


Emergency department (ED) deliveries can be among the most stressful events an emergency physician can encounter. We must assess both mother and fetus simultaneously and be prepared to manage both maternal and neonatal resuscitations and any complications within the intrapartum and postpartum periods.
Although the incidence of performing ED deliveries is low, the stakes are much higher. The following list outlines the increased rates of various complications1:
- Infant resuscitation → 25%
- Infant mortality → 9%
- Nuchal cord → 9%
- Postpartum hemorrhage → 6%
- Shoulder dystocia → 3%
- Cord prolapse → 1%
Given these higher rates of obstetrical emergencies in the ED setting, this blog post aims to highlight the need-to-know details and provides an approach you can use when managing deliveries in the ED and their feared complications. By the end of this 2-part series, we hope you will feel more comfortable with the following scenarios:
- Performing a precipitous delivery
- Managing shoulder dystocia
- Managing nuchal cord emergencies
Part 2 will focus on: - Managing postpartum hemorrhage
- Running a maternal cardiopulmonary arrest code, while aware of the indications and steps to performing a resuscitative hysterotomy
For more information on early pregnancy loss — a Patient-centered approach, click here.
OBJECTIVE 1: Managing Precipitous Deliveries
The initial ED assessment involves determining if a delivery is deemed imminent. If imminent, your priority will be preparing for two patients.
What equipment and medications will be needed?
- For infant → neonatal warmer, blankets, suction, cardiorespiratory monitors, pediatric airway equipment
- For mother → sterile gloves, gown and towels, 2 umbilical clamps or hemostats, sterile scissors, uterotonic agents (ie. oxytocin)
If time permits, perform a quick evaluation to determine:
- Estimated due date (if unknown, use last menstrual period or fundal height)?
- Single vs multiple gestation?
- Complicated vs uncomplicated pregnancy?
- Bishop score including cervical effacement & dilation
- What the presenting part is?
What are the steps to performing the delivery itself?
- Place the patient in the resuscitation area of the ED, preferably in a gyne bed and in the dorsal lithotomy position.
- Apply gentle pressure with a sterile towel using your dominant hand to support the perineum, easing the pressure of head descent to prevent vaginal tears. Apply gentle pressure with your non-dominant hand to the head with slight flexion to the infant’s neck as the mother gives small pushes.
- The infant will restitute and rotate to face the maternal thigh after the head is delivered. Now is the time to check for a nuchal cord by running your finger around the neck.
- To deliver the anterior shoulder, place your palms on the infant’s cheeks and apply gentle downward traction. Oxytocin 10 units IM should be administered after delivery of the anterior shoulder. In the ED setting, it can be administered promptly following the infant’s delivery.
- Use gentle upward traction to lift the head to deliver the posterior shoulder.
- Following both shoulders, the rest of the body usually delivers spontaneously without difficulty. Support the infant carefully with one hand at the neck and one at the feet. If you remember anything from this blog post – don’t drop the baby!
- Place two clamps or hemostats 4-5 cm apart about 3 cm away from the infant’s umbilical insertion point and cut the cord at 30-60 seconds between the two clamps.
- If both patients are stable, place the infant on the maternal chest. If there’s any instability, the infant should be taken directly to the warmer for further resuscitation.

What about delivering the placenta?
Separation of the placenta after delivery of the infant usually happens within 5 minutes but can take up to 15 minutes. Remember the signs to recognize impending placental delivery including: a gush of blood, firming of the uterus, or spontaneous umbilical cord lengthening.
The mother can bear down to aid in delivery of the placenta if it has not spontaneously separated after 5 minutes. If maternal force alone is not sufficient, you can help by applying suprapubic pressure while keeping the cord taught with a clamp in the other hand.
Remember – you should never use forceful traction or force the expulsion of the placenta before its natural separation, as this increases the risk of uterine inversion.
Take home point #1: There are higher rates of complications with deliveries in the ED setting so being adequately prepared and aware of the possible downstream sequelae is of greatest importance.
OBJECTIVE 2: Managing Shoulder Dystocia
What is it?
Shoulder dystocia refers to the bony impaction of fetal shoulders against the pelvic outlet after fetal head delivery. Often, it is difficult to predict which cases may encounter this complication but proposed and reported risk factors include: gestational diabetes, fetal macrosomia, and post-term pregnancies.
How do I recognize shoulder dystocia?
It can be recognized by presence of the “turtle sign” during deliveries – when the fetal head retracts back toward the mother’s perineum immediately after its presentation. You can also look for fetal facial flushing and failure to deliver the anterior shoulder as other signs after the head is delivered.
Importance of early recognition?
This presentation requires rapid action by the caring physician, as failure to recognize or manage it can result in significant fetal and maternal morbidity, such as postpartum hemorrhage, 3-4th degree maternal tears, fetal brachial plexus injuries, fetal clavicle and humerus fractures, and fetal hypoxic-ischemic encephalopathy. The following algorithm can help to provide a rational and easy approach to managing shoulder dystocia, outlining the least to most invasive maneuvers.
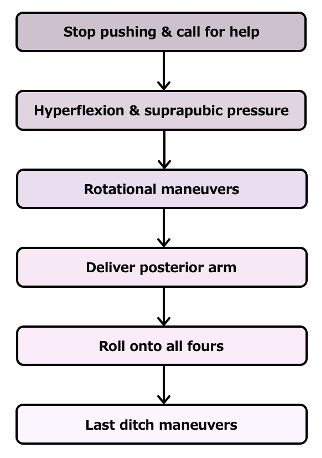
Step 1: Stop pushing and call for help
- Once recognized, instruct the mother to stop pushing to avoid worsening the underlying problem, announce the diagnosis to your team & get help from your colleagues (ie. obstetrics, neonatologists, anesthesiologists).
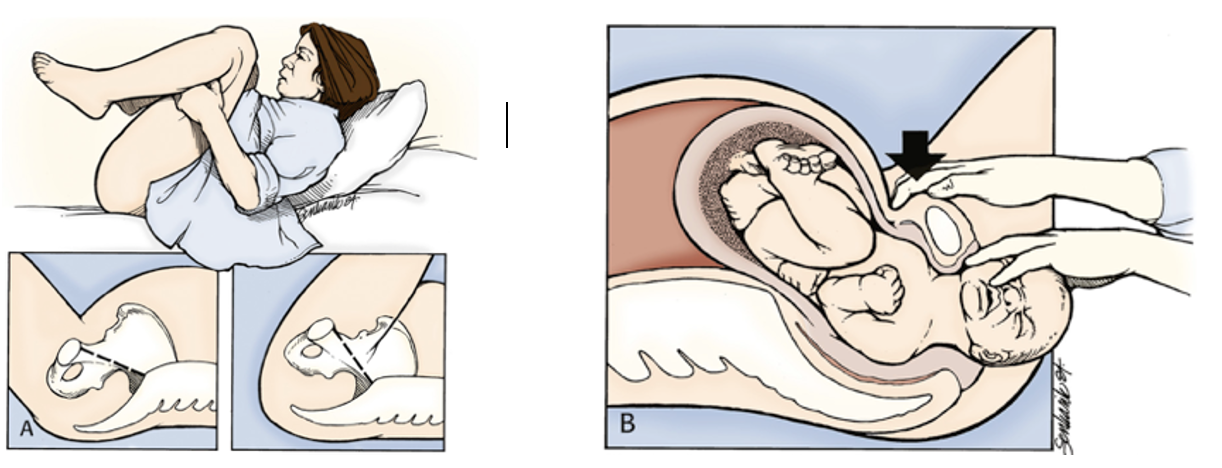
Step 2: Hyperflexion and Suprapubic Pressure
- Given its ease and non-invasive nature, perform the McRoberts maneuver next by hyperflexion of the maternal hips. Use two assistants on either side of the patient holding up the legs flexed against the abdomen. The goal is to move the symphysis pubis cephalad, walking it up and over the infant’s anterior shoulder.
- Simultaneously, suprapubic pressure is applied in an oblique direction from the posterior aspect of the top shoulder towards the fetal face, allowing it to internally rotate and adduct, reducing overall diameter.
- The success rate of this technique is approximately 60%.
Step 3: Rotational Maneuvers
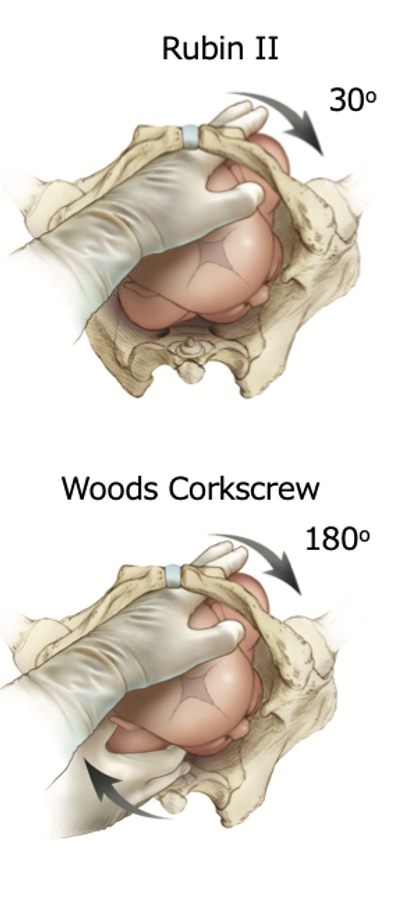
- If the above fails, perform internal maneuvers to manually attempt to rotate the fetal shoulders and mitigate impaction.
- Rubin II → insert two fingers on the backside of the anterior shoulder and rotate the shoulder 30 degrees toward the fetal chest.
- Wood’s Corkscrew → keeping two fingers in the same location as the Rubin II, place your other hand on the anterior aspect of the bottom shoulder, apply pressure and continue to rotate the fetus 180 degrees in the same direction. If successful, the posterior shoulder becomes the anterior shoulder, advancing the infant down the pelvic outlet.
Step 4: Delivery of the posterior arm
- Although this method relieves up to 84% of cases, it is one of the most complicated maneuvers to perform.
- Insert one hand along the infant’s posterior arm, down to the elbow level. Place pressure in the antecubital fossa, flexing the fetal arm until the forearm or hand can be gripped by you and swept across the infant’s chest to deliver the posterior arm.
Step 5: Roll onto all Fours
- Next, roll the patient onto their hands and knees.
- This repositioning technique increases the pelvic outlet by up to 2 cm and in combination with gravity, allows for more space to deliver the posterior arm and disimpact the anterior shoulder.
Step 6: Last Ditch Maneuvers
- Intentional fracture of the clavicle → Offloads clavicle from the maternal pubic ramus. Apply pressure anteriorly and superiorly away from the fetal lung.
- Zavanelli maneuver → cephalic replacement by reversing the cardinal movements of labour in preparation for emergent c-section.
- Symphysiotomy → sharp midline dissection of the pubic symphysis (if absolutely no other alternatives are available).
*** The Step 6 techniques carry significant risk of fetal and maternal morbidity but can be considered as a last resort if all else fails ***
To Episiotomy or not to Episiotomy?
An episiotomy is an elective incision of the skin to widen the perineal area. Does it help with shoulder dystocia you ask?
Well, shoulder dystocia is an obstruction of bone on bone rather than soft tissue, so routine episiotomies won’t solve the underlying problem. However, in cases of shoulder dystocia failing to resolve with the initial steps, an episiotomy may be beneficial in providing more space for the physician’s hands to perform internal or rotational maneuvers.
FYI: The medio-lateral approach is preferred over the midline approach when performing episiotomies, given the reduced risk of damage to the anal sphincter.
Take home point #2: Be able to identify signs of shoulder dystocia promptly and employ the sequence of maneuvers outlined above with help from your team and specialty colleagues.
You can remember the stepwise order of maneuvers using the following acronym:
H – call for Help
E – End maternal pushing
L – Leg hyperflexion via McRoberts maneuver
P – apply suprapubic Pressure
E – Enter internally to perform rotational maneuvers
R – Remove the posterior arm
R – Roll the patient onto all fours
OBJECTIVE 3: Managing Nuchal Cord Emergencies
How do I handle a nuchal cord during deliveries and how dangerous are they?
About 30% of deliveries will have a nuchal cord around the neck present. Although they are perceived as high-risk situations, the cord is usually loose and does not harm the infant.
- Dealing with a loosely wrapped cord → manually reduce the cord above the fetal head. If unsuccessful, you can try bringing the cord caudally over the shoulders and deliver the fetus through the cord then unwind it after delivery.
- Dealing with a tightly wrapped cord → although rare, if a tight cord cannot be reduced manually, it will require clamping and cutting as a last resort. Clamp the cord in two locations ~4cm apart followed by cutting it in between the clamps. To note, this sometimes-necessary management has been associated with serious fetal complications including: hypovolemia, anemia, shock, hypoxic-ischemic encephalopathy, cerebral palsy.
How common is cord prolapse and how do I deal with one during a delivery?
Cord prolapse is a less common presentation, only occurring in about 2-6% of deliveries. Although rarer to occur, they are much more dangerous carrying a 10% perinatal mortality rate.
- Cord prolapse with immediate caesarean section capability available:
- call for help immediately (obstetrics & pediatrics)
- instruct the mother to stop pushing
- position the stretcher in Trendelenburg with mother in a knee to chest position
- manually elevate the fetal presenting part while waiting for the OR (do not touch or replace the cord)
- Cord prolapse without caesarean section availability:
- perform a funic reduction and replace the cord gently into the uterus
- perform a rapid vaginal delivery while trying to limit the amount of cord trauma to avoid vasospasm
Take home point #3: During a delivery if you see a cord, don’t freak out! Nuchal cords around the neck are more common than we think and can be easily manually reduced over the fetal head. Don’t forget the equipment in your toolkit if you run into trouble! Cord prolapse is a rarer occurrence but if you do encounter it, call for help early as definitive management is a caesarean section and don’t touch the cord!
Check out part 2, where we will discuss the management of postpartum hemorrhage, and resuscitative hysterotomy! For the full grand rounds video, please see below.
References
- Brunette D. Prehospital and emergency department delivery: a review of eight years experience. Annals of Emergency Medicine. 1989. 18(10); 1116-1118.
- Practice Bulletin No. 183: Postpartum hemorrhage. Obstetrics and Gynecology. 2017. 130(4);e168-186.
- WOMAN trial collaborators. Effect of early tranexamic acid administration on mortality, hysterectomy, and other morbidities in women with postpartum hemorrhage (WOMAN): an international, randomised, double-blind, placebo-controlled trial. Lancet. 2017. PMID:28456509.
- Katz V, Dotters D, Droegemueller W. Perimortem cesarean delivery. Obstet Gynecol. 1986 Oct;68(4):571-6.
- Katz V, Balderston K, DeFreest M. Perimortem cesarean delivery: were our assumptions correct? Am J Obstet Gynecol. 2005 Jun;192(6):1916-20.
- Einav S, Kaufman N, Sela H. Maternal cardiac arrest and perimortem cesarean delivery: Evidence or expert-based? Resuscitation. 2012. 83; 1191-1200.
- Roberts, Custalow, Thomsen, et al. 2019. Roberts and Hedges’ Clinical Procedures in Emergency Medicine and Acute Care. 2019. 7th Elsevier.
- Borhart J, Voss K. Precipitous Labor and Emergency Department Delivery. Emergency Medicine Clinics of North America. 2019. 37; 265-276.
- Del Portal D, Horn A, Vilke G, et al. Emergency department management of shoulder dystocia. Journal of Emergency Medicine. 2014. 46(3); 3780382.
- Ferguson F, Guzman J. Cardiac arrest in special populations. Emergency Medicine Clinics of North America. 2012. 30; 169-178.
- Mercado J, Brea I, Mendez B, et al. Critical obstetric and gynecologic procedures in the emergency department. Emergency Medicine Clinics of North America. 2013. 31; 207-236.
- Rose C, Faksh A, Traynor K et al. Challenging the 4- to 5-minute rule: from perimortem cesarean to resuscitative hysterotomy. American Journal of Obstetrics and Gynecology. 2015. 2013 (5); P653.E1.
- Silver D, Sabatino F. Precipitous and Difficult Deliveries. Emergency Medicine Clinics of North America. 2012. 30; 961-975.
- WHO recommendations for the prevention and treatment of postpartum hemorrhage. 2012 Available at: http://apps.who.int/iris/bitstream/10665/75411/1/9789241548502_eng.pdf
- Photo Credit:
https://partiesideas.com/facts-about-pushing-the-baby-during-childbirth
Roberts, Custalow, Thomsen, et al. 2019. Roberts and Hedges’ Clinical Procedures in Emergency Medicine and Acute Care. 2019. 7th edition. Elsevier.

