

In situ simulation, informally thought of as “crash testing the dummy”, is defined as a team-based training technique conducted within the actual patient care environment, involving members of the healthcare team using equipment and resources from the unit1,2. It is a training technique that lends itself to the field of emergency medicine given the complex and chaotic nature of the discipline, which is often difficult to replicate in a simulation lab. In situ simulation has been pivotal for systems testing and integration of novel workflows, protocols, and cognitive aids to institute rapid changes to practice and care delivery3. Consequently, it seemed logical to apply it to address the rapidly evolving COVID-19 response.
Benefits and Challenges of Conducting In Situ Simulation
Benefits
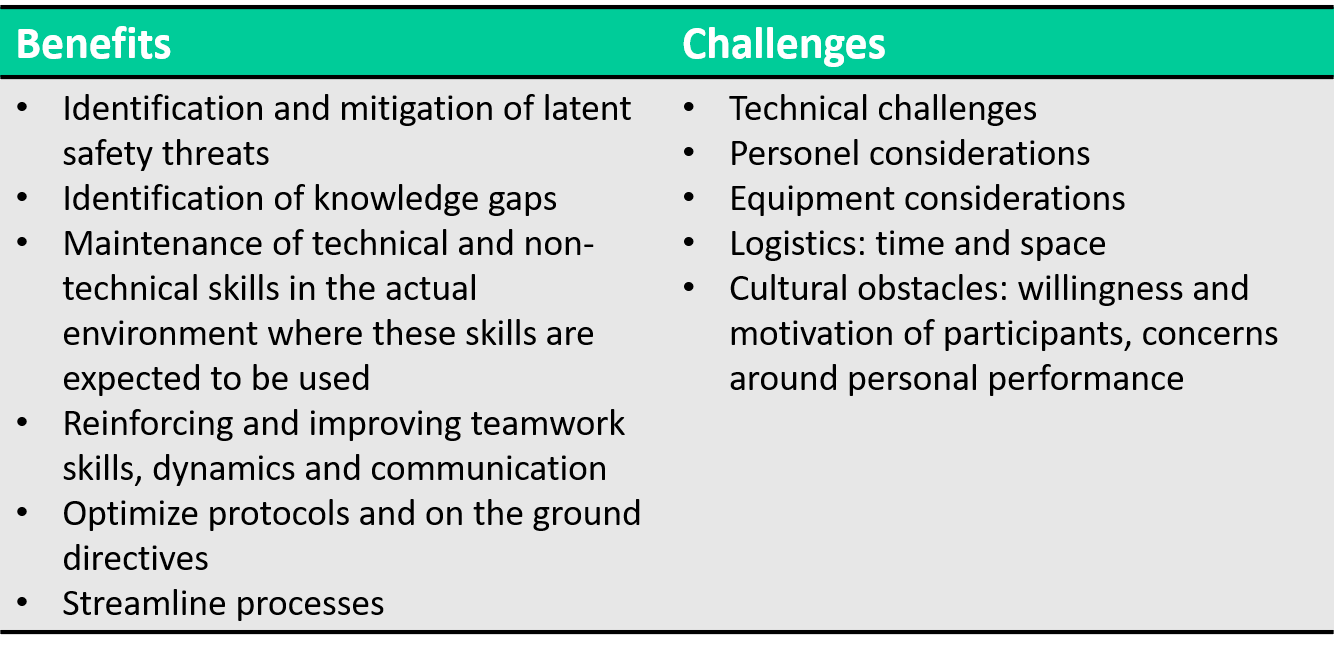
It is important to consider both the utility and the challenges of in situ simulation in the context of emergency preparedness. First, in situ simulation allows for the identification and mitigation of latent safety threats (LSTs), thus improving patient safety and care. LSTs are system-based threats to patient safety that lie dormant or are unrecognized by healthcare providers and administrators. They can materialize at any time and may influence patient morbidity and mortality. As such, their identification is of importance. Second, through in situ simulation, individual providers are able to identify gaps in knowledge and refine both their technical and non-technical skills within the environment where they would be applying these skills. Third, in situ simulation affords benefits to the healthcare team by reinforcing and improving teamwork skills, dynamics, and communication. Finally, there are benefits to the healthcare system at large, as optimization of protocols and directives on the ground and streamlining operations, affords financial and systemic efficiencies.
Challenges
Despite these benefits, in situ simulation does have its challenges. There are technical challenges with the mobilization of high fidelity simulation equipment into the clinical environment. There are also resource considerations regarding personnel (eg., who will be participating in the sim, who will be running the sim, who will be operating the equipment), and medical equipment (eg., what supplies should be used for the simulation, should we be using mock equipment that might be dedicated to simulation activities or should we be using the ED equipment and supplies recognizing that we might deplete resources that may be required for actual patient care). Furthermore, there are logistic considerations for time and space; in recognition that in situ simulation may place stress on an already stressed system. Additionally, a poorly timed in situ simulation may have the dual negative impact of disrupting patient care and failing to achieve the objectives of the simulation, due to poor participant engagement. Cultural obstacles are also present in the form of participant willingness and motivation to participate in the context of concerns surrounding personal performance1,3.
Table 1. Summary of the Benefits and Challenges of Conducting In Situ Simulation
A New Simulation Frontier…Translational Simulation
Traditionally, simulation descriptors often focus on the type of device used (for example high fidelity or low fidelity mannequin) or the location where the simulation takes place (for instance in situ vs. off-site simulation). However, by relying solely on these descriptors, we underplay the critical importance of the outcomes gained from simulation4. Consequently, over the past few years, a new concept has emerged in the simulation world known as Translational Simulation.
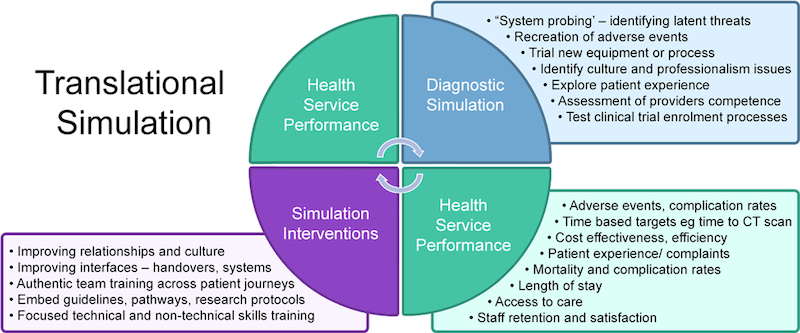
Translational simulation describes a subset of simulation activities that are aimed directly at improving healthcare processes and outcomes4. It achieves this through two main categories of simulation:
- Diagnostic Simulations: which includes system probing simulations, trialing of new equipment, assessment of provider and team competence, and identifying cultural and professional issues.
- Simulation Interventions: which are simulations aimed to improve relationships and culture, enhance team training across the entire patient journey, embed guidelines, pathways and protocols, in addition, to focusing on technical and non-technical skills training.
Similar to quality improvement approaches like the Plan Do Study Act (or more commonly known as the PDSA cycle), translational simulation first plays a role in diagnosing safety issues and then by creating simulation-based intervention to address those safety issues.
The First Simulations for COVID
So how did we leverage simulation-based education, in situ simulation, and a translational simulation approach to preparing our staff, department, institution, and system at large to prepare to care for COVID-19 patients during this pandemic?
Our first simulation was conducted on March 9, 2020, and was a multi-disciplinary, in situ simulation involving MDs, ED nurses, RTs, care facilitators, and members of the hospital security team. It focused on the case of a returning traveler from China who was presenting to triage with respiratory distress and fever. Initial simulations were conducted at both The Ottawa Hospital (TOH) General and Civic campus emergency departments.
It was conducted as a hybrid simulation; where a standardized patient actor, played by a nurse educator, presented to emergency triage with COVID-19 symptoms. They were then registered, triaged, and transferred to a negative pressure resuscitation bay, where the actor was replaced by a 3G simulation mannequin. In subsequent minutes, the team performing the simulation was responsible for the identification of hypoxic respiratory failure requiring intubation and transfer to the ICU. The simulation scenario was terminated when the team arrived at the doors of the ICU with the sim mannequin. After completing the exercise, a debrief of the scenario was conducted with the entire team to identify challenges, latent safety threats requiring an immediate attention, and strong/ideal performances.
Translational Simulation Cycle for COVID
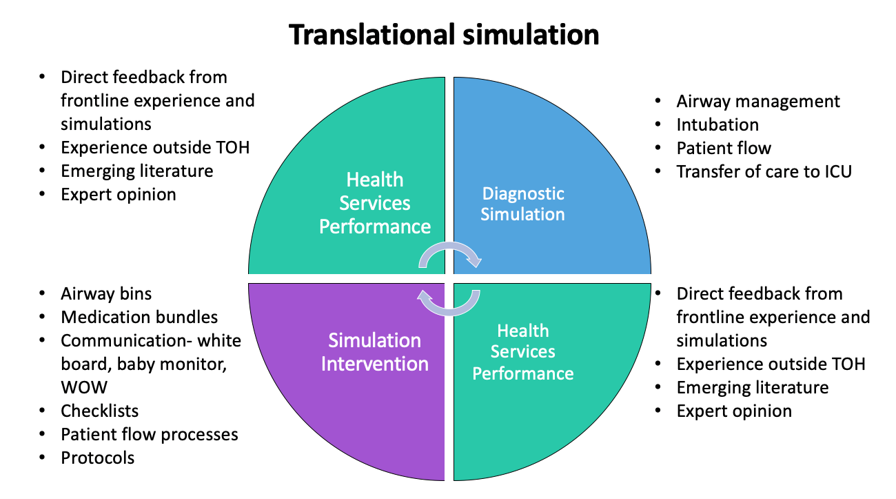
We started with several diagnostic simulations similar to the above scenario, which focused on airway management and intubation. These were used to probe the system, examine patient flow, and identify gaps both in knowledge and existing processes. Information gathered from diagnostic simulation debriefs was amalgamated with direct feedback from frontline experiences, emerging literature, and expert opinion to develop procedures, protocols, and system processes that identified and mitigated safety threats. We then developed interventions to address these threats and then trialed them in subsequent simulations. Through further debriefing of these scenarios, we sought feedback about what worked, what didn’t work, and what was still unclear. This iterative process continued over the course of March and early April until we finalized our protocols.
Identification of LSTs Using Simulation for COVID
From our simulations, we identified a number of latent safety threats that fell into a few key categories:
- Process and Workflow;
- Equipment;
- Communication;
- Knowledge gaps.
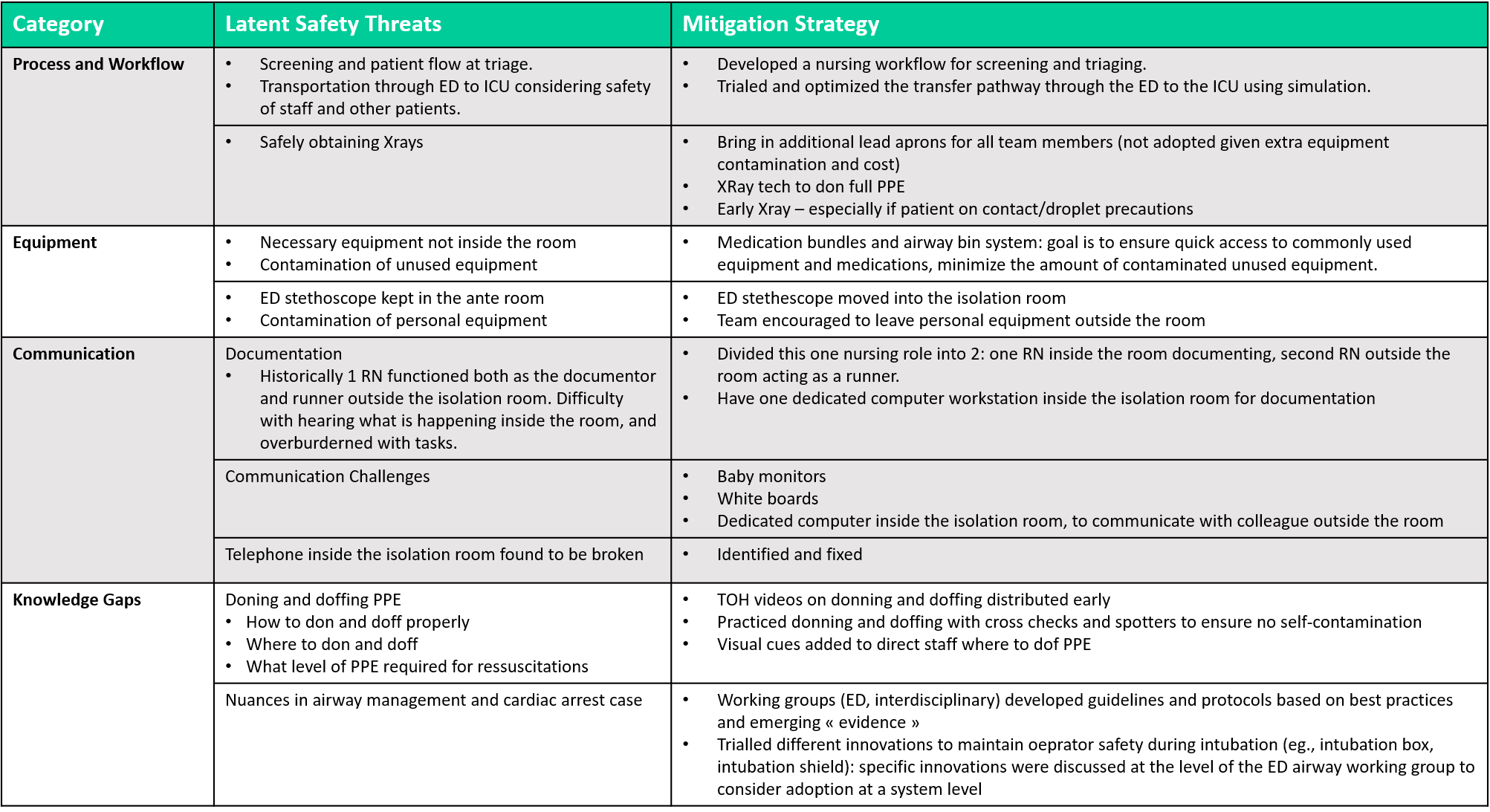
The key latent safety threats, mitigation strategies, and interventions are summarized in the table below.
Table 2. Identification of Latent Safety Threats During In Situ Simulation
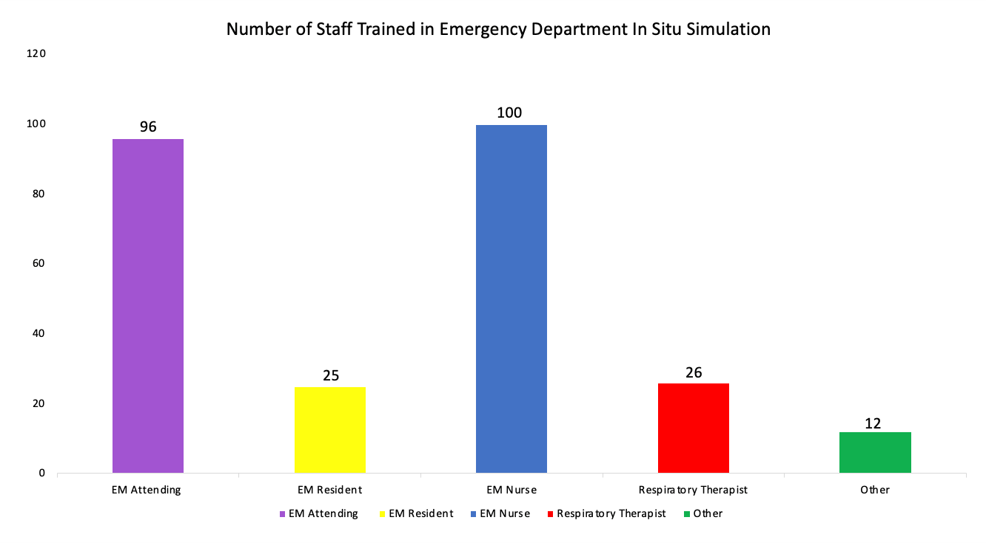
Training using simulation
Once our protocols and processes were finalized and key safety threats were mitigated, our focus shifted to training medical staff. In situ simulations were used to rapidly disseminate new knowledge to front line staff. In addition to in situ simulation and on-shift airway training, infographic summaries and cognitive aids were used to summarise protocols and to help disseminate key messages. A total count of staff trained in ED in situ simulations is provided below.
Challenges to Running In Situ Simulation for COVID During a Pandemic
Upon reflection of our experience, we found a number of benefits of conducting in situ simulation during the COVID-19 pandemic:
- Ability to work through practical aspects of care of COVID patients: craft protocols, test drive them through sim and streamline patient care processes;
- Rapidly disseminate new knowledge and to train frontline staff on newly established procedures and protocols;
- Optimize our communication and to continue to identify and mitigate latent safety threats.
However, as the pandemic progressed, there were certain challenges related to in situ simulations that warranted careful consideration:
- The need to maintain physical distancing and limiting the number of people participating in a given simulation;
- Possible exposure of participants, educators, and simulation techs and the potential for occupation spread of the virus;
- Placing more stress on an already stressed ED system;
- Potentially depleting PPE supplies, which may be required for actual patient care.
Turning to a Digital Strategy with Virtual Reality (VR) Video Technology
Considering the above limitations, the TOH education and the Simulation Patient Safety Program quickly pivoted to a digital strategy with the development of virtual reality (VR) videos.
The goals of this initiative were threefold:
- Use VR as an educational tool to improve patient care and the safety of frontline healthcare providers amidst the COVID-19 pandemic;
- Maximize the impact of simulation training across institutions by sharing organizational learnings, and;
- Coordinate a largescale response to the pandemic over wide geographic areas, in particular areas that may not have access to in situ simulation training.
A virtual reality 360-degree digital camera was used to capture video from exemplar scenarios of rehearsed teams managing complex situations. The benefit of the VR videos, as opposed to traditional static videos of the simulation, was that you got a 360-degree view of the room. This enabled the learner to immerse themselves in the scenario and to explore multiple viewpoints as the case progressed.
There are a couple of different options to watch VR videos in order to get the full immersive experience. There are handsfree options, such as high tech gaming headsets (cost = $400), or the google cardboard (cost = $20). You can also watch VR videos on YouTube on your smartphone (although this option does not provide a hands-free experience).

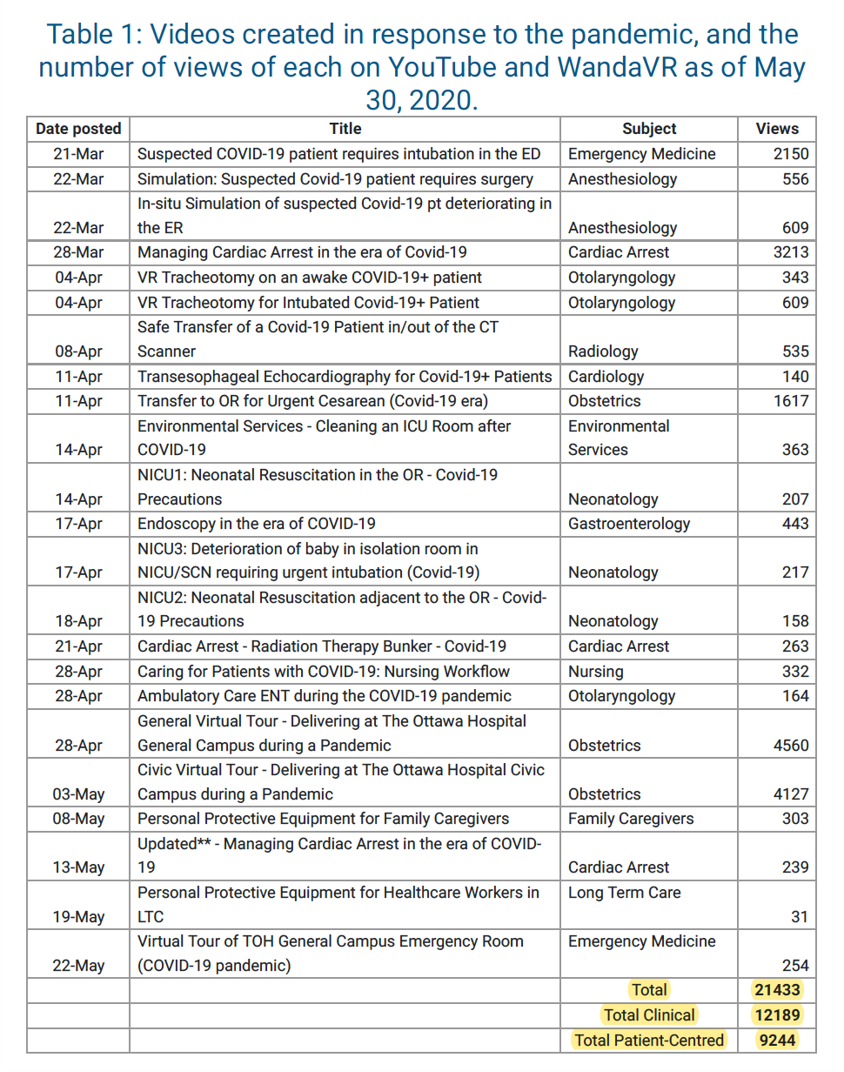
Some of the first VR video recordings at our institution occurred in our emergency department; videos covering the treatment of a COVID-19 patient in respiratory distress and the COVID-19 patient requiring intubation. Different cases were designed to improve team preparedness for safe and effective patient care in various clinical settings where a code blue or Aerosol Generating Medical Procedure (AGMP) is required. In total, 19 clinical scenarios were filmed, including a COVID-19 patient requiring a C-section, transesophageal ECHO, tracheotomy, transfer in and out of the CT scanner, and neonatal resuscitation cases.
Once the videos were recorded and edited, they were shared on the TOH Education website, which is publicly accessible on the internet. This allows us to share our organizational learnings on a larger scale. Each case is accompanied by a link to a VR video on YouTube. They also all have an identified goal, specific learning objectives, and demonstrates an aspect to hospital preparedness for managing patients during the COVID-19 pandemic. Once the content was created for all essential front-line areas of the hospital, content geared towards patients, family caregivers, and long-term care facilities including virtual tours of the hospital and PPE training videos.
Outcomes of Virtual Simulation for COVID
By the end of May 2020, there had already been over 12,000 views of the 19 clinical videos and nearly 10,000 views of patient-centered videos5. TOH education has also received local as well as international feedback from other institutions that have used these videos to guide local practice, as well as implement protocols that are adapted based on local resource availability.
Future Directions of Simulation for COVID-19
In situ simulations continues to be practiced in our emergency departments, with the goals of improving pandemic resuscitations by:
- Reviewing and practicing our established protocols, highlighting nuances in airway management and in protected code blue scenarios;
- By practicing effective team communication;
- And by identifying latent safety threats to patients and healthcare providers when caring for these high-risk patients in a resource-limited setting.
In addition to ongoing in situ simulations in our departments, two of our staff physicians Dr. Lindsey McMurray and Dr. Marianne Yeung are working to establish a community outreach COVID simulation program for EDs in the Ottawa area. The idea is to run in situ simulations in community EDs within the Ottawa area. This would help with the identification of local latent safety threats, optimize treatment protocols for COVID patients, and tailor protocols to available local resources. We are looking forward to offering this program to community EDs in the near future!
Furthermore, our very own resident Dr. Wilson Lam is also working alongside the SRPC to develop SIM programs for Rural Emergencies.
References
- Patterson MD ea. In situ simulation: detection of safety threats and teamwork training in a high risk emergencydepartment. BMJ Quality and Safety2013. p. 468–477.
- Posner GD, Clark ML, Grant VJ. Simulation in the clinical setting: towards a standard lexicon. Adv Simul (Lond). 2017;2:15. doi:10.1186/s41077-017-0050-5
- Petrosoniak A, Auerbach M, Wong AH, Hicks CM. In situ simulation in emergency medicine: Moving beyond the simulation lab. Emerg Med Australas. Feb 2017;29(1):83-88. doi:10.1111/1742-6723.12705
- Brazil V. Translational simulation: not ‘where?’ but ‘why?’ A functional view of in situ simulation. Adv Simul (Lond). 2017;2:20. doi:10.1186/s41077-017-0052-3
- G P, J M, J D-T, K E, J C. Virtual reality videos for training and protocol dissemination during a pandemic, MedEdPublish, 2020


Fantastic, well done. Have you tried to use McKinsey Model. Thanks