
Case: You are the emergency physician taking care of a 45-year-old male who has a background history of hypertension and dyslipidemia for which he is on a ACEi and a statin. He presents with 2.5 hours of ongoing non-radiating chest discomfort while at work. His presenting ECG shows normal sinus rhythm without ischemic changes. His initial high-sensitivity troponin T (hs-cTnT) comes back at 9 ng/L.
Questions
- When would you like to repeat this patients hs-cTnT?
- What would be considered a significant delta?
- How can we implement a risk stratification score like the HEART score to assess the patients risk for major adverse cardiovascular events (MACE)?
The purpose of this post is to provide guidance on ruling out ACS in patients presenting to the emergency department (ED) with low-risk chest pain.
General outline:
- Part 1: Introduction to hs-cTnT testing in the ED.
- Part 2: Evidence surrounding rule out algorithms using hs-cTnT.
- Part 3: Evidence surrounding the use of the HEART score with hs-cTnT; and the presentation of a proposed rule-out algorithm with hs-cTnT that incorporates the HEART score.
PART 1 – INTRODUCTION
4th Universal Definition of Myocardial Infarction (MI)1
- There needs to be a rise and/or fall of cardiac Tn with one value above the 99th percentile with one of the following:
- Symptoms of myocardial ischemic
- New ischemic ECG changes
- Development of pathological Q waves
- Imaging evidence of new loss of viable myocardium or new regional WMA in a pattern consistent with ischemic etiology
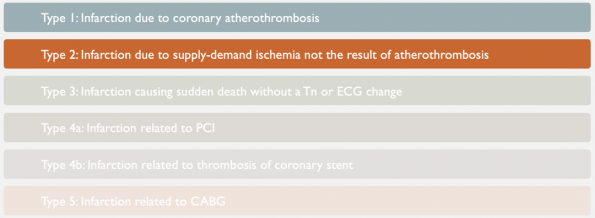
There are 5 main types of MI.1 As emergency physicians, we most commonly encounter types 1 and 2. Type 1 MI is due to coronary artery disease precipitated by plaque rupture. This blog post will focus exclusively on type 1 MI.
Laboratory definitions
- Limit of detection (LOD) is the lowest Tn concentration that can be measured in 95% of samples.
- For our hs-cTnT Roche assay used here at TOH that is 5 ng/L.
- 99th percentile refers to the value above which 1% of healthy individual will have.
- For our hs-cTnT Roche assay that is 14 ng/L.
- So in order to diagnose an MI one value needs to be above 14 ng/L.
- The 99th percentile was chosen as lower thresholds would result in excessive false positives.
- Delta refers to the change in hs-cTnT concentration over fixed time intervals.
- The delta is always compared to the first or presentation Tn.
Conventional troponin vs hs-cTnT

- Conventional troponin assays, as illustrated on the left, were unable to measure low concentrations of TnT and were not precise at measuring concentrations near the cutoff – the 99th With this poor precision, there was a higher chances of missing a MI.
- Historically, we overcame this challenge by performing serial testing to see if these values became detectable. The green arrows along the x-axis, show serial sampling at ED presentation, 3h and 6h from CP onset. As depicted in the graph, we may not detect Tn during our first two samples and only detect them at our 6 hour sample point.
- hs-cTnT is shown on the right. The 99th percentile for this assay is much lower compared to conventional assays. Consequently, much lower physiological levels of troponin are detectable. This results in earlier detection compared to conventional assays.
hs-cTnT is not only more sensitive but is also more precise
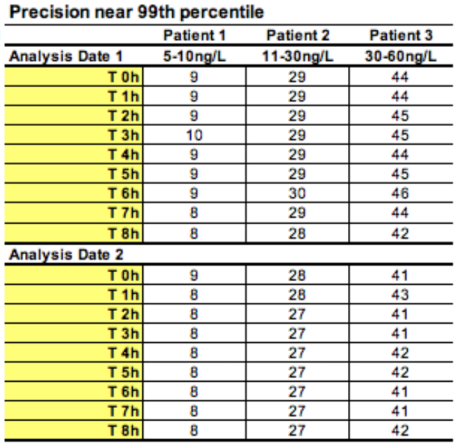
- Precision is defined as the variation seen between measurements.
- This figure shows hs-cTnT samples taken from three patients that were serially tested over eight hours over two separate days.
- In any one of these patients, there is an analytical variability of < 5% at the 99th Our previous conventional troponin had variations between 5-10 ng/L at the 99th percentile.
hs-cTnT testing goes beyond the binary
- Because of this greater precision, troponin values should not be seen as being either positive or negative.
- Evidence shows that as our level of hs-cTnT increases so does out PPV for diagnosing an MI.2
- In other words, the differential diagnosis of an abnormal hs-cTnT is broad at lower concentrations, and narrower at higher concentrations of hs-cTnT.2
- hs-cTnT values should thus be seen as a continuum.
PART 2 – RULE OUT ALGORITHMS
In this section, I will review the evidence for the best validated rule out algorithms for AMI.
- Most algorithms use a combination of absolute cutoff values with the presence or absence of an absolute change over defined time intervals.
- I will discuss rule-out algorithms for when your presentation hs-cTnT is undetectable and more commonly when serial testing is needed at one, two and three hour deltas.
Undetectable hs-cTnT at presentation-
Below the level of detection
- These algorithms were derived on the premise that hs-cTnT assays are sensitive and precise in detecting very low concentrations of troponin and thus an undetectable concentration would be associated with a low risk of AMI.
- Multiple early studies have shown that a value below an assays LOD (Roche hs-cTnT < 5 ng/L) can safely rule out an AMI.3-8
- Pickering et al9 showed that a hs-cTnT < 5 ng/L has a sensitivity of 98.7% and negative predictive value (NPV) of 99.3% for AMI. Additionally, they showed that the pooled sensitivity for MACE was 98% in patients who were ruled out. Moreover, having a hs-cTnT < 5 ng/L and a non-ischemic ECG was able to classify over 30% of patients as being low-risk and safe to go home.
Serial hs-cTnT testing
In most cases patients may present too early for us to reliably depend on a single Tn for rule out. These patients will require serial testing. That is, a hs-cTn taken at ED presentation and subsequent hs-cTn taken at fixed time points to detect the presence or absence of a clinically significant delta.
One-hour hs-cTnT algorithm
- This includes a combination of an ED presentation hs-cTnT < 99th percentile and a non-significant delta one hour after the presentation hs-cTnT was obtained.
- Reichlin et al.10 derived and validated a one-hour rule out algorithm in adult patients presenting to the ED, shown below.
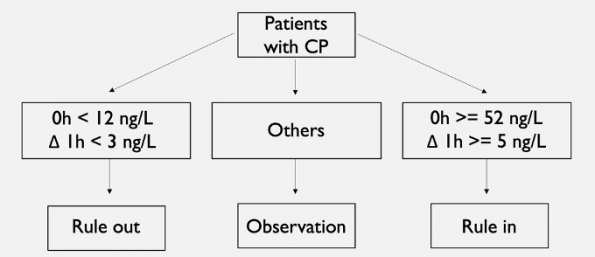
- Rule-out was defined as having a presentation hs-cTnT < 12 ng/L and an absolute change < 3 ng/L.
- Rule-in was defined as either a baseline hs-cTnT >= 52 ng/L or an absolute change >= 5 ng/L. Patients not meeting either criteria were put into an observational zone were additional serial testing was performed.
- The algorithm gave a definitive diagnosis of rule-in or rule-out in 77% of patients within one hour.
- The algorithm had a sensitivity and NPV for rule-out of 100%. For overall rule-in it had a specificity of 94% and a positive predictive value (PPV) of 76%.
- In those ruled-out, the overall pooled 30 day mortality was only 0.2%.
- Reichlin and colleagues11, using their derived algorithm, then performed a large prospective multicenter European validation study.
- The algorithm gave a definitive diagnosis of rule-in or rule-out in 75.9% of patients within one hour.
- The algorithm has a sensitivity of 99.6%, NPV of 99.9%, specificity of 95.7% and PPV of 78.2%.
Two-hour hs-cTnT algorithm
- This includes a combination of an ED presentation hs-cTnT < 99th percentile and a non-significant delta two hours after the presentation hs-cTnT was obtained.
- These algorithms rely on large delta changes compared to one hour algorithms.
- Reichlin et al.12 derived a two-hour algorithm shown below.
- The algorithm was derived in a European cohort then prospectively validated in a non-European cohort.
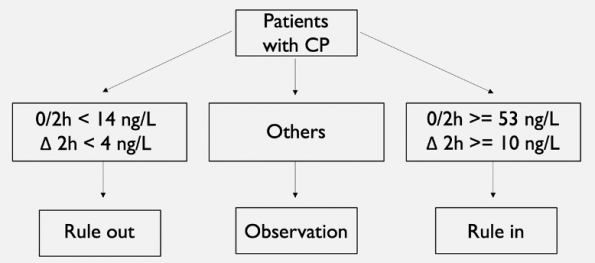
- Rule-out was defined as having a hs-cTnT at presentation and at 2 hours < 14 ng/L and an absolute change within two hours of < 4 ng/L. Rule-in was defined as a hs-cTnT level in the first 2 hours >= 53 ng/L or an absolute change within two hours >= 10 ng/L. Patients who were not classified by either were put into the observational group where serial testing was performed.
- In the overall cohort, the algorithm was able to classify > 75% of patients within 2 hours.
- For rule-out, the algorithm had an overall sensitivity of 98% and NPV 99.6%.
- For rule-in, it had a specificity of 73% and PPV of 42%.
Three-hour hs-cTnT algorithm
- Three hour algorithms use absolute hs-cTnT levels < 99th percentile at 0 and 3 hours or a combination of a low initial concentration and non-significant changes over the 3 hours interval.
- There is comparably more data supporting the aforementioned algorithms.
- The European Society of Cardiology (ESC) three-hour algorithm,13,14 shown below, has the best supporting evidence.
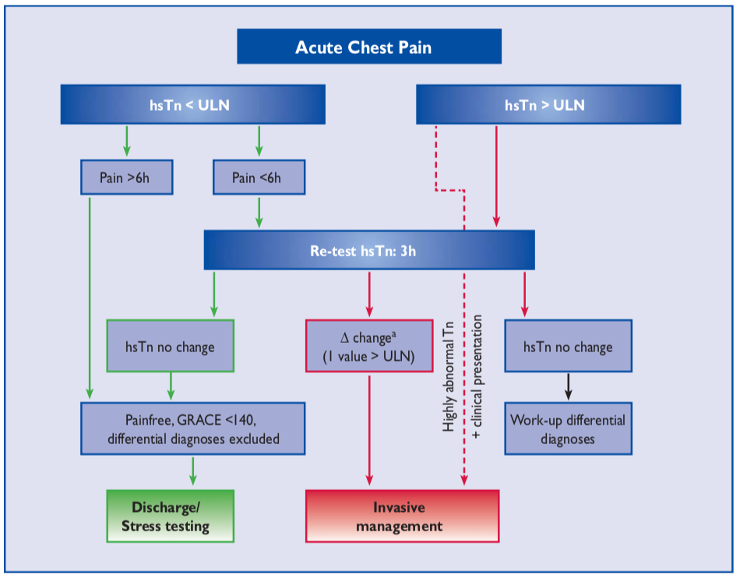
- The ESC 3 hour algorithm is quite complex, requiring the use of the GRACE score, which is a risk-stratification score that estimates six month mortality for patients with ACS.
- With this algorithm, a MI can be ruled out in one of two ways.
- Patients with CP onset >= 6 hours with a presentation hs-cTnT <= 14 ng/L; is CP free; and had a GRACE score < 140.
- Patients with CP onset < 6 hours with a presentation and three hour hs-cTnT <= 14 ng/L; is CP free; and a GRACE score < 140.
- Given the complexity of this algorithm, some studies have opted to include the GRACE score and others have decided not to.
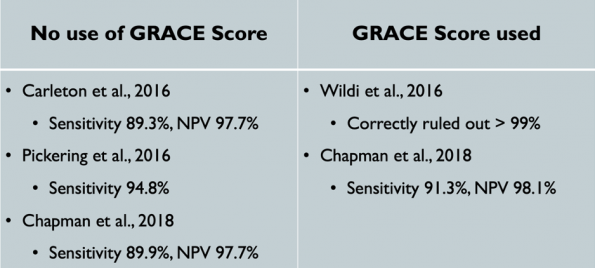
- Overall taken together, regardless of whether the GRACE score was incorporated or not, these studies show that the ESC three hour algorithm has poorer sensitivities in detecting AMIs compared to previous algorithms discussed.
PART 3 – CLINICAL APPLICATION
The previous rule-out algorithms that we covered above are sensitive for AMI but less so for MACE. To improve sensitivities for MACE, there are several algorithms that incorporate risk-scores like the HEART score. In this section, we will focus specifically on the use of the HEART score with hs-cTnT.
HEART pathway
- McCord and colleagues15 conducted a study to see if the HEART pathway could identify low-risk patients using the Reichlin one hour algorithm with hs-cTnT. The intervention group was hs-cTnT levels taken at presentation,1, 2, and anywhere between 4-14 hours combined with a modified HEART score (mHS). Their outcome was 30 day MACE.
- A modified heart score, shown below, takes the first 4 components of the HEART score to create a composite score between 0-8.
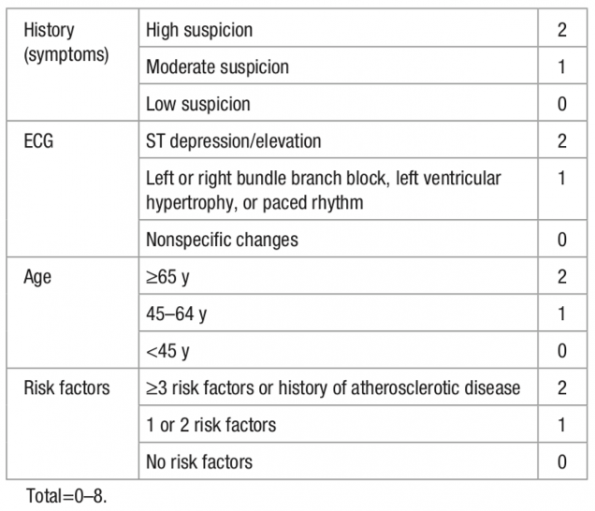
- In order to be considered low risk, patients needed to have either a hs-cTnT < 14 ng/L at various time points or be ruled-out by the one hour algorithm and have a mHS <=3. Having a mHS >= 4 automatically placed a patient in the moderate to high risk group.
- Patients with a hs-cTnT <14 ng/L with a mHS <=3 had lower rates of MACE compared to those >=4, regardless of when the hs-cTnT was taken.
- In patients who were ruled out by the Reichlin one hour algorithm, those with a mHS <=3 had lower rates of MACE compared to those with a mHS >= 4.
- The overall sensitivity and NPV for 30-day MACE was 99.8%.
A systematic review16 found that using a HEART score with hs-TnT lowers MACE from 1.8 to 0.8% compared to conventional troponin.
- The below table shows the diagnostic accuracy of a low-risk HEART score and MACE using hs-cTnT vs conventional troponin.
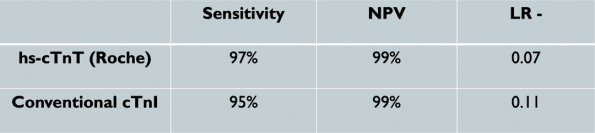
- The use of a hs-cTnT with a low-risk HEART score had lower MACE rates and lower negative likelihood ratios (LR-) compared to conventional troponin.
In this last section, we are going to dive into my proposed hs-cTnT algorithm that takes into consideration the best available evidence for rapid rule out protocols while incorporating the HEART score to help us identify those low-risk patients who can safely go home.
My proposed hs-cTnT algorithm
- Disclaimer: This algorithm is my suggested algorithm based upon the best supporting evidence. This was not clinically derived and validated. This algorithm should not replace clinical judgement and ECG changes. Those patients with high-risk presentation and/or ischemic ECG changes should be considered high-risk regardless of their hs-cTnT value.
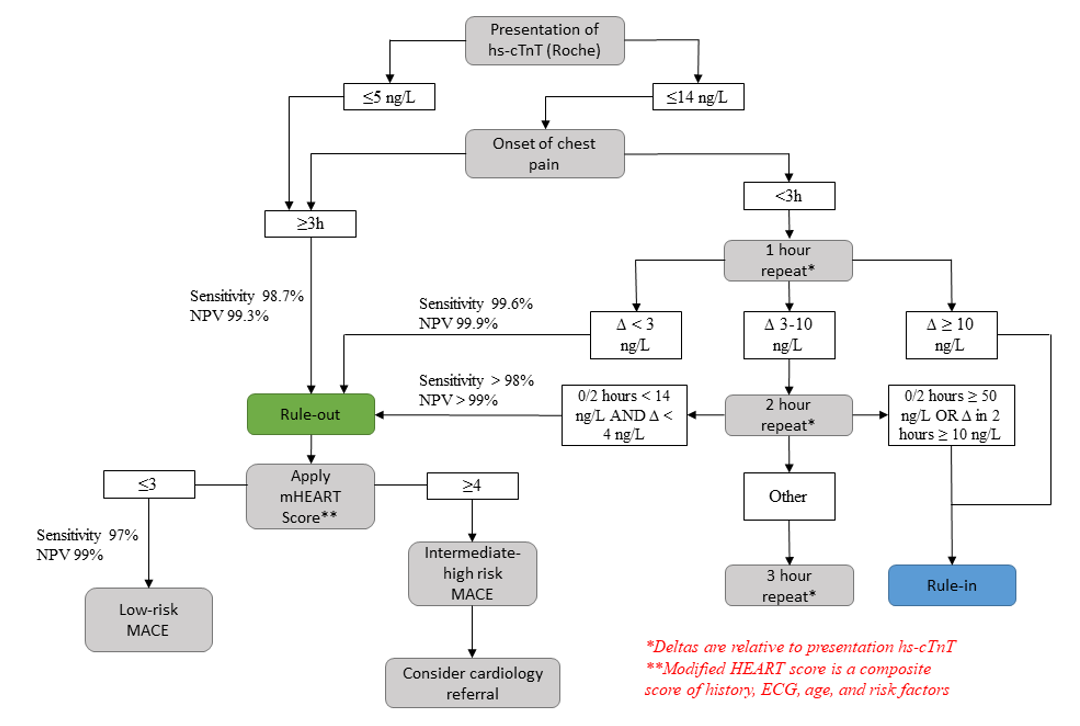
- This proposed algorithm is a combination of a rapid rule-out protocol based upon being undetectable at presentation, or a presentation hs-cTnT < 14 ng/L with non-significant changes at one and two hours.
- A two hour delta was chosen over a three hour delta as there is better evidence and would potentially result in decreased ED length of stay.
Conclusions
- hs-cTnT is much more sensitive and precise compared to conventional troponin.
- hs-cTnT goes beyond the binary and values should be seen on a continuum with larger values representing a narrower differential diagnosis and a larger positive predictive value for diagnosing a MI.
- A hs-cTnT < 5 ng/L can safely exclude an AMI with sensitivities and NPV > 99%. This should only be used in patients with three or more hours of chest pain onset.
- The Reichlin one and two hour algorithms have high sensitivities (>98%) and NPV (>99%) and can classify > 75% within one or two hours, respectively.
- The Reichlin two hour algorithm has the best combination of efficiency and accuracy and requires larger deltas, making it less prone to analytical assay variation.
- Overall sensitivities for the ESC three hour algorithm are not as robust when compared to other algorithms. Additionally, given the requirement of the GRACE score, it is not clinically feasible.
- The use of the HEART pathway and hs-cTnT give sensitivities and NPV > 99%.
- A single hs-cTnT <= 5 ng/L after three hours of chest pain onset or a two hour delta < 4 ng/L in concert with a HEART score <= 3, and a non-ischemic ECG rules out AMI and lowers 30-day MACE to 0.8%. These are the patients who are low-risk and safe to be discharged home.
References
1Thygesen, K. (2018). What’s new in the Fourth Universal Definition of Myocardial infarction? European Heart Journal, 39(42), 3757–3758. doi: 10.1093/eurheartj/ehy655
2Januzzi, J. L., Mahler, S. A., Christenson, R. H., Rymer, J., Newby, L. K., Body, R., … Jaffe, A. S. (2019). Recommendations for Institutions Transitioning to High-Sensitivity Troponin Testing. Journal of the American College of Cardiology, 73(9), 1059–1077. doi: 10.1016/j.jacc.2018.12.046
3Body, R., Calrey, S., McDowell, G. et al. (2011). Rapid exclusion of acute myocardial infarction in patients with undetectable troponin using a high-sensitivity assay. J Am Coll Cardiol, 58, 1332-9.
4Gimenez, M. R., Twerenbold, R., Reichlin, T., Meller, B., Moehring, B., Haaf, P., … Mueller, C. (2013). One-hour algorithm for early rule-out and rule-in of acute myocardial infarction using sensitive cardiac troponin i. European Heart Journal, 34(suppl 1). doi: 10.1093/eurheartj/eht308.p1300
5Bandstein, N., Ljung, R., Lundbäck, M., Johansson, M., & Holzmann, M. J. (2017). Trends in admissions for chest pain after the introduction of high-sensitivity cardiac troponin T. International Journal of Cardiology, 240, 1–7. doi: 10.1016/j.ijcard.2017.04.028
6Shah, A., Anand, A., Sandoval, Y., et al. (2015). High-sensitivity cardiac troponin I at presentation in patients with suspected acute coronary syndrome: a cohort study. Lancet, 386, 2481-8.
7Parsonage, W. A., Mueller, C., Greenslade, J. H., Wildi, K., Pickering, J., Than, M., … Cullen, L. (2016). Validation of NICE diagnostic guidance for rule out of myocardial infarction using high-sensitivity troponin tests. Heart, 102(16), 1279–1286. doi: 10.1136/heartjnl-2016-309270
8Mcrae, A. D., Innes, G., Graham, M., Lang, E., Andruchow, J. E., Yang, H., … Kavsak, P. (2017). Comparative Evaluation of 2-Hour Rapid Diagnostic Algorithms for Acute Myocardial Infarction Using High-Sensitivity Cardiac Troponin T. Canadian Journal of Cardiology, 33(8), 1006–1012. doi: 10.1016/j.cjca.2017.04.010
9Pickering et al. (2017). Rapid Rule-out of Acute Myocardial Infarction With a Single High-Sensitivity Cardiac Troponin T Measurement Below the Limit of Detection. Annals of Internal Medicine, 166, 715-724. doi:10.7326/M16-2562
10Reichlin et al. (2012). One-Hour Rule-out and Rule-in of Acute Myocardial Infarction Using High-Sensitivity Cardiac Troponin T. Arch Intern Med, 172 (16): 1211-1218
11Reichlin et al. (2015). Prospective validation of a 1-hour algorithm to rule-out and rule-in acute myocardial infarction using high-sensitivity cardiac troponin T assay. CMAJ, 187(8): 243-252
12Reichlin, T., Cullen, L., Parsonage, W., et al. (2015). Two-hour algorithm for triage toward rule-out and rule-in of acute myocardial infarction using high-sensitivity cardiac troponin T. Am J Med, 128(4), 369-379.
13Hamm, C., Bassand, J., Agewall, S., et al. (2011). ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur Heart J, 32, 2999-3054.
14Wildi et al. (2017). Direct comparison of 2 rule-out strategies for acute myocardial infarction: 2-h accelerated diagnostic protocol vs 2-h algorithm. Clinical Chemistry, 63(7): 1227-1236.
15McCord et al. (2017). Prognostic utility of modified HEART score in chest pain patients in the Emergency Department. Circ Cardiovasc Qual Outcomes, 10: 1-8.
16Laureano-Philips, J., Robinson, R., Aryal, S., et al. (2019). HEART score risk stratification of low-risk chest pain patients in the emergency department: A systematic review and meta-analysis. Annals of Emergency Medicine, 74(3), 187-203.


Thanks, fantastic review and helpful suggestions for clinical application!
I’m just seeing this now a few years after posting, but thank you so much for this review!
Such an organized approach to ACS diagnostics. I wish the AHA and JACC reviews could be this logical/organized!
One question about your proposed hs-cTnT algorithm. I agree that a patient with >3hrs of chest pain and 3hrs of chest pain and 5.0-14.0ng/L (3hrs of chest pain and a hs-cTnT < 5.0ng/L (and a "non-ischemic appearing" ECG).
Is this correct? Or have I missed something?
Thank you again for this fantastic review.
I look forward to your response!
Sorry my above comment didn’t come through in full…
I’ll repeat here:
I’m just seeing this now a few years after posting, but thank you so much for this review!
Such an organized approach to ACS diagnostics. I wish the AHA and JACC reviews could be this logical/organized!
One question about your proposed hs-cTnT algorithm. I agree that a patient with >3hrs of chest pain and 3hrs of chest pain and 5.0-14.0ng/L (3hrs of chest pain and a hs-cTnT < 5.0ng/L (and a "non-ischemic appearing" ECG).
Is this correct? Or have I missed something?
Thank you again for this fantastic review.
I look forward to your response!