
What is patient safety?
- Patient safety is a discipline developed in response to the rise in hospital adverse events over the years.
- Aims to take lessons learned from prior unfavourable outcomes and make improvements that mitigate risks, prevent errors, and reduce harm.
- The World Health Organization (WHO) recognizes patient safety as a global health priority
- Patient Safety allows us to evolve alongside our increasingly complex health care system.
How does harm occur?
- There are multiple factors that contribute to an adverse event as demonstrated in what’s known as the “Swiss Cheese” model of accident causation1.
- Each layer or slice of cheese in Figure 1 represents a barrier against an adverse event2.
- Each layer of security has areas of weakness illustrated by holes in the slices.
- A failure event happens when these areas align and cause a breakdown of the entire system.
- The Swiss Cheese model shows that each weak point is in fact an opportunity for intervention and improvement.
- Discovering where these gaps in defences against medical errors occur is key to quality improvement.
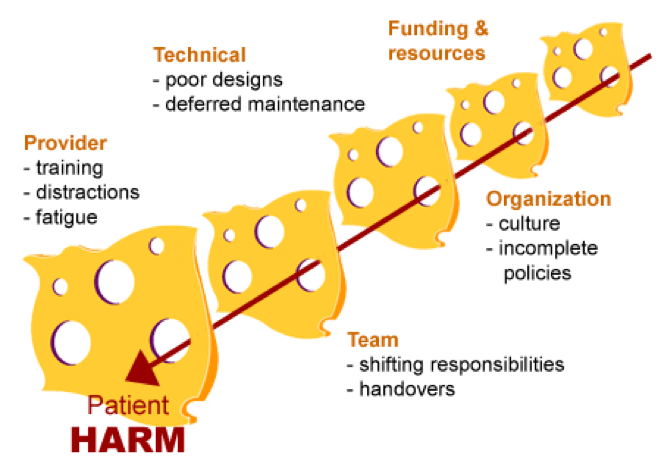
Figure 1. The Swiss Cheese model of accident causation. Adapted from CMPA, 2019.
A framework for organizing patient safety ideas
- A framework based on research priorities for patient safety in Emergency Medicine established by Plint et al in 2015 helps to organize patient safety ideas and facilitate future discussion about patient safety problems3.
- There are four key themes:
- Identification of patient safety issues
- Understanding human and environmental factors related to patient safety
- The patient’s perspective in patient safety
- Interventions for improving patient safety
Identifying Patient Safety Issues
The willingness of employees to share experiences learned from unfavourable outcomes depends significantly on the culture of the organization within which they work.
A safety culture:
- Recognizes that mistakes are inevitable for individuals working in such a complex and high-stress environment
- takes a non-punitive and fair stance when handling incidents.
This approach shifts the focus away from a culture of blame and instead towards creating an error-proof healthcare environment that will safeguard against adverse events that can harm patients.
How do you identify patient safety issues?
- Retrospectively through voluntary reporting
- Prospectively, through algorithms that predict the likelihood of an adverse event
Commonly, reporting of events in medical institutions is done through a Safety Learning System (SLS), which enables safety events, near misses, and potentially unsafe events to be electronically recorded, investigated, and managed. Everyone working in the institution is encouraged to use this system. All incidents are reviewed by a quality improvement team who will take actions to address each issue accordingly and employ preventative measures.
Electronic medical records provide novel trigger tools to identify and measure the rate of adverse events over time.
For example:
- A patient’s blood work shows a high International Normalized Ratio (INR)
- This triggers a warning for a potentially major bleeding event
- The healthcare team is prompted to determine the cause and provide treatment as needed to prevent such an event from happening in the first place
While promoting patient safety culture is an overarching goal of the healthcare system, successful uptake is dependent on adoption at the level of individual units. Work is needed to measure safety culture in the Emergency Department (ED) and to determine ways to empower people to share their experiences so that others can learn from them. Future research is also needed to broaden the approaches to identifying patient safety issues and preventing adverse events.
Understanding human and environmental factors
What is a human factor?
- Human factor is a discipline that studies the way in which individuals interact with their surroundings and with one another in their work environment with the goal of understanding human limitation and limiting risks.
- Human factor identifies ways to leverage technology to reduce human errors and help providers give better health care
- Using evidence-based approaches, experts design ways to make it easier to perform tasks like,
- ordering correct medications with appropriate doses,
- handing over patient cases without missing important information,
- organizing workflows to achieve the most efficient care in the ED.
- human factor principles can be applied to streamline care and avert adverse patient events.
What is an environmental factor?
- Environmental factor focuses on building a workspace designed for the best possible patient outcomes.
- Examples of how environmental factor can impact patient care include:
- Ideal placement of alcohol rub dispensers to reduce rates of hospital acquired infections.
- A workspace design that minimizes sound and noise, reduces interruptions and distractions, and has optimal lighting for visual tasks
- Development of acuity-adaptable rooms that remove the need to transfer patients to higher acuity areas if their condition changes
- Overall, a better understanding of how to optimally design the physical space can also contribute significantly to better and safer care.
The patient’s perspective
Why is patient perspective important?:
- Comparatively, research on how to improve patient engagement in healthcare quality is less well known relative to other areas of quality improvement and patient safety.
- This is surprising since direct patient contact and patient care are a priority in emergency medicine.
- Partnering with patients and their families shows them that their insights and experiences are valued, which in turn empowers them to take a more active role in their care.
- Moreover, patient engagement gives the opportunity to learn from their point of view what needs change within the organization.
Patient stories and feedback is often shared in quality team meetings. Themes from a complaint perspective are identified and important data generated from the feedback helps to determine areas needing improvement and set the stage for new standards.
Patient feedback is often collected but more ways are needed to incorporate them in meaningful ways. It is important to also focus energy on strengthening connections and collaborations between patients and the ED.
Interventions for improving patient safety
Morbidity and Mortality (M&M) rounds:
- M&M rounds have stood the test of time as a way for healthcare professionals to learn from one another about medical mistakes and near misses.
- The structure of M&M rounds is carefully designed and cases are specifically selected to ensure that they will teach the audience key points about cognitive biases and/or system issues that lead to harm5.
- (Click here to check out the Ottawa M&M Model)
Handovers and transitions of care
- Research has shown that using standardized ways to facilitate these processes can mitigate risks and reduce harm6.
- This tool prevents crucial information like management details, investigations and disposition from being missed during exchange of patient information between shifts.
- One tool that helps to reduce ED bounce backs is discharge templates, which include clear directions for patients on medical treatments and give specific instructions on when to return to the ED.
Checklists:
- Checklists have been used successfully in various areas of medicine.
- In the ICU, checklists helped to reduce rates of central line infections by 66%7.
- Surgical and anesthesia safety checklists have also been shown to decrease both morbidity and mortality, and are associated with cost savings and improved communication among team members.
- Checklists are effective because they allow complex medical procedures to be simplified to stepwise components and avoids the need to completely rely on human memory to recall important information in high stress situations.
Overall, although multiple tools currently exist to help improve patient safety, much more research is needed to ensure seamless and safe care in the ED.
References
- Reason J. (2000). Human error: models and management. BMJ (Clinical research ed.), 320(7237), 768–770. https://doi.org/10.1136/bmj.320.7237.768
- What is “systems thinking”. CMPA Good Practices Guide – What is “systems thinking”. (n.d.). Retrieved May 9, 2022, from https://www.cmpa-acpm.ca/serve/docs/ela/goodpracticesguide/pages/patient_safety/Systems/systems_thinking_2-e.html
- Plint, A. C., Stang, A. S., Calder, L. A., & Priorities in Patient Safety Research in Emergency Medicine Consensus Panel (2015). Establishing research priorities for patient safety in emergency medicine: a multidisciplinary consensus panel. International journal of emergency medicine, 8, 1. https://doi.org/10.1186/s12245-014-0049-9
- Griffey, R. T., Schneider, R. M., & Todorov, A. A. (2020). The Emergency Department Trigger Tool: A Novel Approach to Screening for Quality and Safety Events. Annals of emergency medicine, 76(2), 230–240. https://doi.org/10.1016/j.annemergmed.2019.07.032
- Kwok, E., Calder, L. A., Barlow-Krelina, E., Mackie, C., Seely, A., Cwinn, A. A., Worthington, J. R., & Frank, J. R. (2017). Implementation of a structured hospital-wide morbidity and mortality rounds model. BMJ quality & safety, 26(6), 439–448. https://doi.org/10.1136/bmjqs-2016-005459
- Kwok, E., Clapham, G., White, S., Austin, M., & Calder, L. A. (2020). Development and implementation of a standardised emergency department intershift handover tool to improve physician communication. BMJ open quality, 9(1), e000780. https://doi.org/10.1136/bmjoq-2019-000780
- Pronovost, P., Needham, D., Berenholtz, S., Sinopoli, D., Chu, H., Cosgrove, S., Sexton, B., Hyzy, R., Welsh, R., Roth, G., Bander, J., Kepros, J., & Goeschel, C. (2006). An intervention to decrease catheter-related bloodstream infections in the ICU. The New England journal of medicine, 355(26), 2725–2732. https://doi.org/10.1056/NEJMoa061115
