

- Pediatric cardiac arrests are rare occurrences in Canada
- Due to the infrequency, pediatric cardiac arrest and resuscitation are challenging areas to study so the data we have is limited in scope and quality.
- This is an area for future research and improvement
- Pediatric in hospital cardiac arrests (PIHCA) outcomes have improved in recent times
- Pediatric out of hospital cardiac arrests (POHCA) outcomes remain very poor

Alexis A. Topjian. Circulation. Part 4: Pediatric Basic and Advanced Life Support: 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care, Volume: 142, Issue: 16_suppl_2, Pages: S469-S523
PALS Guideline Updates
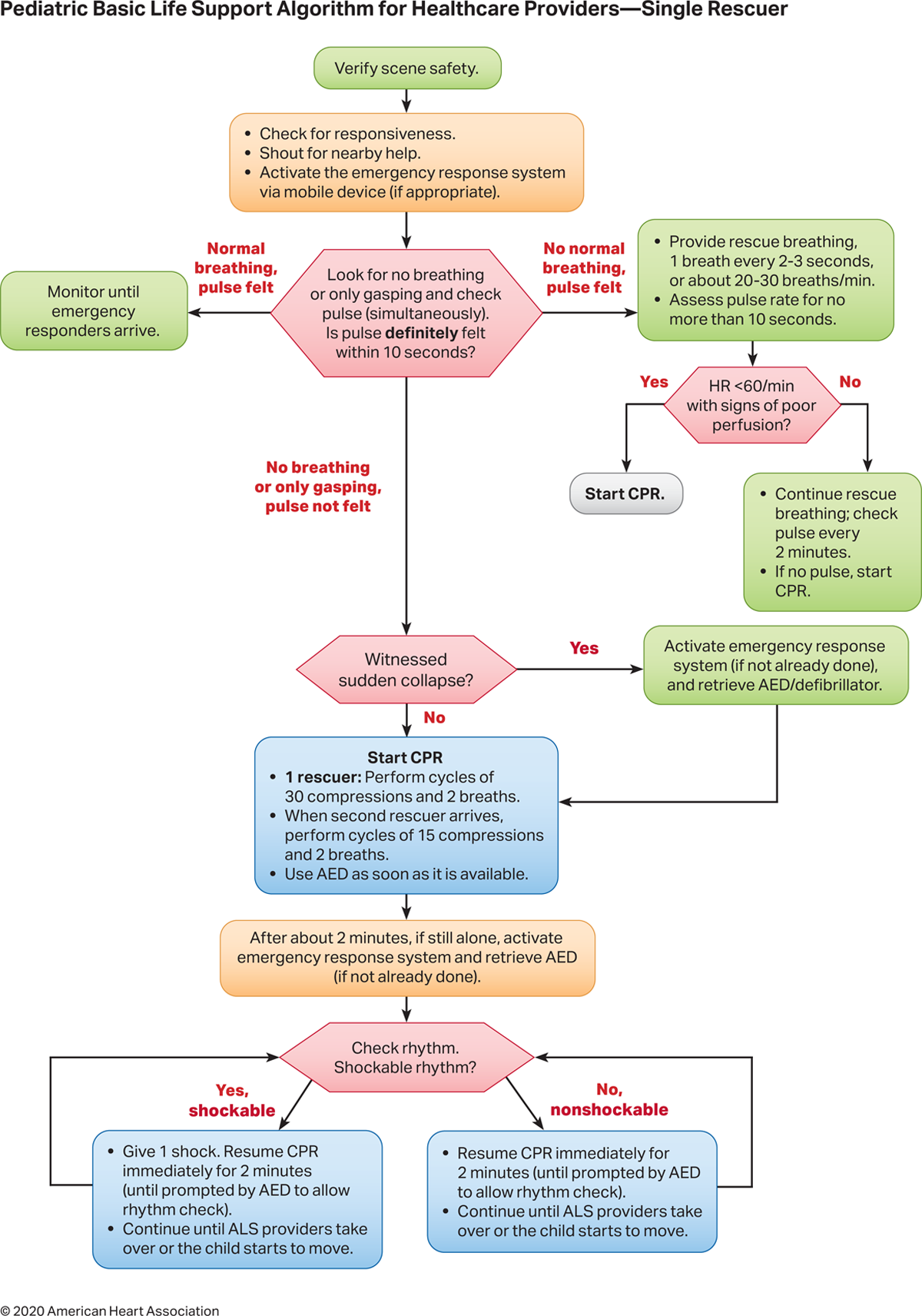
RESCUE BREATHING
2010 Previous Recommendation:
If there is a palpable pulse 60/min or greater but there is inadequate breathing, give rescue breaths at a rate of 1 breath every 3-5 seconds (12-20/min)
2020 Update:
For infants and children with a pulse but absent or inadequate respiratory effort, it is reasonable to give 1 breath every 2-3 seconds (20-30 breaths/min)
The causes of cardiac arrest in infants and children differ from those in adults, with pediatric cardiac arrests most often due to hypoxia.
HEMODYNAMIC MANAGEMENT
FLUID RESUSCITATION
2010 Previous Recommendations:
Push repeated boluses of 20ml/kg of isotonic crystalloid to treat shock
2020 Update:
In patients with septic shock, it is reasonable to administer fluids in 10-20 ml/kg aliquots with frequent reassessments
Patients who received higher fluid volumes or faster fluid resuscitation were more likely to develop clinically significant fluid overload characterized by increased rates of mechanical ventilation and worsening oxygenation
This is not a departure from liberal fluid resuscitation, it is an addition of frequent clinical reassessments for patients’ response to fluids and signs of fluid overload.
Clinical reassessments may include the use of POCUS.
VASOPRESSOR CHOICE
2010 Previous Recommendation
Titrate dopamine to treat shock that is unresponsive to fluids
2020 Update:
In infants and children with fluid refractory septic shock, it is reasonable to use epinephrine or norepinephrine as an initial vasoactive infusion
However if epinephrine or norepinephrine are unavailable, dopamine may be considered
Epinephrine is more effective than dopamine to resolve fluid-refractory hypotensive cold shock and improve organ function, within the first hour of resuscitation.
Bottom Line:
If you suspect hypovolemia or septic shock, start with 20ml/kg then reassess with subsequent fluid administration
It is reasonable to continue with 10ml/kg with reassessment of fluid responsiveness and signs of fluid overload. This may be done clinically with POCUS as an adjunct
Have a lower threshold to move to vasoactive agents if there are signs of fluid overload, preferably epinephrine or norepinephrine
AIRWAY MANAGEMENT
For more on pediatric airway management, check out this excellent grand rounds.
Endotracheal Tubes
2010 Previous Recommendation:
Both cuffed and uncuffed ETTs are acceptable for intubating infants and children. In certain circumstances (poor lung compliance) a cuffed ETT may be preferrable to an uncuffed tube, provided that attention is paid to ETT size, position and cuff inflation pressure
2020 Update:
It is reasonable to choose cuffed ETTs over uncuffed ETTs for intubating infants and children.
When a cuffed ETT is used, attention should be paid to ETT size, position, and cuff inflation pressure (<25cm H2O)
Cuffed ETTs have been shown to be safe, have a decreased need for tube changes or reintubation and decreased risk of aspiration
Subglottic stenosis is rare when cuffed ETTs are used in children and careful technique is followed.
CRICOID PRESSURE
2010 Previous Recommendation:
There is insufficient evidence to recommend routine application of cricoid pressure to prevent aspiration during endotracheal intubation in children
2020 Update:
Routine use of cricoid pressure is not recommended during endotracheal intubation of pediatric patients
Routine use of cricoid pressure is associated with decreased first pass success
Cricoid pressure does not reduce the rate of regurgitation
Bottom line:
When intubating the pediatric patient, select the appropriate cuffed tube size and have alternative sizes available, use a careful technique and avoid using cricoid pressure
Consider the use of a supraglottic airway when feasible, to decrease interruptions to high quality CPR
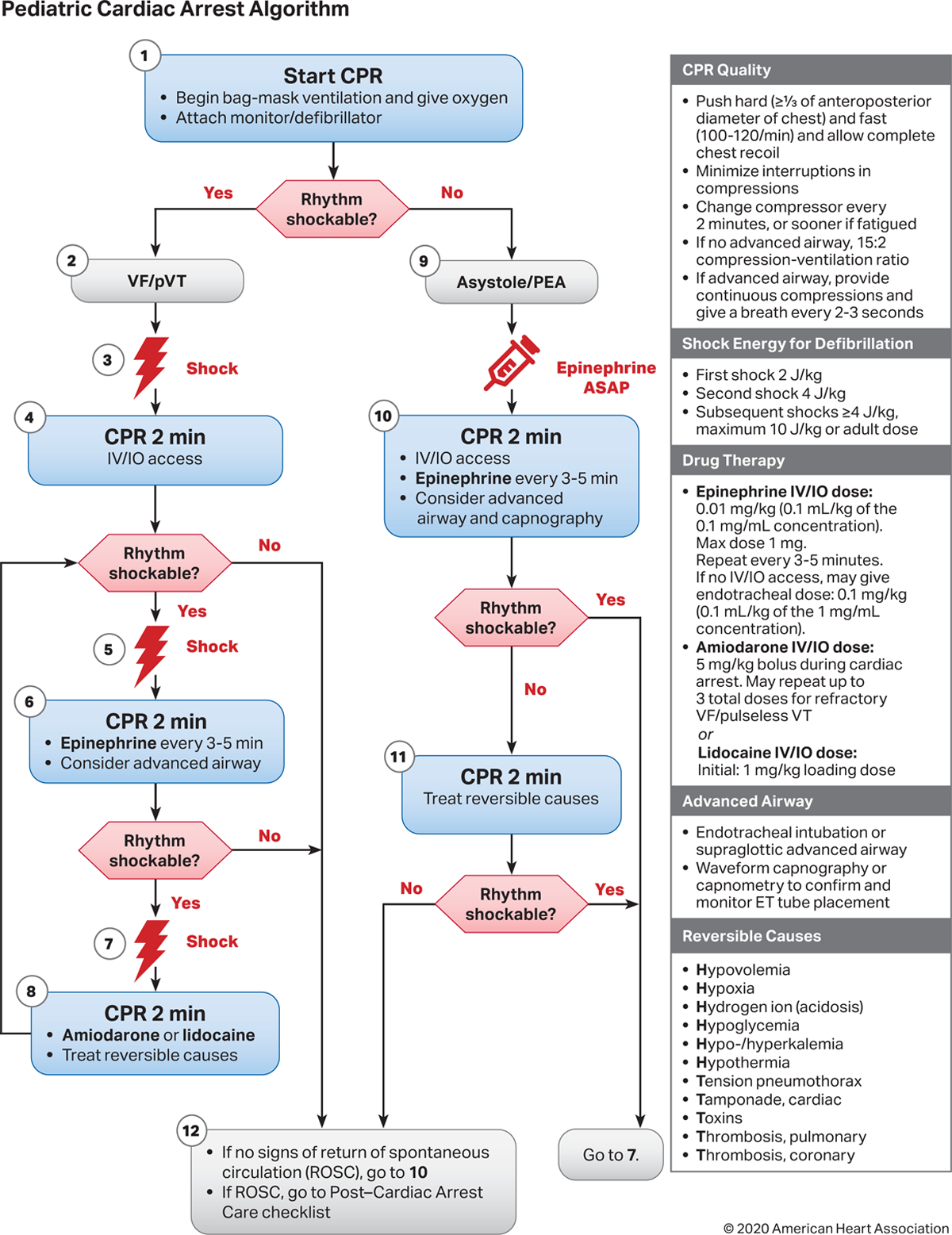
EPINEPHRINE ADMINISTRATION
2010 Previous Recommendation:
It is reasonable to administer epinephrine in pediatric cardiac arrest
2020 Update:
For pediatric patients in any setting, it is reasonable to administer the initial dose of epinephrine within 5 minutes from the start of chest compressions
Anderson et al (2015) noted that for every minute of delay in administration of epinephrine, there was a significant decrease in: ROSC, 24h survival, survival to discharge, and survival with favourable neurologic outcome (Andersen, Lars W., et al. “Time to epinephrine and survival after pediatric in-hospital cardiac arrest.” Jama 314.8 (2015): 802-810. )
Bottom line:
Establish intravenous or intraosseous access early, have a low threshold to move to intraosseous access and administration of epinephrine within the first five minutes of cardiac arrest
VENTILATION DURING CPR WITH ADVANCED AIRWAY
2010 Previous Recommendation
If the infant or child is intubated, ventilate at a rate of 1 breath every 6 seconds (10 breaths/min) without interrupting chest compressions
2020 Update
When performing CPR on infants and children with an advanced airway, it may be reasonable to target a respiratory rate of 1 breath every 2-3 seconds (20-30 breaths/min), accounting for age and clinical condition. Rates exceeding these recommendations may compromise hemodynamics.
This is a significant and controversial departure from previous recommendation.
Sutton et al conducted a single center study with recruitment over 3 years in a pediatric ICU. They included 47 patients who received at least one minute of CPR and looked at ventilation rates in PIHCA and survival outcomes. All patients were already intubated and had arterial lines, 60% had congenital cardiac defects and, of all the arrests, 74% were secondary to bradycardia with poor perfusion. During the arrest, none of the patients were ventilated according to PALS guidelines at the time while they received CPR (10 +/- 2 breaths per minute). Of note, of all of the patients with PEA/asystole, NONE survived.
The authors concluded that high ventilation rates associated with higher odds of survival to discharge.
The study supporting this guideline change is not generalizable to the ED pediatric patient, who primarily presents with out of hospital cardiac arrest, who’s presenting rhythm is predominantly PEA or asystole
We know the cause of cardiac arrest differs in pediatric patients but once the patient is in cardiac arrest, careful attention must be paid to balancing oxygenation and hemodynamics
We know that positive pressure ventilation decreases systolic blood pressure and decreases cardiac output
Pediatric patients who are already in cardiac arrest need resuscitation that balances their oxygenation, along with hemodynamics.
Assisted ventilation in the pediatric patient with a pulse, who likely has a respiratory cause of their shock, is very different than managing the pediatric patient in cardiac arrest.
ILCOR did not support this change– “The optimum ventilation rate during continuous chest compressions in children with an advanced airway is based on limited data and requires further study”
Bottom Line:
Consider the etiology of the arrest and remember that though the etiology is likely respiratory, the patient is already in circulatory collapse and you should cautiously provide mechanical ventilation and balance the need for oxygenation with supporting cardiac output.
Ventilation has to match perfusion needs.
Consider using an initial lung recruitment strategy with two “larger breaths” initially and move toward cautious ventilation while CPR is ongoing for the arrested patient
REFERENCES
Andersen, Lars W., et al. “Time to epinephrine and survival after pediatric in-hospital cardiac arrest.” Jama 314.8 (2015): 802-810.
De Orange FA, Andrade RG, Lemos A, Borges PS, Figueiroa JN, Kovatsis PG. Cuffed versus uncuffed endotracheal tubes for general anaesthesia in children aged eight years and under. Cochrane Database Syst Rev. 2017 Nov 17;11(11)
Donnino MW, Salciccioli JD, Howell MD, et al; American Heart Association’s Get With the Guidelines-Resuscitation Investigators. Time to administration of epinephrine and outcome after in-hospital cardiac arrest with non-shockable rhythms: retrospective analysis of large in-hospital data registry. BMJ. 2014;348:g3028.
Girotra S, Spertus JA, Li Y, Berg RA, Nadkarni VM, Chan PS; American Heart Association Get With the Guidelines–Resuscitation Investigators. Survival trends in pediatric in-hospital cardiac arrests: an analysis from Get With the Guidelines-Resuscitation. Circ Cardiovasc Qual Outcomes. 2013;6(1):42-49.
Kleinman ME, Chameides L, Schexnayder SM, et al. Part 14: Pediatric advanced life support: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2010;122(18)(suppl 3):S876-S908.
Kleinman ME, de Caen AR, Chameides L, et al; Pediatric Basic and Advanced Life Support Chapter Collaborators. Part 10: Pediatric basic and advanced life support: 2010 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations. Circulation. 2010;122(16)(suppl 2):S466-S515.
Kojima T, Harwayne-Gidansky I, Shenoi AN, Owen EB, Napolitano N, Rehder KJ, Adu-Darko MA, Nett ST, Spear D, Meyer K, Giuliano JS Jr, Tarquinio KM, Sanders RC Jr, Lee JH, Simon DW, Vanderford PA, Lee AY, Brown CA 3rd, Skippen PW, Breuer RK, Toedt-Pingel I, Parsons SJ, Gradidge EA, Glater LB, Culver K, Nadkarni VM, Nishisaki A; National Emergency Airway Registry for Children (NEAR4KIDS) and Pediatric Acute Lung Injury and Sepsis Investigators (PALISI). Cricoid Pressure During Induction for Tracheal Intubation in Critically Ill Children: A Report From National Emergency Airway Registry for Children. Pediatr Crit Care Med. 2018 Jun;19(6):528-537.
Nadkarni VM, Larkin GL, Peberdy MA, et al; National Registry of Cardiopulmonary Resuscitation Investigators. First documented rhythm and clinical outcome from in-hospital cardiac arrest among children and adults. JAMA. 2006;295(1):50-57.
Ortmann L, Prodhan P, Gossett J, et al; American Heart Association’s Get With the Guidelines–Resuscitation Investigators. Outcomes after in-hospital cardiac arrest in children with cardiac disease: a report from Get With the Guidelines-Resuscitation. Circulation. 2011;124(21):2329-2337.
Ramaswamy KN, Singhi S, Jayashree M, Bansal A, Nallasamy K. Double-Blind Randomized Clinical Trial Comparing Dopamine and Epinephrine in Pediatric Fluid-Refractory Hypotensive Septic Shock. Pediatr Crit Care Med. 2016 Nov;17(11):e502-e512.
Sankar J, Ismail J, Sankar MJ, C P S, Meena RS. Fluid Bolus Over 15-20 Versus 5-10 Minutes Each in the First Hour of Resuscitation in Children With Septic Shock: A Randomized Controlled Trial. Pediatr Crit Care Med. 2017 Oct;18(10):e435-e445.
Alexis A. Topjian. Circulation. Part 4: Pediatric Basic and Advanced Life Support: 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care, Volume: 142, Issue: 16_suppl_2, Pages: S469-S523
Weiss, Scott L. et al. Surviving Sepsis Campaign International Guidelines for the Management of Septic Shock and Sepsis-Associated Organ Dysfunction in Children, Pediatric Critical Care Medicine: February 2020 – Volume 21 – Issue 2 – p e52-e106
Weiss M, Dullenkopf A, Fischer JE, Keller C, Gerber AC; European Paediatric Endotracheal Intubation Study Group. Prospective randomized controlled multi-centre trial of cuffed or uncuffed endotracheal tubes in small children. Br J Anaesth. 2009 Dec;103(6):867-73. doi: 10.1093/bja/aep290. Epub 2009 Nov 3.
Wolfe HA, Morgan RW, Zhang B, Topjian AA, Fink EL, Berg RA, Nadkarni VM, Nishisaki A, Mensinger J, Sutton RM; American Heart Association’s Get With the Guidelines-Resuscitation Investigator. Deviations from AHA guidelines during pediatric cardiopulmonary resuscitation are associated with decreased event survival. Resuscitation. 2020 Apr;149:89-99. doi: 10.1016/j.resuscitation.2020.01.035. Epub 2020 Feb 11. PMID: 32057946.
