

Assisted reproductive technology (ART) is an evolving field with many therapies that have a common goal: to maximize the chance of pregnancy while minimizing the risk of multiple gestations. As the Canadian infertility rate approaches 15%, the use of ART is steadily increasing (1). In fact, 1-4% of all newborns in industrialized nations are conceived with assisted reproductive technology (2). Thanks to therapeutic advances, complication rates continue to decrease. Nevertheless, the risks are non-negligible, particularly for ovarian hyperstimulation syndrome. It is imperative than we understand how ART works and that we be prepared to recognize and manage any potentially serious complications presenting to our emergency departments.
Assisted Reproductive Technology 101
Assisted Reproductive Technology has come a long way. The turn of the 20th century saw the development of artificial insemination; by 1978, the first child conceived via in vitro fertilization (IVF) was born (3).
For patients suffering from ovulatory dysfunction, letrozole (and more historically, clomiphene citrate) can be prescribed to induce ovulation. Common side effects include headache, visual disturbances, abdominal pain, nausea and multiple pregnancies.
Controlled ovarian stimulation is offered to select patients with unexplained or mild male-factor infertility. Gonadotropins (e.g. Gonal-F) are injected subcutaneously early in the menstrual cycle to promote the growth and maturation of multiple oocytes. Patients are closely monitored during this process, which is followed by either timed intercourse or intrauterine insemination. Common side effects include headache, abdominal pain, nausea, and injection-site reactions.
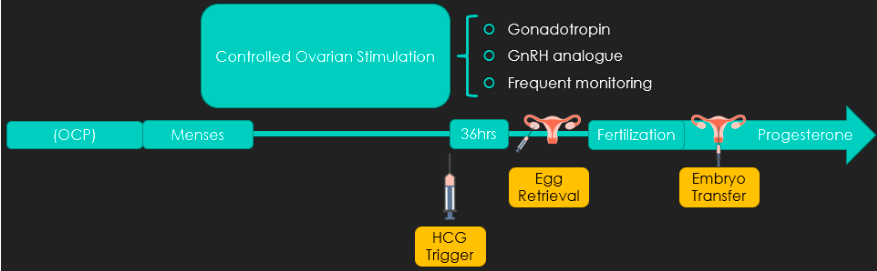
IVF begins with menstrual cycle regulation with a combined or progesterone-only oral contraceptive pill. Upon menses, controlled ovarian stimulation is initiated with the addition of a GnRH analogue (e.g. Cetrotide) to prevent the LH surge and subsequent early ovulation. Guided by ultrasound observation of the patient’s stimulated follicles, ovulation is then triggered. This is most commonly achieved with an injection of HCG, which can result in a positive serum βHCG for up to 14 days! 36hrs after triggering ovulation, eggs are retrieved via ultrasound-guided transvaginal needle aspiration, which are then fertilized in the laboratory. Resulting embryos are transferred into the uterus 3-6 days later and patients take progesterone supplements to support an early pregnancy. Patients undergoing IVF may suffer from the side effects of controlled ovarian stimulation and are at particularly high risk for ovarian hyperstimulation syndrome, among other complications reviewed below.
Take-Home Points
- There are many indications for, and varieties of, ART
- Most are well tolerated
- A positive βHCG may not mean that your patient is pregnant
Recognizing & resuscitating ovarian hyperstimulation syndrome
Ovarian hyperstimulation syndrome (OHSS) occurs almost exclusively in patients undergoing ART. Up to 36% of IVF patients experience mild to moderate OHSS; severe OHSS is less common (0.1-2%) (4). Risk factors include young maternal age (<30yrs), PCOS, prior OHSS, early pregnancy, and the use of HCG to trigger ovulation (5). It appears to be mediated by increased vascular permeability and presents either early (3-7 days post-trigger) or late (10-17 days post-trigger), with the latter usually being more severe.
OHSS presents as a spectrum of disease, ranging from abdominal bloating to diffuse extracellular shift and volume contraction, leading to hemoconcentration, AKI, and thrombophilia (6). While it remains a clinical diagnosis, pelvic ultrasound is indicated for any ART patient presenting with abdominal pain or distension; it may identify ovarian enlargement (>5-8cm), multiple follicles and intraabdominal free fluid (3).
Mild to moderate OHSS is treated conservatively, with analgesics, antiemetics, close follow-up and consideration for thromboprophylaxis. Severe OHSS can require crystalloids to support perfusion and culdocentesis to drain large-volume ascites causing respiratory impairment or abdominal compartment syndrome. Thoracentesis has been described for symptomatic large pleural effusions. Thromboprophylaxis is indicated. In all cases of confirmed or suspected OHSS, the patient’s fertility specialist should be contacted to advise management and to arrange close follow-up (6).
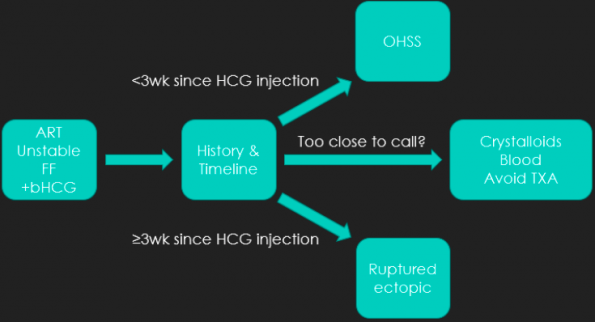
Notably, patients with severe OHSS may present with abdominal pain, intraabdominal free fluid and a non-definitive intrauterine pregnancy on POCUS, with a positive βHCG; similar to ectopic pregnancy. These two entities can fortunately be distinguished on history; those presenting <3 weeks since HCG trigger are likely OHSS while those presenting ≥3 weeks post-trigger would be at higher risk of a ruptured ectopic pregnancy. If you are uncertain, resuscitating with crystalloids while calling for blood and liaising with OB-GYN and fertility specialists would be the best course of action. I would avoid TXA in this instance unless an ectopic is diagnosed or is highly suspected in later-presenting patients (>3 weeks post-trigger).
Take-Home Points
- OHSS is common
- It’s a spectrum of disease
- A good history can distinguish severe OHSS from ruptured ectopic
- Managed in tandem with fertility specialists
Ectopic & heterotopic pregnancy: what’s new?
While the historic ectopic pregnancy rate for patients undergoing ART was as high as 8.6%, it has since decreased to that of the general population at 1.6%, for patients undergoing a single embryo transfer (3,7). Similarly, the heterotopic pregnancy rate has decreased from ~1:100 to 1:1000 (8). Single embryo transfers are becoming the standard of care as advances in ART now allow for much higher success rates for each IVF cycle. Nevertheless, even with a single embryo transfer, patients are at high risk of a heterotopic pregnancy; the reasons for this are unclear but may be related to a coincident natural pregnancy (9).
Patients with a heterotopic pregnancy often present with first-trimester pelvic pain & bleeding. While the test of choice is pelvic ultrasound, up to 26% of such patients have a normal ultrasound initially (i.e. only an intrauterine pregnancy) (8).
Once diagnosed, these patients are often co-managed by fertility specialists and the on-call OB-GYN team. Therapeutic options for stable patients with heterotopic pregnancy include laparoscopic removal of the ectopic via salpingectomy or salpingostomy (10). While this is designed to preserve the viable intrauterine pregnancy, these patients are at higher risk for subsequent miscarriage.
Take home points:
- Heterotopic pregnancies are common, even in the era of single embryo transfers
- Patients presenting unstable, ≥3 weeks post-triggering of ovulation, have a ruptured ectopic pregnancy until proven otherwise
- Liaise with OB-GYN and fertility specialists
Other associated complications to keep on your radar
The incidence of ovarian torsion among ART patients is 0.2%, nearly double that of the general population (11). Meanwhile, up to 8% of patients with OHSS experience ovarian torsion (12). Classically, patients present with sudden onset nausea/vomiting and abdominal pain, and while pelvic ultrasound is the investigation of choice, it is not perfectly sensitive (13).
The oocyte retrieval process during IVF involves an ultrasound-guided transvaginal needle aspiration; as such, any nearby intraperitoneal structure may be injured. Severe injuries occur in up to 0.8% of patients, and include intraperitoneal bleeding requiring operative repair, pelvic infection, or anesthetic complications (14). More commonly, patients experience self-limited pelvic pain and/or vaginal bleeding (15).
Thromboembolic complications occur at higher frequency in ART patients than in both the general population and in pregnant patients. They may be either venous or arterial, and in patients afflicted with OHSS, up to 80% of thromboembolic events occur in the upper extremities (11). Low molecular weight heparin is indicated for treatment.
Take-home points
- Patients with a history of infertility or who are undergoing ART are at much higher risk of ovarian torsion
- Severe complications of the oocyte retrieval process are rare; consider intraperitoneal injuries and pelvic infections
- Thromboembolic complications occur at a greater frequency
Summary:
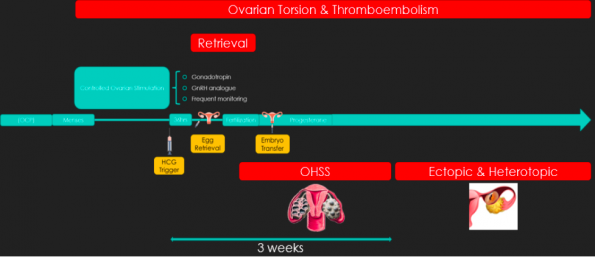
In summary, ART is a complicated process. Map each patient you see on the timeline below to better assess their risk for each complication. OHSS is common, and its infrequent severe variety can be distinguished from a ruptured ectopic pregnancy by a careful history. Ensure to involve the fertility specialists for each patient that you see presenting with a suspected complication of ART. Importantly, consider the patient’s perspective; they have worked so hard to become pregnant. It behooves us to empathetically and carefully communicate with them while assessing for complications.
References:
- Bushnik T, Cook JL, Yuzpe AA, Tough S, Collins J. Estimating the prevalence of infertility in Canada. Hum Reprod. 2012;27(3):738–46.
- Grafodatskaya D, Cytrynbaum C, Weksberg R. The health risks of ART. EMBO Rep. 2013 Feb;14(2):129–35.
- Hilbert SLM, Gunderson S. Complications of Assisted Reproductive Technology. Vol. 37, Emergency Medicine Clinics of North America. W.B. Saunders; 2019. p. 239–49.
- Timmons D, Montrief T, Koyfman A, Long B. Ovarian hyperstimulation syndrome: A review for emergency clinicians. Vol. 37, American Journal of Emergency Medicine. W.B. Saunders; 2019. p. 1577–84.
- Humaidan P, Nelson SM, Devroey P, Coddington CC, Schwartz LB, Gordon K, et al. Ovarian hyperstimulation syndrome: Reviewand new classification criteria for reporting in clinical trials. Vol. 31, Human Reproduction. Oxford University Press; 2016. p. 1997–2004.
- Shmorgun D, Claman P. No-268-The Diagnosis and Management of Ovarian Hyperstimulation Syndrome. J Obstet Gynaecol Canada. 2017 Nov 1;39(11):e479–86.
- Perkins KM, Boulet SL, Kissin DM, Jamieson DJ. Risk of ectopic pregnancy associated with assisted reproductive technology in the United States,2001-2011. Obstet Gynecol. 2015 Jan 1;125(1):70–8.
- Pontius E, Vieth JT. Complications in Early Pregnancy. Vol. 37, Emergency Medicine Clinics of North America. W.B. Saunders; 2019. p. 219–37.
- Lee JS, Cha H-H, Han AR, Lee SG, Seong WJ. Heterotopic pregnancy after a single embryo transfer. Obstet Gynecol Sci. 2016;59(4):316.
- Gao B, Cheng C, Pan Q, Johnson G, Qin X, Xu D. Laparoscopic strategy for heterotopic interstitial pregnancy following assisted reproductive techniques. J Soc Laparoendosc Surg. 2019 Apr 1;23(2).
- Santos-Ribeiro S, Mackens S, Racca A, Blockeel C. Towards complication-free assisted reproduction technology. Vol. 33, Best Practice and Research: Clinical Endocrinology and Metabolism. Bailliere Tindall Ltd; 2019. p. 9–19.
- Gorkemli2002_Article_AdnexalTorsionAfterGonadotroph.
- Dewey K, Wittrock C. Acute Pelvic Pain. Vol. 37, Emergency Medicine Clinics of North America. W.B. Saunders; 2019. p. 207–18.
- Levi-Setti PE, Cirillo F, Scolaro V, Morenghi E, Heilbron F, Girardello D, et al. Appraisal of clinical complications after 23,827 oocyte retrievals in a large assisted reproductive technology program. Fertil Steril. 2018 Jun 1;109(6):1038-1043.e1.
- Özaltin S, Kumbasar S, Savan K. Evaluation of complications developing during and after transvaginal ultrasound – Guided oocyte retrieval. Ginekol Pol. 2018;89(1):1–6.
