

It’s time for another BHP Corner! This quarterly submission by the Base Hospital Physician Group for the RPPEO , aims to discuss topics specific to prehospital settings to educate paramedics and other healthcare providers interested in PTM on the realities of their management in this setting. Up this time – Atrial Fibrillation.
If you came to this post looking for AFib/AFlutter Best Practices, make sure to check-out the post by Dr. Pascale King, on this very same topic, by pressing HERE.
Atrial Fibrillation
Atrial Fibrillation is a common condition that paramedics encounter. Most of the time it is not the reason for the 911 call but gets identified coincidentally during your vital signs assessment and cardiac monitoring. For patients in whom the diagnosis hasn’t yet been made, this is critical information for them to be aware of and to share with their primary health provider. Appropriate anticoagulation prevents stroke and saves many people from devastating and deadly strokes every year. Long term stroke risk is the biggest concern with atrial fibrillation, and it rarely causes an acute medical emergency for the paramedic to address. When patients are unstable, rapidly transport them to the hospital and treat secondary causes of tachycardia. With this knowledge you can play a role in preventing death and disability in your community.
The Condition
Atrial fibrillation is the most common non-sinus arrhythmia that is encountered by paramedics (1). Approximately 200,000 Canadians have this condition, meaning on any given day there are tens of thousands of people walking around with atrial fibrillation, most of whom are asymptomatic (2). The most common risk factor for developing atrial fibrillation is age, meaning paramedics will increasingly see patients with this condition as our population lives longer and gets older. Atrial flutter is a similar condition and comes with the same risks and is treated the same way as atrial fibrillation.
The Risk
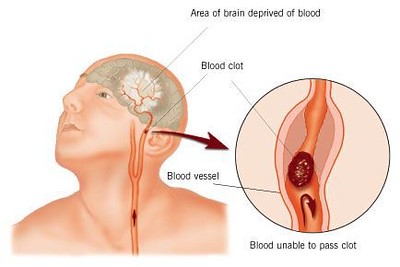
While atrial fibrillation on its own is rarely serious or immediately life-threatening, even at rapid rates, it is a major risk factor for ischemic stroke (3). The reason for this is the disorganized activity of the atria precludes the coordinate contraction of atrial systole, consequently, blood to pool in the atria and increases the risk of clot formation. Blood clots in the atria can then travel to the left ventricle and be pumped through the systemic circulation and cause arterial embolic phenomenon, most commonly affecting the brain, which leads to ischemic stroke. This makes stroke the most dangerous complication of atrial fibrillation, which of course can be disabling and even deadly.
It’s estimated that patients with atrial fibrillation are up to 5 times more likely to have a stroke than those without the condition (5), and there is anywhere from a 1-20% risk of stroke annually for patients with untreated atrial fibrillation (4). The risk is increased in patients who are older, have high blood pressure, diabetes, congestive heart failure, a previous stroke or TIA, and with increasing age. Unfortunately, the stroke risk holds true even if the patient only has paroxysmal atrial fibrillation and spends much of their time in sinus rhythm.
Stroke Prevention
Fortunately, the risk of stroke with atrial fibrillation is modifiable with modern medicine. Anticoagulation with medications like warfarin, and newer novel oral anticoagulants (NOACs) such as dabigatran (Pradaxa), rivaroxaban (Xarelto), apixaban (Eliquis), and edoxaban (Lixiana( have been shown to reduce the risk of ischemic stroke by 70-80% (2). One older but practice changing study demonstrated a reduction of risk of ischemic stroke from 4.5% annually to 1.4% with anticoagulation (5).
The Importance for Paramedics
Why is this important for paramedics to understand?
While atrial fibrillation might be the reason for the 911 call and transport to hospital when it causes palpitations, chest pain and shortness of breath, it will often be identified co-incidental to the reason for the 911 call. Many patients in whom you identify this condition will not previously have the diagnosis and given the ongoing risk of ischemic stroke associated with this condition, and our ability to modify this risk with medication, this represents an important opportunity for prevention of serious morbidity and mortality. As alternate dispositions including discharge from the scene become more common, this issue becomes even more consequential.
If you identify atrial fibrillation in your patient, make sure the strip is recorded. This documents the diagnosis. The next step is to inform the patient of the condition they have, and if they have no previous diagnosis of this or aren’t sure, they should be advised to speak with their primary health care provider, emergency physician, or other health care provider about this. Some clues that the patient may already have the diagnosis are that they are on an anticoagulant, like one mentioned above, and they might be on AV nodal blockers like digoxin, beta blockers or calcium channel blockers. These medications help control the tachycardia, which is typically the most bothersome aspect of atrial fibrillation for patients.
If you are transporting your patient to the hospital, inform the triage nurse and leave a strip, with the patient identifiers, on the chart. If you are discharging them from the scene, leave a strip with the patient and inform them to take it to their primary health care provider or a walk-in clinic.
There are no recommendations for emergent initiation of anticoagulation, because the risk of a stroke on any given day of atrial fibrillation is relatively low. But, it is important that the diagnosis is not discounted and forgotten about. This represents an important opportunity for prevention that paramedics can offer, especially since many of the patients you encounter do not see health care providers regularly. In the meantime, you can advise the patient that this is a condition many people get as they age, it causes an irregular heartbeat, and it needs to be discussed with their health care provider at the soonest opportunity they get.
Not everyone with atrial fibrillation will benefit from anticoagulation, including young patients with no stroke risk factors or those who are deemed to have unacceptable bleeding risk with blood thinners, but this is unusual, and anticoagulation must be considered by the patient and their primary care provider once the diagnosis of atrial fibrillation is made. We will often start patients on anticoagulation in the emergency department when we make the diagnosis for the first time, not because of imminent stroke risk, but because this helps ensure the condition is identified and anticoagulation is begun and continued to prevent stroke in the future.
What About Cardioversion?
Traditional ACLS teaching is that when a patient has a non-sinus tachyarrhythmia and is hypotensive, electrical cardioversion is the treatment of choice. This strict adherence to ACLS teaching for rapid atrial fibrillation can be problematic for a couple of reasons.
First, cardioversion of atrial fibrillation in patients who are not anti-coagulated or have not been compliant with prescribed anticoagulation has been associated with ischemic stroke (6). The risk of this adverse event increases the longer the patient is in atrial fibrillation and the greater their risk factors for stroke 97). It is believed that if a clot has formed in the atria because of the disorganized activity of fibrillation, restoring sinus rhythm affords the clot a better opportunity to embolize into the systemic circulation. We often provide a period of anticoagulation and/or investigate for atrial thrombus before attempting cardioversion, especially if the patient has been in atrial fibrillation for more than 12-48 hours, of it is not known.
Second, most cases of rapid atrial fibrillation are not immediately life threatening when it is the primary problem. Patients may be uncomfortable and have soft blood pressures, but emergent cardioversion is typically not required, especially considering the stroke risk discussed above. Furthermore, rapid atrial fibrillation is often secondary to a different problem (sepsis, bleeding, pulmonary embolism, etc.) and the tachycardia is an appropriate compensation for this secondary insult. Lifesaving treatment in these cases focuses on treating the secondary problem and not on restoring sinus rhythm.
Conclusion
Remember to check-out the full Afib/Aflutter Best Practice Guideline review by clicking HERE.
References
- Lippi G, Sanchis-Gomar F, Cervellin, G: Global Epidemiology of Atrial Fibrillation: An Increasing Epidemic and Public Health Challenge. International Journal of Stroke. 2021;16;217-221.
- Atrial Fibrillation. Available at: https://www.heartandstroke.ca/heart- disease/conditions/atrial-fibrillation. Accessed December 16, 2022.
- Mukherjee K, Kamal, K: Impact of Atrial Fibrillation on Inpatient Cost for Ischemic Stroke in the USA. International Journal of Stroke. 2019;14;159-166.
- Alshehri, A: Stroke in Atrial Fibrillation: Review of Risk Stratification and Preventive Therapy. J Family Community Med. 2019;26;92-97.
- Laupacis A, Boysen G, Connolly S, et al. Risk factors for stroke and efficacy of antithrombotic therapy in atrial fibrillation: analysis of pooled data from five randomized controlled trials. Arch Intern Med. 1994;154;1449-1457
- Forslund T, Braunschweig F, Holzmann M, et al. Early Risk of Stroke in Patients Undergoing Acute Versus Elective Cardioversion for Atrial Fibrillation. Journal of the American Hearth Association. 2021;10.
- Airaksinen K, Gronberg T, Nuotio I, et al. Thromboembolic Complications After Cardioversion of Acute Atrial Fibrillation: The FinCV Study. Journal of the American College of Cardiology. 2013;62;1187-1192.
Trackbacks/Pingbacks