surg. 1982;195(4):492–5.
- Boue Y, Payen JF, Torres JP, Blancher M, Bouzat P. Full neurologic recovery after prolonged avalanche burial and cardiac arrest. High Alt Med Biol. 2014;15(4):522–3. doi:10.1089/ham.2014.1082.
- Putzer G, Braun P, Zimmermann A, et al. LUCAS compared to manual cardiopulmonary resuscitation is more effective during helicopter rescue – a prospective, randomized, cross-over manikin study. Am J Emerg Med 2013;31:384–9.51
- Mazur P, Kosiński S, Podsiadło P, Jarosz A, Przybylski R, Litiwnowicz R, Piątek J, Konstanty-Kalandyk J, Gałązkowski R, Darocha T. Extracorporeal membrane oxygenation for accidental deep hypothermia—current challenges and future perspectives. Ann Cardiothorac Surg 2019;8(1):137-142. doi: 10.21037/acs.2018.10.12
- Bolte RG, Black PG, Bowers RS, Thorne JK, Corneli HM. The use of extracorporeal rewarming in a child submerged for 66 minutes. JAMA 1988;260:377-9.
- Romlin BS, Winberg H, Janson M, Nilsson B, Björk K, Jeppsson A, et al. Excellent outcome With Extracorporeal Membrane Oxygenation after accidental profound hypothermia (13.8° C) and drowning. Crit Care Med. 2015;43:e521–5. doi:10.1097/CCM.0000000000001283.
- Locher T. Walpoth BH: [Differential diagnosis of circulatory failure in hypothermic avalanche victims: retrospective analysis of 32 avalanche accidents]. Praxis (Bern 1994). 1996;85(41):1275–82.

