
In the past 5-10 years we have seen a significant increase in mental health-related complaints in the Emergency Department (ED), and during COVID this is especially noticeable. Historically, we’ve classically been taught to focus on performing safety assessments, and as a result, we don’t often end up doing anything helpful for these patients, or we end up consulting psychiatry for patients that they subsequently send home – and I think we can do better.
In this post, we are going to focus primarily on engaging patients with depression, anxiety, and suicidality. Sure, talking to these patients can be time-consuming, but you’ll find that when you engage these patients, you can make a significant impact during your assessment, and this can help to mitigate some of the negative reactions/counter-transference one often feels when grabbing these patient charts (I don’t think it is a huge secret that people tend to cherry-pick around these complaints).
In this post, we are NOT going to discuss medications. The evidence for antidepressants is questionable at best. There are thousands of studies looking at the effectiveness of antidepressants, but only a few robust meta-analysis. The problem with the data in these studies is that the trials are often heavily biased, and most negative trials are not published. The reality is, when you take a serious look at studies on SSRIs and other medications to treat depression – they are likely not much better than placebo. It appears that they may have a role in minimizing anxiety disorders, but for depression itself, it is likely low yield in most patients. I think intuitively, you know this to be true, as many of the patients you see with mood disorder related complaints are already on (or have been on many different types) these medications.
Panic Attacks
Panic attacks are relatively common in patients with anxiety-related disorders. We’ve all been in that scenario where a patient has either a) a panic attack in front of you, or b) tells you about their fear of another one happening.
In these scenarios, physicians will often start prescribing benzodiazepines, but as you all know, that is a dangerous road to start traveling down. Some evidence-based suggestions instead:
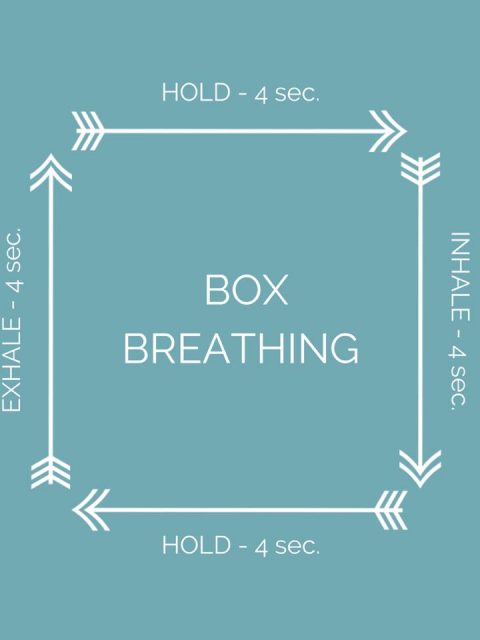
- Box breathing: have the patient inhale for 4 seconds, hold for 4 seconds, out for 4, hold for 4. Another suggestion here is to breathe in and out of a paper bag (not plastic!)
- Grounding exercise: Tell a story with the objects you can see around you
- Symptom focus: Focus on the symptoms and think about how to describe them in great detail to a physician (i.e.: exactly which fingers are numb, describe the palpitations experienced, etc).
- Guided meditation: Just search ‘guided meditation’ on any streaming platform/youtube/google – a calm voice and calming music with deep breathing can help anchor the patient and help to alleviate their panic attack. While this may seem silly to do in the ED, it is non-invasive, and highly effective.
It is important to remind these patients that there are two aspects to treating their anxiety/panic attacks – one is what to do when they occur. The second aspect is to try and uncover why they’re having them in the first place – and directing them to psychology/counseling as appropriate. Sometimes, you may not identify an underlying trigger, but it is important to plant this seed in the patient’s mind.
Anxiety and Depression
When talking about anxiety, it is important to remember that it does have an evolutionary benefit. It comes from the fight or flight response – and in modern days it isn’t being stimulated as it once was. The fight or flight response was helpful 5000 years ago when we were running away from lions and tigers. it is the result of ‘I am hungry, I need to hunt something to eat’, and is coded within our DNA. Now, you can get food delivered right to your door without having to stop watching Netflix. People need to appreciate this message in order to understand and get a better grasp of their anxiety.
When it is clear that someone’s presentation is due to anxiety, or they have concerns related to their mood; you need to figure out why today/what specifically, and to be fair, sometimes there is no answer, but if you can delve into what is driving their mood symptoms, this will really help. If you’re able to identify a specific problem that has caused a deterioration in their symptoms:
- You can attempt to help problem solve
- Find coping strategies to help deal with it
- Coach the patient to use their own established coping techniques to address the issue(s)
Some helpful questions:
- “What do you think is driving your anxiety?”
- “Is there anything you a particularly stressed about right now?”
- “How do you cope with stress and difficult things going on in your life?”
Remember, that with mood disorders – these people deal with their symptoms day in and day out, but they don’t normally come to the ED, so isolating what is different today is very helpful, just like seeing any patient with a chronic pain disorder.
Substance misuse
You have to ask about substance misuse, especially pot.
15-20% of Canadians are using Cannabis, and up to 25% in the 24-34 age range. I also suspect (no data is available) that these numbers are higher during the current COVID-19 Pandemic. It is also important to remember that cannabis use is twice as high in those with mental health disorders, and is often a result of patients self-medicating. Some key things to know about cannabis from the literature (1):
- Two forms of marijuana; CBD and THC
- THC binds to cannabinoid receptors in the brain and causes a high or sense of euphoria
- CBD binds very weakly to CNS cannabinoid receptors and is non-psychoactive
- THC is the most likely to increase anxiety. Some literature suggests at lower doses it may help lessen anxiety, but it is much more likely to result in worsening anxiety
- Most CBD based literature suggests it does help to lessen anxiety (3) – but this is acutely only. Long term data suggests this benefit does not continue forward, which makes sense – no matter what you’re self-medicating with, if you don’t take care of the underlying issues/address them – it’ll continue to cause psychological distress.

From a mental health perspective – it is important to remind patients that the things that are causing them distress, they need to find ways to address or cope with it. For them, pot is an escape – but you can’t run from your problems forever, and that their anxiety is their body’s way of telling them they need to find ways to cope.
Everyone needs homework
As the fight or flight response drives a lot of anxiety, it becomes important to find ways to ‘feed’ this response, and so people need actionable items, or homework.
I will often write a prescription for patients, and document the importance of evidence-based interventions:
- 30-60 minutes of exercise daily
- Exercise certainly helps with mood symptoms – the hard part is overcoming the depression to do the exercise. This is why a prescription may be valuable; the patient probably won’t want to do it, but they need to. They wake up in the morning, feel awful, and don’t want to do anything. They can’t envision how some exercise will help, but it requires some coaching and reinforcement because exercise helps.
- Do something productive
- Productivity is important; when people are engaged it helps to provide meaning, which will help with mood symptoms. It doesn’t matter what activity is being performed – work, organizing, cleaning, even just taking a shower and putting on pants in the morning.
- Make ‘to-do lists’
- ‘To do lists’ help to lessen anxiety symptoms, especially when obsessive-compuslive personality traits are present. Ideally, this should be ‘unboxed’ as much as possible, i.e.: instead of writing down ‘do laundry’, write ‘wash clothes, dry clothes, fold’ – each ‘checkbox’ helps to minimize symptoms.
- Have a hobby? Do it. If not – find one
- Everyone has to do something they enjoy. A recently published study demonstrated that engaging in a hobby (pre-existing or a new one) results in a 30% decrease in depressive symptoms and increased recovery from that depressive episode (OR 2.72 95% CI 2.09-3.53).
- Do something social every day
- One of the initial symptoms of depression is withdrawing from social contacts/supports, try to encourage people to continue doing something social (even if it is socially distant nowadays).
Patients will often say that they are trying to do these things, nr know that they need to do them – but lack the motivation to do so. The analogy I will often use is that when a patient has cancer – they don’t want to do chemotherapy, it sucks. But they do it, because it can help them get better. With mood disorders, you have to think of them as disease entities that will improve with these interventions.
Suicidality
For patients who are specifically vocalizing suicidality, a few high yield questions to consider:
- “On a scale of 1-10, how suicidal do you feel today? Where do you sit on a normal day?”
- One thing commonly expressed by patients is that they feel suicidal most days, but that today is worse
- “Based on that, you feel suicidal every day… but normally, you do not present to the ED, and you’re able to cope at home. What is different about today?”
- You want to attempt to isolate the factor that is increasing suicidality today (note: sometimes there is no acute variable, but more often than not you will uncover something).
- “If it weren’t for that ‘thing’ making things worse today, would you be here today?”
- This doesn’t take an expert, but remember to focus is on providing the patient with (or reminding them of existing) coping strategies to attempt to deal with these problems effectively.
- Documentation:
- “Based on my assessment I have no acute safety concerns, however, due to the patient’s history of BPD, they are at chronically elevated suicide risk due to non-modifiable risk factors, over which I have no control”.
References
- Stoner S. Effects of Marijuana on Mental health: Aniety disorders. Alcohol and Drug abuse Institute. Univ. of Washington. June 2017
- Fancourt D, Opher S, de Oliveira C: Fixed-Effects Analyses of Time-Varying Associations between Hobbies and Depression in a Longitudinal Cohort Study: Support for Social Prescribing? Psychother Psychosom 2020;89:111-113. doi: 10.1159/000503571
- Stoner S. Effects of Marijuana on Mental health: Aniety disorders. Alcohol and Drug abuse Institute. Univ. of Washington. June 2017

This is a great post. Physicians tend to rely on medication, which is not the most beneficial. These are good tips to have. Maybe an infographic would be useful to keep in the department
Hi,
I have read your article and found it very interesting. Thanks for the write-up.