

Equity, Diversity and Inclusion (EDI) has become an important rallying point and component of organizational structures. Recognizing the importance of equity in the social determinants of health, healthcare organizations have begun to place very specific focus on this issue.
Locally, our EDI committee has a vision statement to reflect its valuables and principles:
The Equity, Diversion and Inclusion committee in the Department of Emergency Medicine at the University of Ottawa recognizes that bias and discrimination are barriers to patients receiving appropriate and compassionate care. We seek to disseminate knowledge, develop helpful policies, and foster systems of accountability by targeting bias and discrimination in the Emergency Department to ensure that our staff are supported to provide inclusive patient centred care to our diverse patient population.
It is through this lens that earlier this year, Dr. Patrick, the CMAJ editor-in-chief defended the CMAJ publishing articles “calling for dismantling racism in Canadian healthcare and medical academia”:
I am writing today to state categorically CMAJ’s position on the matter, which is that systemic racism exists in Canadian society and within its health care systems. My purpose here is not to debate the existence of racism in Canada. Ample evidence and testimony support its existence. I invite readers to acquaint themselves with it. As CMAJ is part of the system that produces medical knowledge, it is and has been part of the problem. It is essential that we recognize how and take action to be part of the solution.
Now, after being involved in EDI work, I’ve come to appreciate how emotionally and cognitively challenging this work is. Ive also learned, it can be harder than you think to ‘get it right’.
The major reason that EDI is such a challenge in 2021, is that so many inequalities are related to implicit bias rather than explicit bias. Sure, we see openly racist incidences every day, but implicit bias often stings more – because it is felt rather than heard.
The hard part with our biases is that they often live in our blindspots, so when approaching EDI work, it is inevitable that people are sometimes going to get it wrong because of their cognitive gaps.

And in the past month, the CMAJ got it wrong. In December, CMAJ published an editorial by Dr. Sharif Emil called “Don’t use an instrument of oppression as a symbol of diversity and inclusion” in reference to a stock photo of a child wearing a hijab in their publication. It was certainly hard to find the intent behind the article, as it was incredibly islamophobic; “girls as old as those in the picture are being sold into marriage to old men — institutionalized child rape”.
Unsurprisingly, there was significant criticism against this article and CMAJ, with thoughts expressed very eloquently by others:

In response to significant backlash against the article, CMAJ apologized for their editorial process, and formally retracted the letter.
It would be pretty easy to sit here and stay mad at CMAJ because of a lack of judgement in the publishing of this article, but, that isn’t exactly the point of EDI. Equity, Diversity and Inclusion work has to have a primary focus on fostering a culture change within medicine (and the world around us). It is through this culture change and dialogue that we will foster systems of accountability. So it is important that we look at mistakes in EDI as opportunities to learn and improve, rather than focusing entirely on the criticism.
I, for one, think that Dr. Patrick and the editorial team at CMAJ did a great job in ‘sitting with their discomfort’ in the growth zone in their apology letter. As we continue to embrace EDI in healthcare, we are going to stumble and make mistakes, but the key lies in learning from these situations in order to foster change.
What is the best way to respond to (implicit or explicit) bias?
Being an EDI lead this year, this is one of the more common questions I have been asked. Recognizing that bias is happening is the first step, and developing an appropriate interpersonal response is the second (and harder) part.
1. Check yourself
You’ve heard something, or something has happened that you suspect is related to bias; the first thing is to check in with yourself (notice the I statements):
- Is this something that I have done in the past?
- Have I fallen short on this in the past?
- What is my energy level?
- How calm or angry am I?
- These are obviously normal emotions, but understanding these feelings in yourself is the first step to developing a response.
- If you recognize that the incident is very triggering for you, or you are very upset about it – it may be best to allow some time to reflect upon it and address it outside of the ‘heat of the moment’.
- If it is an issue that you have worked through, or recognized in yourself in the past, it is important to acknowledge that you have gained insights because of your reflection, and to not assume that others have done this yet.
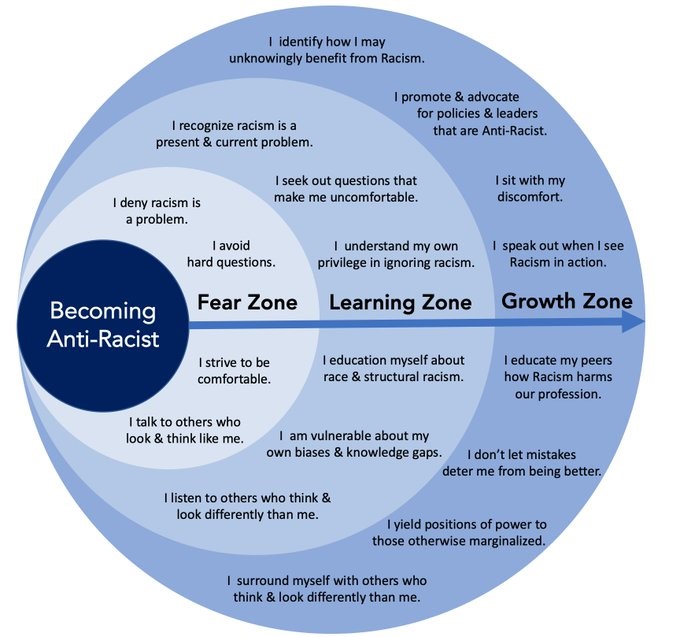
2. Where are they?
- You need to recognize where the individual is at (i.e.: whom is saying this, and why) – are they in the fear zone, learning zone or growth zone?
- Diagnosing the stage of progression where they are will help to inform the tone of the conversation
- The closer one is to the ‘fear zone’, the less effective a direct approach will be. For people in the fear zone, the best approach is to model good behaviour
- i.e.: using appropriate pronouns, addressing the patient specific concerns, etc.
- For the person in the learning zone, draw on your own experiences and use ‘I’ phrases
- i.e.: “I used to struggle with pronouns before recognizing the importance of utilizing them appropriately”
- For those in the growth zone, individuals tend to be very receptive and interested in discussing their discomfort, and the situation that occurred
- i.e.: ‘sitting with their discomfort‘
- Avoid making conclusions or judgement about a person, instead, invite that person to consider further reflection – as this is a great foundation for beginning to address an issue. Nobody likes being confronted, and we should review addressing implicit bias an an educational opportunity.
Follow up
Follow up is a component that often gets missed – consider this like a post-case debrief.
- Follow up with the person affected by the interaction
- Follow up if you engaged in an EDI discussion with somebody
- Report what is going on through formal, existing channels as appropriate
- Remember that the main focus of EDI work is fostering culture change through dialogue and open communication
