

In PART 1 of our HIV in the ED Blog series, we explored the importance of diagnosing HIV in the ED, and the approach to the diagnosis.
In PART 2, we hope to address the following:
-
- Indications for occupation & non-occupational post-exposure prophylaxis (PEP)
- Indications & resources for pre-exposure prophylaxis (PrEP)
- Barriers to patient engagement and ways we can overcome them
Post-Exposure & Pre-Exposure Prophylaxis
Post-Exposure Prophylaxis (PEP)
There is a limited scope of responsibility in which the emergency physician would prescribe antiretroviral therapy. One is in the form of PEP, in both occupational and non-occupational exposures. Institutions have location-specific algorithms, but at The Ottawa Hospital, our PEP protocol is related to blood/body fluid exposure (most commonly needle-stick injuries), and is a streamlined process initiated at triage.
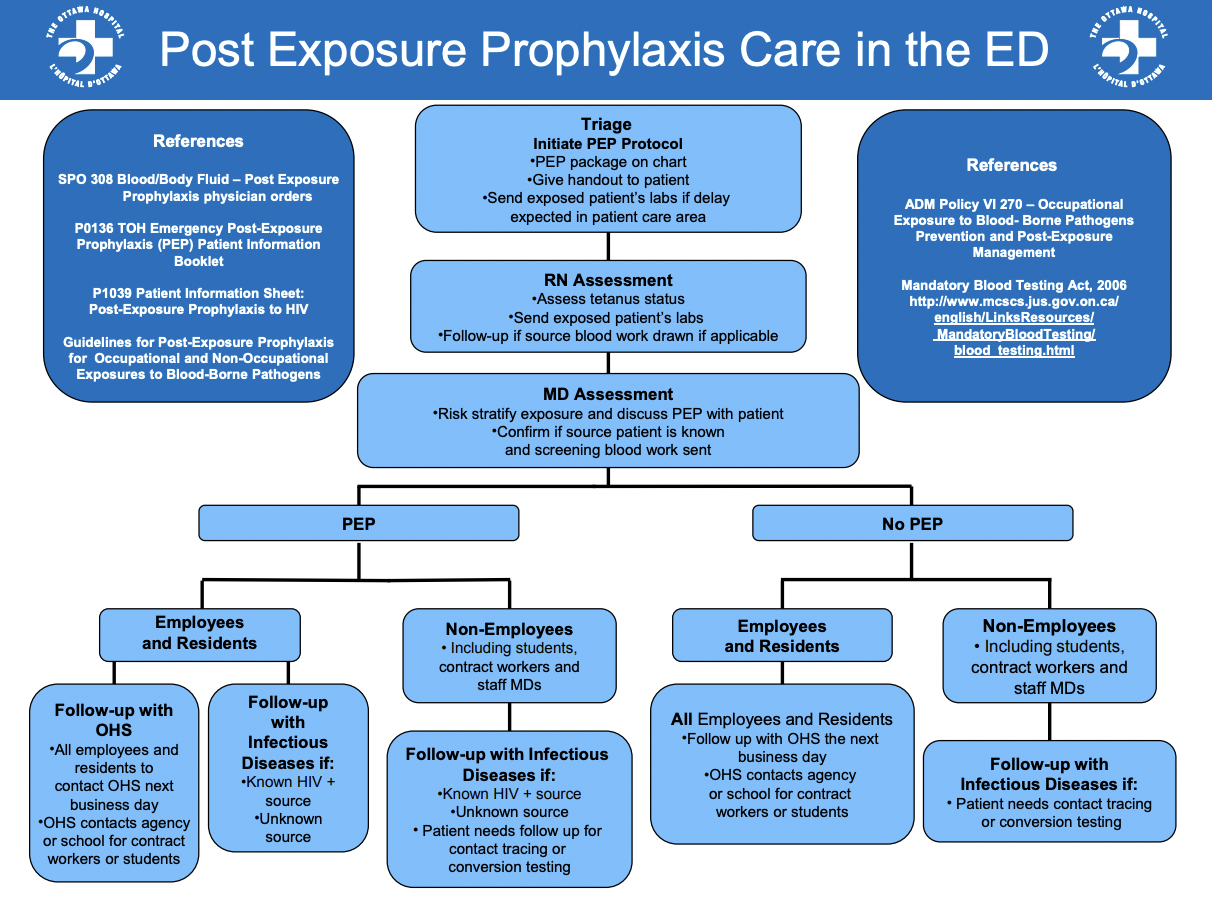
The exposed person’s labs are sent using TOH serology forms and procurement of the source person’s status is obtained via our care facilitator corresponding with the other unit care facilitator.
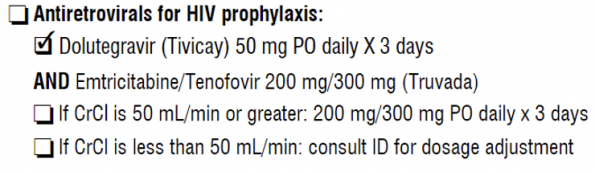
The MD then assesses the patient’s risk and, with patient consent, offers a 3-8 day course of ART in the form of Tivicay (dolutegravir), an integrase inhibitor, and Truvada (emtricitabine + tenofovir), a combination of two nucleoside reverse-transcriptase inhibitors. This will then be renewed to span a total of 28 days after being seen in follow up.
As a suggested alternative, a 2022 study by Mayer et al. revealed that Biktarvy (combined bictegravir, emtricitabine, and tenofovir), was found to be very well tolerated when used for PEP and has been proven to be very effective for treatment of confirmed HIV infection.
Some common side effects of PEP include: nausea & vomiting (15%), fatigue (10%), and diarrhea/loose stools (8%). Some patients also report lightheadedness. It’s important to point to your patients that these sides effects are typically present near the initiation of PEP, and will most often decrease or disappear after 1-2 weeks of continued use.
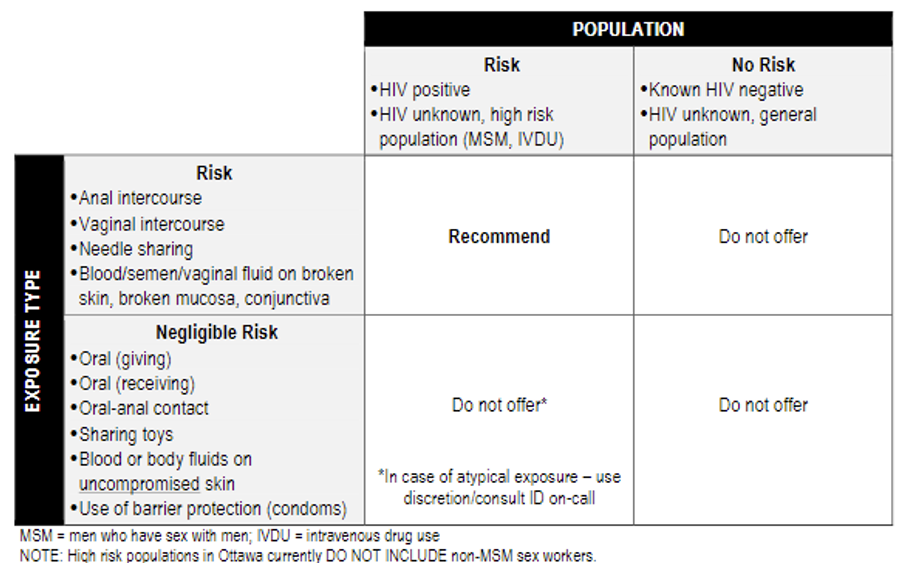
Non-occupational exposures (i.e., for non-hospital-related exposures) occur via sexual contact, needle sharing, or blood/semen/vaginal fluid exposure to broken skin, mucosa, or conjunctiva. As assessment between the patient and MD serves to determine whether their exposure was higher-risk. Should PEP be indicated, the same regimen of medications is used and an outpatient referral to infectious disease is initiated.
Those that are not initiated on PEP should be given reassurance and advised to follow up with their primary care provider or a sexual health clinic for screening once they reach the appropriate seroconversion window. As per PHAC’s PrEP and PEP fact sheet, appropriate initiation of PEP can reduce the risk of HIV infection by more than 80%.
Pre-Exposure Prophylaxis (PrEP)
UNAIDS data showed a steady increase in PrEP use since its inception, with approximately 845,000 people in 54 countries having received it in 2020. One of the more important studies, the l’Actuel PrEP Cohort, initiated in 2013 in Montreal, has greatly contributed to the data regarding its efficacy in Canada. The study was open to all adults over 18 years who were seeking PrEP and over a period of 5 years, 1551 patients initiated PrEP care and were provided periodic follow-up appointments to monitor for adherence and provide additional support. Of those who initiated PrEP treatment, 98% were cisgender males and 97% identified as homosexual or bisexual.
Unfortunately, this study experienced significant loss to follow-up over time and were only able to draw vague conclusions as to the reason. But for those that initiated and adhered to PrEP across 1637 person-years of follow-up, there were no new HIV infections were detected. According to the Ontario HIV Treatment Network, there were approximately 9600 patients started on PrEP in 2019 alone, with Toronto and Ottawa contributing to 60% of all prescriptions. And while these were either prescribed by a primary care provider or an infectious disease specialist, we as emergency physicians have a role to play as well. While we are not yet at the point of being ready to prescribe these medications ourselves, we should prepare mentally that this could possibly become a reality as it becomes more prevalent.
The Canadian guidelines – last updated in 2018 – recommend PrEP for the following:
-
- Strong Recommendations for
- men who have sex with men (MSM) and transgender women who report condomless anal sex within the last 6 months AND one of the following:
- ongoing relationship with an HIV-positive partner with risk for transmission
- 1 or more incidences requiring PEP
- history of syphilis or rectal bacterial STI within 12 months
- HIV Incidence Risk Index for MSM > 11
- HIV-negative partners in serodifferent relationships
- men who have sex with men (MSM) and transgender women who report condomless anal sex within the last 6 months AND one of the following:
- Strong Recommendation against
- individuals in stable sexually-monogamous relations with no or negligible HIV transmission risk
- Weak recommendation for
- patients engaging in needle sharing with a partner who has non-negligible risk of HIV
- Strong Recommendations for
The guidelines currently strongly recommend the combination pill Truvada, which, as you will recall, is the second component of the medications we would prescribe for PEP. These tablets can also be taken “on demand”: 2 pills 2-24 hours before first sexual exposure and 1 pill daily up to 48 hours after. According to PHAC, PrEP reduces the transmission rate of HIV by over 90% and according to another study, has a NNT of 13. That being said, if someone taking PrEP presents to our ED with an acute retroviral syndrome or are requesting HIV testing, we should assess them and initiate testing as if they were not taking PrEP. PrEP should not be taken by anyone with active HIV and should be discontinued if a patient acquires HIV while on PrEP. This is because NRTIs alone are not sufficient for the treatment of confirmed HIV, and this could contribute to resistance, significantly limiting future regimen options for the patient.
Those requesting PrEP can be directed either to their primary care provider, a local sexual health clinic, or you can refer them to comprehensive virtual services that are competent in providing safe care to the 2SLGBTQ+ community:
- The PrEP Clinic (a.k.a, the Ontario Prevention Clinic) can be contacted via phone, text, or email. They have physical sites in Toronto, Brampton, and Ottawa. The clinic is run by nurse practitioners and other allied health and have been around since 2019. Their 4-step approach is very simple to follow for anyone engaging with the service.
- Freddie is a Canada-wide service that functions the same way as the Ontario Prevention Clinic but provides access to physicians in addition to nursing and allied health staff. Both of these services ensure discreet delivery of medications to the patient’s home.
- Rocket Doctor also has an online PrEP pathway for Ontario patients.
Other accessible health centres for those seeking PrEP include:
- Toronto: HQ, Hassle Free, Safer Six, Maple Leaf Medical Clinic.
- Ottawa: Gay Zone, OPH Sexual Health Clinic, University of Ottawa Health Services, MAX Ottawa Suburban Outreach Program, Sandy Hill CHC Oasis Program, TOH PrEP Telemedicine Clinic.
The Ontario HIV Treatment Network’s Ontario PrEP webpage is also great for helping direct patients and providers alike to location-specific providers for PrEP initiation.
Unfortunately, there are many barriers that prevent a patient from seeking counsel regarding HIV testing and treatment. A 2015 literature review identified several barriers both for patients and providers as well as implementations that might facilitate engagement.
For patients
-
- Lack of perceived risk
- Comfort discussing sexual practices and lack of knowledge about HIV
- Fear of stigma or discrimination
- Lack of access to testing
- Historical precedent of medical violence
For providers
-
- Lack of perceived risk
- Comfort discussing sexual practices and lack of knowledge about HIV
- Perceived lack of time for testing or appropriate counselling
- Financial and human resource constraints
- Discriminatory views towards those who are queer, trans, involved in sex work, and/or use substances.
To ensure adequate care for our patients, we should normalize testing and provide patient education to optimize knowledge and awareness. An alternative that has been attempted in large cities, like Vancouver BC, is the opt-out method in which patients admitted to hospital would be tested routinely unless refused by the patient and the ED was encouraged to test everyone for which they suspected HIV infection. With this initiative there was an increase in testing from 0.4% to 7.2% and continues to remain high. Over the 4-year period, there were 68 new diagnoses through the ED just at the 3 sites, representing an increase from 0 to 2 diagnoses per 1000 tests.
TAKE HOME POINTS
-
- We should be able to recognize both acute retroviral syndrome and opportunistic infections.
- Anyone requesting an HIV test should receive a test.
- When a HIV-positive patient requires admission, consider sending CD4 count and HIV viral load to help our in-patient colleagues.
- EDs are the front line of initiating PEP, of which the most common regimen is a combination of Truvada & Tivicay for a total of 28 days.
- Lastly, be a champion for PrEP. Even if we are not offering it in our department right now, there are easily-accessible resources we can provide our patients and we can, at the same time, encourage safer sex practices for those inquiring.
References:
- Ahmed S, Autrey J, Katz IT, et al. Why do people living with HIV not initiate treatment? A systematic review of qualitative evidence from low- and middle-income countries. Social Science & Medicine. 2018;213:72-84. doi:10.1016/j.socscimed.2018.05.048
- Buchacz K, Armon C, Palella FJ, et al. The HIV Outpatient Study—25 Years of HIV Patient Care and Epidemiologic Research. Open Forum Infectious Diseases. 2020;7(5):ofaa123. doi:10.1093/ofid/ofaa123
- Centre for Infectious Disease Prevention and Control (Canada) PHA of C. HIV Transmission Risk: A Summary of the Evidence. Public Health Agency of Canada; 2013. Accessed July 27, 2022. http://epe.lac-bac.gc.ca/100/201/301/weekly_checklist/2013/internet/w13-16-U-E.html/collections/collection_2013/aspc-phac/HP40-78-2012-eng.pdf
- Cillóniz C, Dominedò C, Álvarez-Martínez MJ, et al. Pneumocystis pneumonia in the twenty-first century: HIV-infected versus HIV-uninfected patients. Expert Review of Anti-infective Therapy. 2019;17(10):787-801. doi:10.1080/14787210.2019.1671823
- Cohen MS, Chen YQ, McCauley M, et al. Antiretroviral Therapy for the Prevention of HIV-1 Transmission. N Engl J Med. 2016;375(9):830-839. doi:10.1056/NEJMoa1600693
- Greenwald ZR, Maheu-Giroux M, Szabo J, et al. Cohort profile: l’Actuel Pre-Exposure Prophylaxis (PrEP) Cohort study in Montreal, Canada. BMJ Open. 2019;9(6):e028768. doi:10.1136/bmjopen-2018-028768
- Gustafson R, Demlow SE, Nathoo A, et al. Routine HIV testing in acute care hospitals: Changing practice to curb a local HIV epidemic in Vancouver, BC. Preventive Medicine. 2020;137:106132. doi:10.1016/j.ypmed.2020.106132
- Haddad N, Robert A, Weeks A, Popovic N, Siu W, Archibald C. HIV in Canada—Surveillance Report, 2018. CCDR. 2019;45(12):304-312. doi:10.14745/ccdr.v45i12a01
- Haddad N, Weeks A, Robert A, Totten S. HIV in Canada—surveillance report, 2019. CCDR. 2021;47(1):77-86. doi:10.14745/ccdr.v47i01a11
- Hecht FM, Busch MP, Rawal B, et al. Use of laboratory tests and clinical symptoms for identification of primary HIV infection: AIDS. 2002;16(8):1119-1129. doi:10.1097/00002030-200205240-00005
- Macías J, Téllez F, Rivero-Juárez A, et al. Early emergence of opportunistic infections after starting direct-acting antiviral drugs in HIV/HCV-coinfected patients. J Viral Hepat. 2019;26(1):48-54. doi:10.1111/jvh.13003
- Mayer KH, Gelman M, Holmes J, Kraft J, Melbourne K, Mimiaga MJ. Safety and Tolerability of Once Daily Coformulated Bictegravir, Emtricitabine, and Tenofovir Alafenamide for Postexposure Prophylaxis After Sexual Exposure. JAIDS Journal of Acquired Immune Deficiency Syndromes. 2022;90(1):27-32. doi:10.1097/QAI.0000000000002912
- McKenna M. HIV testing: Should the emergency department take part? Annals of Emergency Medicine. 2007;49(2):190-192. doi:10.1016/j.annemergmed.2006.12.008
- Popovic N, Yang Q, Archibald C. Trends in HIV pre-exposure prophylaxis use in eight Canadian provinces, 2014–2018. CCDR. 2021;47(56):251-258. doi:10.14745/ccdr.v47i56a02
- Public Health Agency of Canada. HIV Factsheet: Biomedical Prevention of HIV : PrEP and PEP.; 2019. Accessed July 27, 2022. http://publications.gc.ca/collections/collection_2020/aspc-phac/HP40-238-2019-eng.pdf
- Public Health Agency of Canada. Estimates of HIV Incidence, Prevalence and Canada’s Progress on Meeting the 90-90-90 HIV Targets, 2018.; 2020. Accessed July 27, 2022. https://epe.lac-bac.gc.ca/100/201/301/weekly_acquisitions_list-ef/2021/21-09/publications.gc.ca/collections/collection_2021/aspc-phac/HP40-282-2018-eng.pdf
- Rodger AJ, Cambiano V, Bruun T, et al. Sexual Activity Without Condoms and Risk of HIV Transmission in Serodifferent Couples When the HIV-Positive Partner Is Using Suppressive Antiretroviral Therapy. JAMA. 2016;316(2):171. doi:10.1001/jama.2016.5148
- Rodger AJ, Cambiano V, Bruun T, et al. Risk of HIV transmission through condomless sex in serodifferent gay couples with the HIV-positive partner taking suppressive antiretroviral therapy (PARTNER): final results of a multicentre, prospective, observational study. The Lancet. 2019;393(10189):2428-2438. doi:10.1016/S0140-6736(19)30418-0
- Smith MK, Rutstein SE, Powers KA, et al. The Detection and Management of Early HIV Infection: A Clinical and Public Health Emergency. JAIDS Journal of Acquired Immune Deficiency Syndromes. 2013;63(Supplement 2):S187-S199. doi:10.1097/QAI.0b013e31829871e0
- Spagnolello O, Gallagher B, Lone N, Ceccarelli G, D’Ettorre G, Reed MJ. The Role of Targeted HIV Screening in the Emergency Department: A Scoping Review. CHR. 2021;19(2):106-120. doi:10.2174/1570162X18666201123113905
- Stanley K, Lora M, Merjavy S, et al. HIV Prevention and Treatment: The Evolving Role of the Emergency Department. Annals of Emergency Medicine. 2017;70(4):562-572.e3. doi:10.1016/j.annemergmed.2017.01.018
- Steen R, Elvira Wi T, Kamali A, Ndowa F. Control of sexually transmitted infections and prevention of HIV transmission: mending a fractured paradigm. Bull World Health Org. 2009;87(11):858-865. doi:10.2471/BLT.08.059212
- Tan DHS, MHSc MWH, BScPhm DY, et al. Canadian guideline on HIV pre-exposure prophylaxis and nonoccupational postexposure prophylaxis. 2017;189(47):11.
- Tan DHS, MHSc MWH, BScPhm DY, et al. Canadian guideline on HIV pre-exposure prophylaxis and nonoccupational postexposure prophylaxis. 2017;189(47):11.
- Traversy G, Austin T, Ha S, Timmerman K, Gale-Rowe M. An overview of recent evidence on barriers and facilitators to HIV testing. CCDR. 2015;(41):304-321. doi:10.14745/ccdr.v41i12a02
- White DAE, Giordano TP, Pasalar S, et al. Acute HIV Discovered During Routine HIV Screening With HIV Antigen-Antibody Combination Tests in 9 US Emergency Departments. Annals of Emergency Medicine. 2018;72(1):29-40.e2. doi:10.1016/j.annemergmed.2017.11.027
- 90-90-90: An ambitious treatment target to help end the AIDS epidemic.
- A Guide for the Healthcare Professional: DISCUSSING SEXUAL HEALTH with Your Patients. :6.
- A Guide to Taking a Sexual History
- HIV Pre-Exposure Prophylaxis CLINIC TELEMEDICINE QUICK REFERENCE PROTOCOL.

