

You’re working a night shift when you are handed the following ECG from triage in a 50 year old male, with no past medical history, presenting with chest pain:
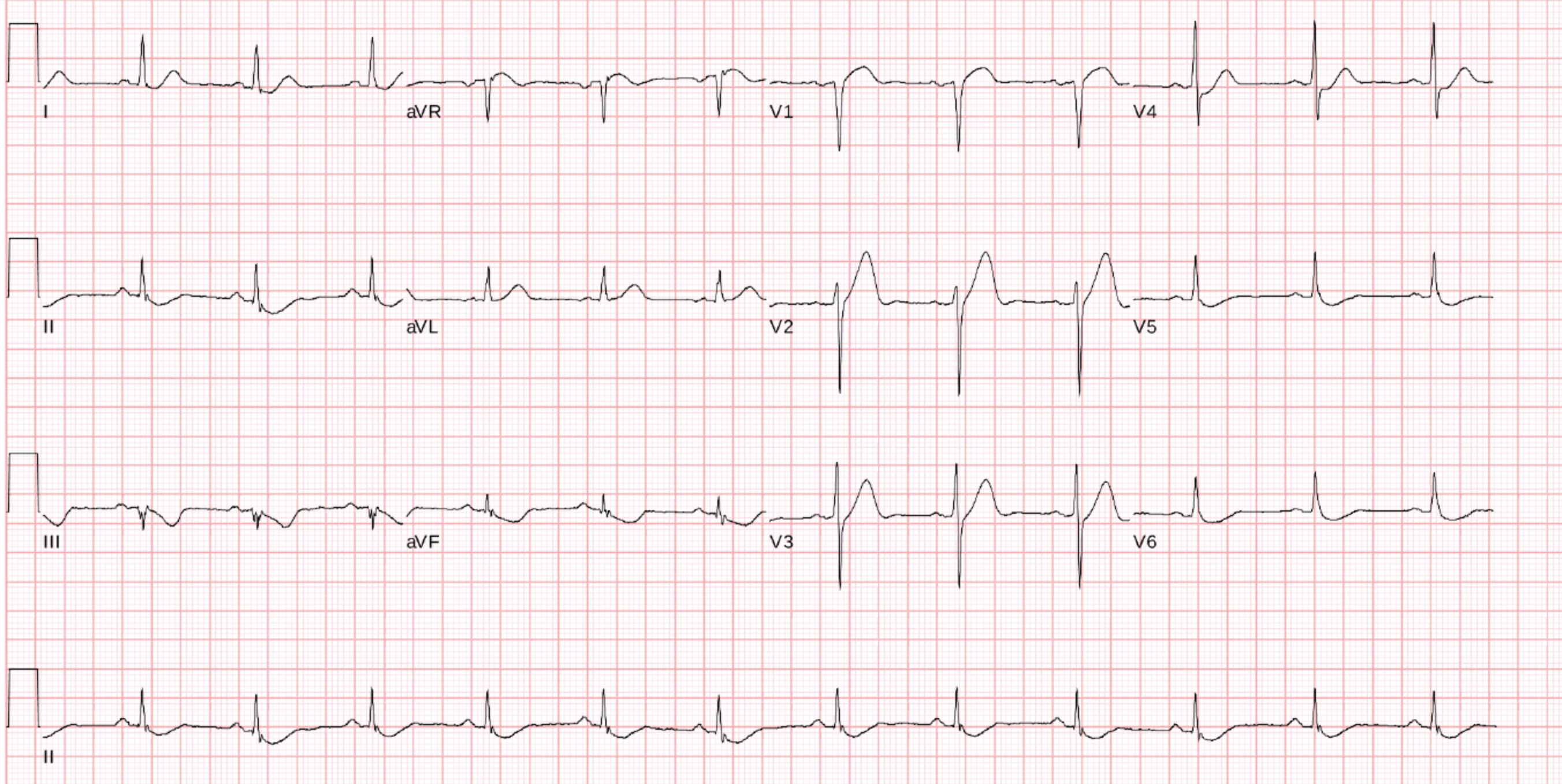
What abnormalities do you notice? What is your approach?
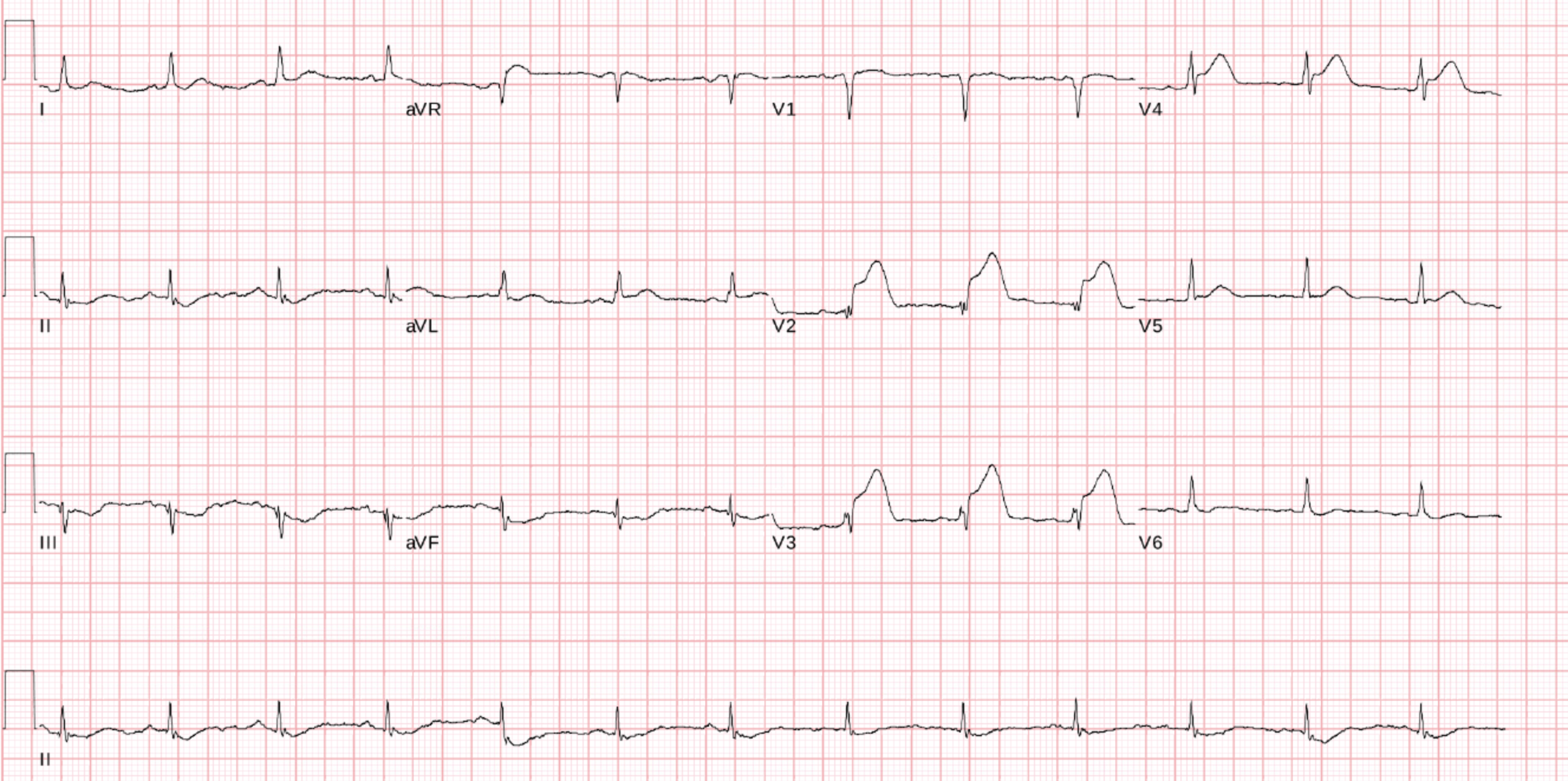
This ECG is concerning for ACS – so the patient is triaged to a monitored area, a repeat ECG ordered and urgent physician assessment. Thoughts? Well… this looks a lot better. Previous abnormalities have corrected. ST/T wave segments are all flat. When you’re observing delta changes, the best course of action is to get another ECG. Hmmmm.. This is a fairly classic ECG for a biphasic Wellens Syndrome – suggestive of a critical stenosis to the LAD. The diagnostic criteria for Wellens Syndrome has previously been established: The patient was found to have no pulse, CPR was started and he was defibrillated immediately with ROSC. He was alert and conscious at this point in time – he was treated for ACS, given anti-dysrhythmias and the Cath lab was activated. His post ROSC ECG was as follows: Unsurprisingly, the patient had a 100% LAD occlusion that was stented, and he returned home neurologically intact a few days later. Interpretation
15 minutes later the patient reports his pain is improving, and his ECG looks like this:
Interpretation
15 minutes later, the patient reports his pain has resolved, and his repeat ECG looks like this: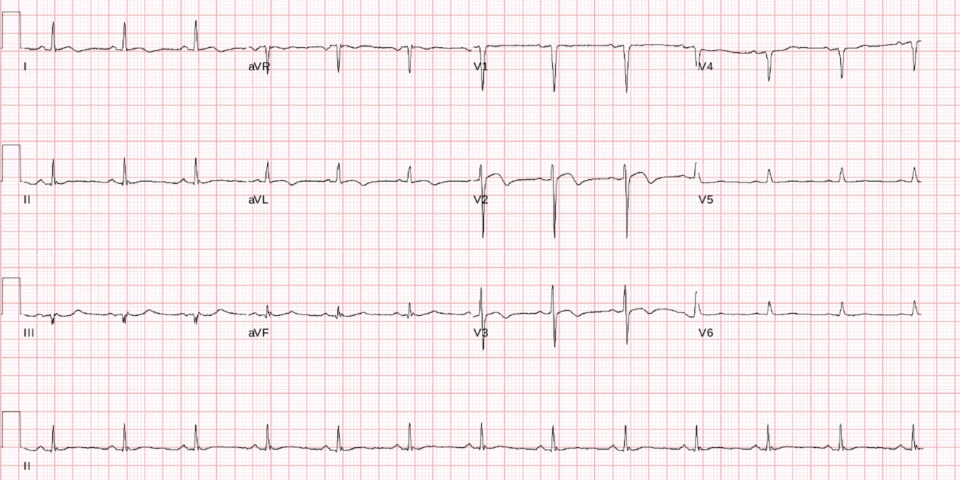
Interpretation
As we were preparing to pick up the phone to call cardiology and initiate treatment for ACS, we were called STAT to the bedside: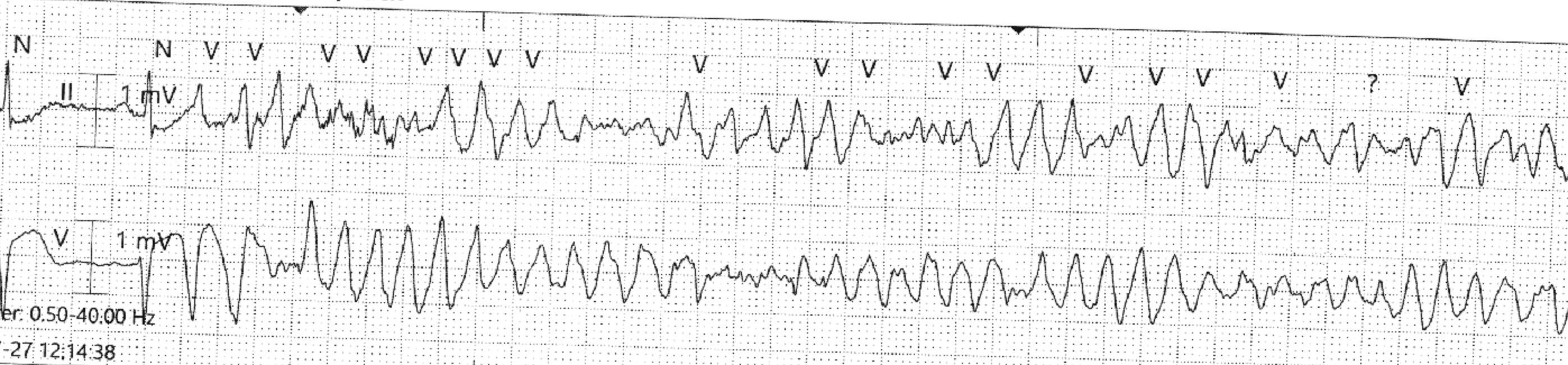
Interpretation and case resolution
Conclusions
Author
