


We are back with Part-2 of our blog series on Emergency Department Deliveries. If you haven’t already, check-out Part 1 HERE. In this post, we will explore postpartum hemorrhage and resuscitative hysterotomy:
- Managing postpartum hemorrhage
- Running a maternal cardiopulmonary arrest code, while aware of the indications and steps to performing a resuscitative hysterotomy
OBJECTIVE 4: Managing Postpartum Hemorrhage
Recognition is key in the initial steps of managing postpartum hemorrhage (PPH), defined as >500 mL of blood loss during or directly following a vaginal delivery. This quantitative amount is controversial; however, given the amount of blood loss is often underestimated and can be quite subtle.
The management of PPH can be divided into 3 main components:
1) Preventative Measures
- Prevention of PPH is key!
- Promote uterine contraction by administering Oxytocin 10 units IM after delivery of the anterior shoulder (realistically this can be given after the fetus is delivered).2
- Perform uterine massage after placental delivery to promote uterine contraction and if no spontaneous delivery of the placenta within 5 minutes of fetal delivery, employ the techniques described above.
2) Resuscitation
- Once PPH is identified, act as you normally would when treating hemorrhagic shock
- Consider initiating a massive transfusion protocol
- Consider administering tranexamic acid:
- The WOMAN trial examined the effect of TXA vs. placebo in over 20,000 PPH patients3
- Despite initial misconceptions, the study concluded no significant difference in the primary outcome (composite of all-cause mortality and requirement of a hysterectomy)
- I’d like to draw your attention to one specific secondary outcome that showed a significant reduction in death from bleeding in the TXA group. This difference; however, was quite small with a fragility index of 0 (meaning if 0 patients had a different result, the outcome would be statistically non-significant)
Bottom line: How should we let this data influence our clinical decision making when dealing with PPH patients?
Given the conflicting and borderline statistics of this secondary outcome, we probably shouldn’t be administering TXA routinely in PPH patients. On the other hand, TXA is objectively a relatively safe drug, and this data demonstrates a small yet potentially important benefit. When it comes down to managing a PPH patient in hemorrhagic shock, I would still reach for it when treating these critically ill patients.
3) Treat the Underlying Cause [4 T’s]
Tone
- Uterine atony accounts for up to ~80% of PPH cases so when in doubt, try to fix this problem first!
- Presents with a soft and boggy uterus in the setting of excessive vaginal bleeding after delivery.
- Decompress the bladder with a foley to allow the uterus to contract.
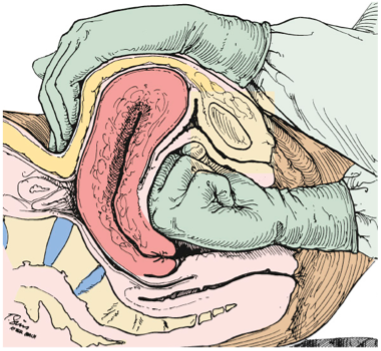
- Uterine massage should be started in a bimanual fashion.
- Start a uterotonic agent:
- Oxytocin 10 units IM (or 40 units in 1L NS; run open until the uterus is firm)
- Methylergonovine 2 mg IM
- Avoid in hypertensive and pre-eclamptic patients due to vasoconstrictive effects
- Carboprost 250 mcg IM Q15 mins up to 8 doses
- Avoid in hypertensive and asthmatic patients due to vasoconstrictive and broncho-constrictive effects
- Misoprostol 800 mcg PO/SL/PR
Tissue
- Inspect the placenta to ensure it is whole and intact.
- Remove any retained placental fragments by employing gentle manual extraction with a finger to bluntly dissect.
Trauma
- Ensure you inspect for and do not miss genital tract lacerations and hematomas.
- Lower and accessible genital tract lacerations can be managed with direct pressure and primary closure using sutures.
- Upper genital tract injuries should be managed by our obstetrics colleagues.
Thrombin
- If there is any suspicion for an inherited or acquired coagulopathy, promptly send blood work and consider resuscitating with empiric blood products
Other tips in your toolkit to consider if there is ongoing active bleeding:
- Attempt to tamponade hemorrhage using a Bakri balloon; however, this will likely be unavailable in the ED setting.
- Alternatively, a foley catheter can be inserted and instilled with saline. It is important to note that this volume will be quite small in comparison to the uterine cavity size and will likely be ineffective.
- Our obstetrical colleagues will be able to suggest and perform other management options including: uterine artery embolization, hemostatic suturing, or hysterectomy as a rare last line.
Take home point #4: Don’t fail to recognize PPH – even the most subtle ongoing bleeding post-delivery can qualify. Remember the “4 T’s” as possible underlying causes of PPH with uterine atony, by far, being the most common. Try to fix uterine tone first by utilizing the typical sequence of bladder decompression, uterine massage and uterotonic agents.
OBJECTIVE 5: Evidence and Indications to Performing a Resuscitative Hysterotomy
What is the rationale behind performing a resuscitative hysterotomy?
Fortunately, cardiopulmonary arrest is a very rare event during pregnancy, which can be precipitated by: hemorrhage, amniotic fluid embolism, heart failure, sepsis, anesthetic complications, and trauma.
Resuscitative hysterotomies have been widely accepted in obstetric and trauma literature and should be initiated within 4 minutes of the onset of an arrest (in the absence of ROSC) and considered in any patient ≥ 24 weeks gestational age (GA) who suffers a cardiac arrest.
What’s the deal with this 4-minute timeframe?
Although sufficient data is lacking regarding the optimal time to fetal delivery post-arrest, it is well-known that fetal survival drastically decreases at the 5-minute mark. Because of this, 4-minutes has become the gold standard when performing resuscitative hysterotomies and the overall procedure should be completed by 5 minutes post-arrest to optimize fetal outcomes.
- Various studies have examined multiple case reports and the associated outcomes of resuscitative hysterotomies.4,5
- These studies demonstrate high survival rates ranging from 40-75% in infants and 1/3 in mothers – which is very high in resuscitation literature!
- One newer study by Einav et al.6 reviewed resuscitative hysterotomy case reports over a 30-year period. They concluded that this 4-minute timeframe is usually not met in 93% of cases, yet neonatal survival is likely if the delivery occurs within 10-15 minutes post-arrest.
- Multiple authors have reiterated the difficulties that come with accomplishing a delivery within 5 minutes post-arrest (both in real life and simulated scenarios) because of the shift in mind-set the clinician has from resuscitating mother to then resuscitating the fetus, despite not achieving ROSC of the mother.
- Keep in mind that early delivery of the fetus may benefit the successful resuscitation of both the mother and the fetus.
Why does early delivery of the fetus increase the chances of a successful resuscitation?
Typically, chest compressions produce a cardiac output of about 1/3 of normal. In a term pregnant patient, the uterus compresses the great vessels which reduces cardiac output by 2/3. This means that in the best of circumstances, CPR results in a cardiac output of 10% of normal, also leading to compromised placental perfusion. Decompression of the IVC and abdominal aorta by removing the fetus allows for improved venous return, permitting more effective CPR.
When it comes down to it, this is a life-saving procedure so using outdated and past terminology such as “peri-mortem C-section” should be avoided as its connotation can create a mental barrier for us as clinicians.
How do I perform a Resuscitative Hysterotomy?
Remember your ABCD’S!
A – Appropriate patient selection:
- Pregnant patients ≥ 24 weeks GA with cardiopulmonary arrest, where ROSC has not been achieved within 4 minutes.
- CPR should be ongoing before and after this procedure.
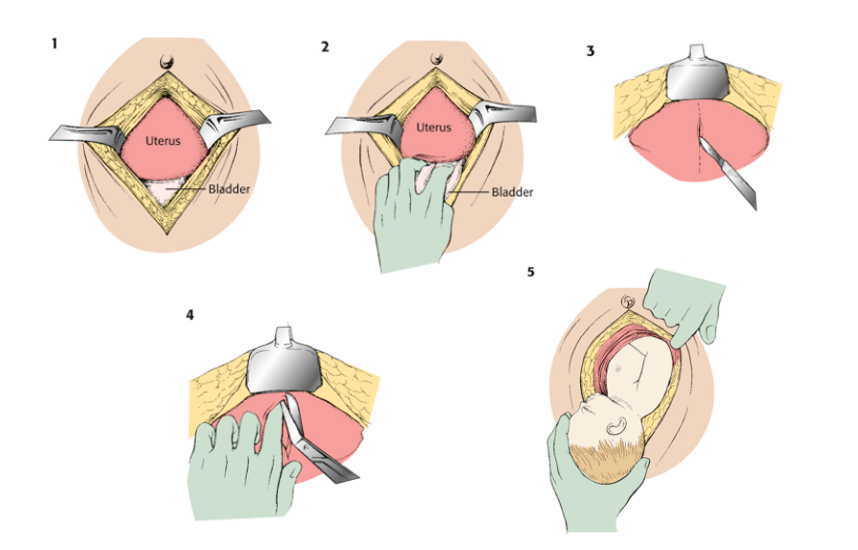
B – Bone to bone cut:
- Using 10 blade scalpel, make a midline vertical incision from the xiphoid process to the pubic symphysis through all the abdominal wall layers into the peritoneal cavity.
- Retractors can be used to expose the anterior surface of the uterus.
- Reflect the bladder inferiorly. If full, it may be decompressed through aspiration to provide better access to the uterus.
C – Cut the uterus:
- Using a scalpel, make a small (~5 cm) vertical incision into the lower aspect of the uterus until you get a big gush of amniotic fluid.
- Place your finger in the opening to keep your landmark and carefully cut the uterus with scissors toward the fundus.
- Pro tip: ensure you make an incision using your scalpel first, as the uterine muscle is thick and hard to cut through with scissors alone.
D – Deliver the baby:
- Ideally, deliver baby’s head first.
- Check the cord to ensure there’s no nuchal cord.
- Clamp and cut the cord, pass the fetus off to your colleagues, then deliver the placenta.
S – Stop the bleeding:
- Compress and pack the uterus then continue with the resuscitation.
- Call any surgical colleagues for help in managing the open abdomen.
Take home point #5: When performing a resuscitative hysterotomy in an arrested pregnant patient at least 24 weeks GA, remember the 4- and 5- minute rules – where the procedure should ideally be initiated within 4 minutes of the arrest onset and completed by 5 minutes post-arrest. Don’t forget your ABCD’S to help get you through the steps of the procedure!
Photo Credit: https://partiesideas.com/facts-about-pushing-the-baby-during-childbirth Roberts, Custalow, Thomsen, et al. 2019. Roberts and Hedges’ Clinical Procedures in Emergency Medicine and Acute Care. 2019. 7th edition. Elsevier.References

