

Preamble: This Grand Rounds was inspired in part by a conversation I had with Dr. Andrew Petrosoniak during my time at St. Michael’s Hospital where we discussed the growing concern of excessive ED wait times and the limited concerted effort on addressing the waiting experience itself. In this blogpost, we will explore the concept of waiting, delve into the psychology and science behind the waiting experience, and explore potential design, technological, and workflow solutions that we can implement.
To prepare for this Grand Rounds, I spent several hours waiting in the main waiting rooms of both EDs at The Ottawa Hospital. This eye-opening experience allowed me to gain a deeper understanding of the end-user experience by observing many patients and their family members. I aim to present this blogpost partly from the perspective of a patient and provide insights into the waiting journey. The making of this Grand Rounds was also informed by the valuable input of many individuals, including the exceptional triage nurses, ED clerks, physician administrators, and the TOH Patient Relations Department. In order to share their candid perspectives with the reader, any anecdotes or quotes mentioned in this blogpost will be anonymized.
Seeking healthcare involves waiting
A large majority of Canadians will find themselves visiting an ED at some point in their lives, and it is an inevitable fact that they will experience a certain amount of waiting time. In Canada, seeking healthcare, particularly in the ED, has become synonymous with waiting. This reality has become increasingly evident, especially in light of a recent Ontario Health report, which indicates that the past year has been the worst on record since 2008.
- In September 2022, approximately 90% of patients waited up to 12 hours in the ED.
- Once admitted, 90% of these patients experienced wait times of up to 45 hours to complete their visit – a staggering increase of 40.5% compared to the previous year.
The increasing wait times represent just one facet of the larger, complex challenges within the healthcare system. These challenges, often referred to as wicked problems, seem insurmountable due to the diverse opinions and stakeholders involved, fiscal constraints, and interconnected nature of the issues. The solution, or at least a partial solution, lies in the realm of politics, extending beyond the confines of our healthcare facilities.
Regardless of how we tackle this problem, it is important to recognize that waits are an inherent part of our healthcare system. With this in mind, our focus should turn to strategies that enhance the waiting experience. The following topics are aimed at providing the reader with a better understanding of the waiting experience and tools to better empathize with those who experience waits within our healthcare system.
Waiting is an emotional experience
The psychology and science of waiting in various fields show that how you feel during the wait is equally, if not more, important than how long you wait. What truly matters is how the patient feels during that wait. A poor waiting experience is bad for all parties involved, creating a destructive cycle of frustration, and at times, even anger. As humans, our capacity for tolerating complaints about waiting may diminish over time. We get frustrated by individuals expressing their discontent about wait times, and consequently, people become increasingly frustrated and distressed by the mistreatment they perceive. Moreover, as indicated by the CAEP Position Statement in 2021, instances of violence in our departments, particularly towards healthcare providers, are on the rise. This highlights the urgent need to address the waiting experience beyond mere systemic changes. While considerable knowledge exists regarding the psychology of waiting in other domains, we have made minimal efforts to harness this understanding and improve the waiting experience in our own departments.
Perception of wait time matters
In the world of business, there is a fundamental principle of customer service that emphasizes the relationship between customer satisfaction and the concepts of perception and expectations. This seemingly simple yet complex equation stands as a guiding principle for many large businesses. In the context of the ED, we can adopt this framework to understand the psychology of patient satisfaction. Patients are satisfied when their perceived level of service or care exceeds their initial expectations. The larger the difference between their perception and expectation, the higher their level of satisfaction:
Patient satisfaction = Perception – Expectations
Consider the case of IKEA as an example. In the 1950s, IKEA emerged as one of the pioneers in crafting a store environment that provided customers with an immersive experience. Their showrooms allowed customers to touch and feel products out, encouraging them to physically interact by testing chairs or mattresses. These rooms played an essential role in demonstrating how IKEA pieces could seamlessly integrate into customer’s lives. While we certainly don’t want to replicate the level of comfort experienced in an IKEA showroom within the ED, this example underscores a crucial principle: perception matters. As ED physicians, we should explore ways to enhance patient’s perception of their waiting experience.
Perception refers to the internal feeling that we experience in response to the sensory information available to us, as well as our cognitive processing of that information. Or in other words, it encompasses what patients see, hear, and feel in their surroundings and how these experiences shape their internal impressions. In the hospital setting, noises are extremely common, whether it’s the PA system announcements, staff calling out names at regular intervals or the sound of frustrated patients. What patients witness plays a substantial role in shaping their perception of care they receive:
“What they’re witnessing plays a big factor. While waiting they witness traumatic events with security or other people escalating. It can cause a scene. Or sometimes they cause a scene. Staff have limited resources as it is and it becomes a “show”, with almost instant escalation.”
In fact, the mere presence of security coming and going from the waiting room can have a negative impact on your waiting experience. A recent study published in CJEM revealed that security personnel are not only responsible for managing agitation, by they are called upon to perform various other tasks, and increasingly during the discharge of patients.
Patients overhear much more than we realize. Although the conversations may not be about them specifically, it can still make them feel uneasy:
“Patients are seeing staff talking to others. They’re sitting there and feel vulnerable. Conversations are easily turned around for an insecure person or misinterpreted as if “they’re laughing at me”.
Patients also tend to estimate their own wait time variably. In fact, only 25-30% patients accurately estimate their wait time, partly because their perception of the wait is heavily influenced by their surroundings and personal experiences. A survey-based study conducted at a Swiss University hospital, involving over 500 patients, examined the factors that influence patients’ perception of wait time. They found that wait times are perceived differently by patients, especially when the wait becomes longer. In other words, two individuals who experience the same wait time will interpret the experience differently, resulting in two distinct perceptions of their wait.
Improve perception and manage expectations
Ultimately, we can positively impact patient satisfaction by enhancing the perception of their experiences and managing/adjusting their expectations. At the core of this lies effective communication. A systematic review conducted in 2017 looked to identify factors that influence ED patient experience. While wait times were found to be significant, other themes such as communication, empathy, compassion, and medical competence also played important roles. Not surprisingly, this finding underscores the inherent value patients place on appropriate and adequate communication. Our triage nurses and patient relations department, who review complaints, believe that communication is the most important element in influencing the perception of wait times. This includes clearly communicating the steps involved and discussing the expected duration for results and imaging, with the caveat that these times may be subject to change depending on the business of the department.
“Improving communication through each process, going through the steps. Being transparent that [the wait] could be longer.”
“Being transparent about the wait process, including waiting for lab results, imaging, etc.”
“A major area of improvement is communication around waiting to see consultants. Patients feel they are often in limbo once they have been consulted. Clear communication around time to consultant services can help improve this.”
The feeling of being forgotten is also identified as a strong reason for patient dissatisfaction and perception of their wait experience. In fact, this sentiment frequently emerges in the literature exploring perceptions of wait times. Lack of proper information about delays and the steps involved in their ED visit is often a contributing factor:
“It’s when they get into the next stage after seeing the doctor… and that’s comprised of being ignored and nobody updating them.”
“Common complaints surrounding waits involve the feeling of being ignored, forgotten, no one check in on them”
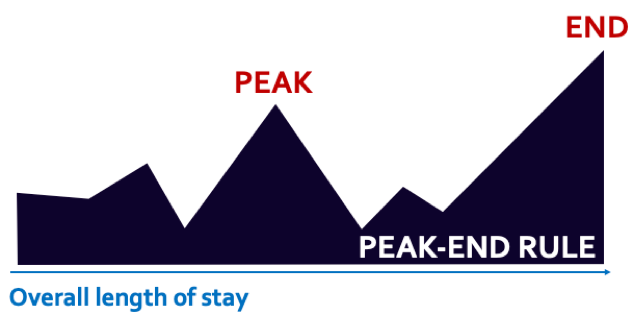
How can we help mitigate this sense of abandonment? One way is to leverage the time we spend with patients and take a few extra minutes to explain the wait process and rationale behind our management plan. This is important because of something called the peak-end rule. Dr. Daniel Kahneman, a psychologist and economist, argues that our memories of an experience are heavily influenced by how it ends and the memorable moments within it. The peak-end rule is a form of cognitive bias that explains why an event is not necessarily remembered by the entirety of its experience, but rather by snapshots that trigger emotional responses. The cumulative value of these snapshots, the peaks and valleys, dominates an individual’s overall experience. Notably, the end of the experience holds significant weight. Here, we can shape how patients perceive their waits to be by ending on a high note.
Communication is one important piece of the puzzle, but we all acknowledge that despite our best efforts, some patients will have negative experiences while waiting. For some, it may be their worst day, and the pain, anxiety and uncertainty they experience only amplify their discomfort. So how can we make the ED visit less uncomfortable? One approach is to examine the physical space and environment. Evidence-based design principles can help address this. They provide an objective dimension to subjective ideas, considering the environmental influences on patients’ well-being, including lighting, space and noise. Many studies have explored the use of biophilic design concepts, which incorporate elements of nature, and natural light to support circadian rhythms, improve sleep quality, reduced delirium and enhance overall patient satisfaction. Similarly, geriatric interventions like providing hearing aids or sleeping masks can improve sleep hygiene and minimize delirium. It’s also important to consider the neurodiversity within our population. Patients who are at a higher risk for agitation or escalation, or those with heightened anxiety, can benefit from having a separate quiet space as they wait for providers or tests.

Psychological principles of waiting
Principle 1: Unoccupied time feels longer than occupied time
In queuing psychology, the example of Disney is frequently described in how they effectively utilize the waiting experiences of riders and families. During peak seasons, the wait times for popular rides can extend to several hours. Disney mitigates this by incorporating the same level of production design found on the ride into the actual queue. Waiting in line is subsequently transformed into an engaging experience with its own entertainment value.
Patients who waited for hours in the ED found different ways to occupy themselves. Some were seen using their phone, while others engaged in conversations with family members or immersed themselves in reading books. However, many patients simply sit and wait, seemingly lacking any distractions from their acute medical concerns. While phones served as a ubiquitous source of entertainment, the patients’ occupied time would drastically reduce when their phone batteries ran out while waiting in the ED. This issue was commonly brought up by patients when they approached our triage RNs and clerks:
“I like the idea of having a phone charging area as there are a good amount of people who do not remember to bring their chargers when coming to the ED. ”
“More chairs, plug in’s/charging stations for phones and electronics, water refill stations, TV’s with shows or music etc.”
We can empower our ED groups to identify patient-centred strategies to address the issue of “unoccupied” time. Implementing cell phone charging stations and providing entertainment options like magazines, loaner iPads, and TVs can effectively reduce patients’ idle time. In the era of emerging technologies, we can also leverage patient-facing digital platforms to actively engage patients in their own care. One approach is to allow patients to input their medical history through technological solutions. By involving patients in their own care through pre-visit questionnaires, we can streamline certain aspects of documentation and gather valuable clinical data for patient assessments, research, or AI technologies. The ongoing pandemic has served as a catalyst for these advancements, proving the value of providing ownership, education and self-management support to patients through mobile apps.
The principle of moving patients forward, rather than returning them to the main waiting room they came from, helps them stay occupied. Evidence-based design solutions such as split flow EDs provide a separate area for patients awaiting results. Having patients physically move through different spaces gives patients a sense of progress and prevents them from feeling demoralized during their wait. In behavioural economics, we refer to this phenomenon as the dual response: consumers gradually become demoralized as they wait, but each forward movement in the queue elicits a positive response. The overall perception of the waiting experience depends on how these two responses balance out. Therefore, reinforcing the sense of progress through the physical environment, such as a dedicated area for receiving results, can significantly enhance patients’ perception of their wait.
Principle 2: Pre-process time feels longer than in-process time
Imagine yourself at a restaurant, eagerly waiting for the waiter to take your order for nearly half an hour. No one has come by to check on you. Instead, if the waiter promptly brings you the menu, takes your drink order, and serves your drinks within the first ten minutes, the overall experience feels less drawn-out. Even if the total time spent at the restaurant remains the same, the initial waiting period for the waiter to take your order feels more frustrating than waiting for your food to be prepared. We encounter this customer service tactic on a daily basis. In other words, pre-process time feels longer than in-process time. Patients perceive the wait more positively when they feel the service has begun.
We should strive to find ways to improve the upfront wait as it will enhance the overall wait experience. A local example of this is the Green Dot process, in which a specific subset of patients is identified by the nursing staff based on various triage criteria. This subset includes patients with chemical injuries, severe headaches, and priority CTAS 2 patients. Early identification of these patients not only improves their outcomes but also makes their experience less uncomfortable as they are “processed” sooner.
Another example involves medical directives that directly impact the patient experience by initiating care, making patients feel that their treatment has begun. Pain, in particular, is a common presenting complaint in the ED, and it serves as a valuable reminder for physicians to respond to those requests as soon as possible.
“I honestly think the medical directives help a lot! We can get a lot completed prior. I also think it is helpful when we can approach the doctor about certain cases and they pre-place an imaging order or med order (Ex: ketorolac for renal colic).”
“At triage I would say that some of the biggest patient care concerns are that they are not being treated promptly for conditions that can be quite painful. I would love to see more medical directives that are specific to certain ED presentations (ie. renal colic and toradol, migraine and toradol/ maxeran), recognizing that the initiation of medical directives can take a LOONNGG time.”
Another way to reduce the pre-process wait is to have a provider-in-triage (PIT) who can initiate care. A wealth of literature discusses the role of PIT doctors, and there have been success stories and failures. A systematic review and meta-analysis conducted in 2016, which included 25 studies, demonstrated that senior doctor triage can be an effective initiative to enhance ED performance. The meta-analysis focused on two RCTs conducted in Canada at Sunnybrook and University of Alberta Hospital. These studies showed a significant reduction in length of stay (LOS) for medium acuity patients, and reduced left without being seen (LWBS) metrics. In theory, any action that shortens the decision-making process and reduces delays can improve the overall patient experience. However, the success of implementing a PIT model is institution dependent. While there are limitations to the studies mentioned above, they highlight that when implemented appropriately, a PIT provider can have a meaningful impact on wait time metrics. Lessons learned from local implementation at TOH in previous years indicated that the effectiveness of a PIT provider relies on having the right individuals (with seniority and experience), proper training, and appropriate implementation strategies.
Principle 3: Uncertain waits are longer than known, finite waits
Imagine going about your daily routine when suddenly, something unexpected happens, throwing you off balance. For instance, you find yourself stuck in traffic, unsure of what the holdup is or how long you’ll be waiting. As humans, we seek and find comfort in predictability. Our patients often don’t experience that same sense of comfort. When their world is disrupted, it often leads to emotional chaos that can easily escalate into a crisis. Psychologists refer to this state of uncertainty as cognitive dread. As ED physicians, we do a really good job of empathizing with patients who are experiencing a crisis, knowing that this may be one of the worst days of their lives.
The psychology of waiting tells us that uncertainty is associated with anxiety and can make wait times feel longer than they actually are. One way to mitigate this is through effective communication of wait times. In 2015, Dr. Calder-Sprackman conducted a study involving patient focus groups and surveys. The patients strongly supported having access to ED wait time information before arrival (81% of patients) and while in the waiting room (90% of patients). At the time, over 3/4 of patients expressed that their overall satisfaction would improve if ED wait times were posted. This makes sense – having more certainty about wait times makes the waiting experience more manageable.
A recent scoping review of ED wait time displays in Canada showed that only 60 out of 647 Canadian EDs provide public-facing real-time wait time displays. Although 95% of these EDs provide an average wait time, averages often fail to provide meaningful certainty. For example, a patient who arrives at the ED late in the evening may have to wait for many hours into the night if there is single-doctor coverage (as is the case in many EDs). The communicated average wait time may differ significantly for patients depending on local ED volume patterns.
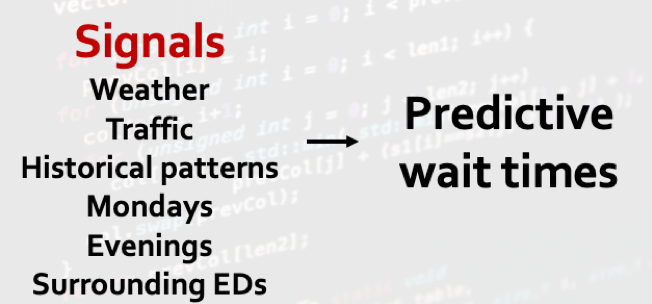
However, it turns out that human behaviour is more predictable and certain than we think. Let’s take a look at this six-month data on daily ED visits at TOH General Campus. At first glance, there may not seem to be an obvious pattern. However, the daily visits hover within a certain range, and there are discernible peaks and valleys that appear to follow a cyclical pattern. This pattern is considered a stationary time series because the mean and variance don’t change drastically over time, and it can be approximated by a straight horizontal line. This is important because when the data isn’t overly “chaotic” and appears stationary, we can start identifying signals amidst the noise. For instance, we know anecdotally that Mondays tend to be busier than other days, and evenings tend to be busier than daytime hours. We also know that Boxing Day is one of the busiest days in the ED, and a significant snowstorm can lead to decreased volumes. With this human predictability and signals in the data, we can forecast what wait times might be like.
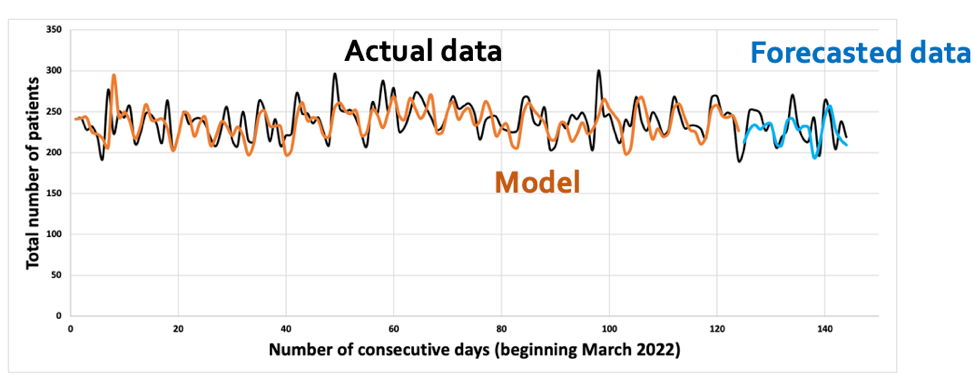
Computers and artificial intelligence (AI) algorithms can take this even further by leveraging recency of data. Based on patterns observed over the past few weeks, days, or even hours, we can predict wait times with a reasonable level of certainty. We can incorporate signals such as weather conditions, traffic, and historical volumes on similar days in previous weeks or months.
Despite advancements in computers and sophisticated algorithms, at minimum, we can improve communication with patients to enhance certainty for those waiting to be seen. When asked about the most common reason patients approach the triage nurses or the clerks, it is frequently to inquire about wait times:
“I would say the most common reason that someone approaches the triage window while waiting would be to see if they have been missed on the list or to see how many people are ahead of them/ how much longer they have to wait.”
“Asking about wait times, where they are in the line up, why they aren’t being called”
“Frequently interrupted about wait times”
So how do we design a better system? Part of the solution involves asking the end-users themselves. A group in Australia obtained qualitative feedback from actual patients waiting in the EDs on various visualization elements and display styles. They conducted multiple rounds of participant testing to rapidly iterate, evaluate, and refine their design features. They initially tested individual design elements and the best ways to present wait times relative to the current time, as well as how to convey ranges of estimates. They compared options that varied in the degree to which text was replaced with visuals. In their study, they found that people felt more reassured about their own waiting time and were able to put their situation into perspective when they knew the urgency of others. They subsequently combined all the design elements into a three-column display, tested different variations, and arrived at an ideal version based on patient feedback. This is a great example of displaying anticipated wait times, coupled with wait time ranges, and emphasizing that there will be perceived inequities and that it won’t solely be a first-come, first-served system.
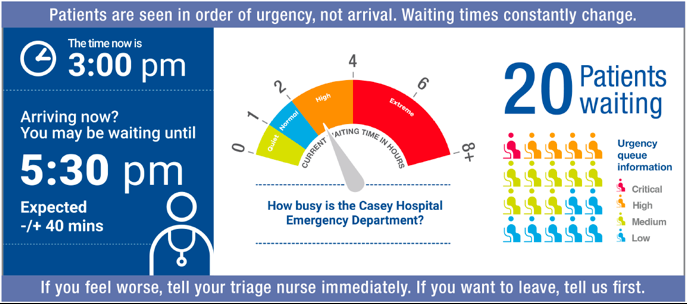
We know there’s uncertainty with wait times. In such a stressful environment where people are emotionally and physically challenged, simplicity is crucial, and the visual language must cater to a diverse audience. When wait times are effectively conveyed in this manner, patient experience improves, as demonstrated by this group’s findings.
Principle 4: Unfair waits feel longer than equitable waits
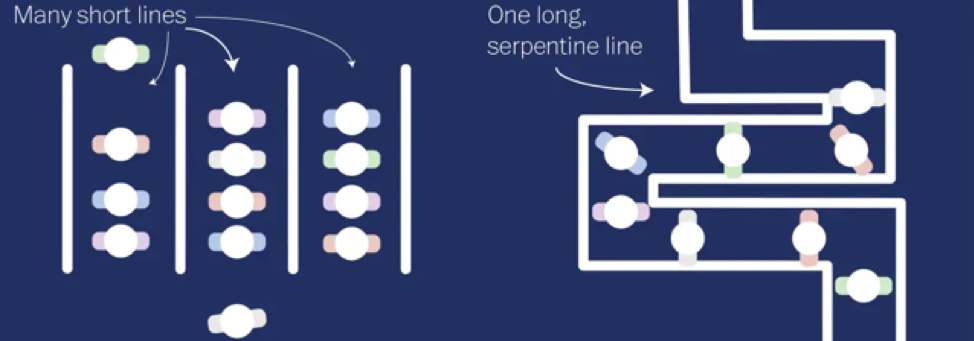
Over the years, we have witnessed the evolution of retail checkouts, such as the example of Walmart who introduced a checkout experience across North America that aims to challenge traditional methods. The design is simple: all individual lanes have been eliminated, and instead, there is a single line leading to 20-30 registers, depending on the store’s size. This setup allows customers to have some control, as they can choose between self-checkout or seeking assistance from hosts who have replaced cashiers. Most importantly, it eliminates the concept of parallel lines and its associated experience.

In queuing psychology, parallel lines, such as those found in grocery store checkouts, can be anxiety provoking. The stress of choosing the shortest line combined with the possibility of unforeseen circumstances causing delays creates uncertainty. No matter how much you analyze the contents of people’s carts, the person in front of you may still pull out a stack of coupons or a bag filled with coins. These situations, known as slips and skips, occur when individuals who joined the line later overtake those who arrived earlier. This generates considerable anxiety and uncertainty.
This system may be challenging to implement in the ED because we prioritize the sickest patients. However, by eliminating the perception of parallel lines, the process appears fairer since no one likes to witness others jumping the queue. Our triage nurses often encounter variations of this complaint.
“They get irritated if they see others jumping ahead or being given priority for no apparent good reason”
”Patients will often come up and say they have been waiting for hours and ask why multiple individuals have gone in after them.”
Psychologists argue that people strive for social fairness, and it feels socially fairer when customers who arrive first are served first. Customers waiting in line often value fairness more than efficiency, and studies have demonstrated that serpentine lines make customers happier than parallel lines, regardless of the wait time. This sense of guaranteed fairness significantly reduces stress and anxiety.
How can we achieve this in the ED? One approach is to implement physical separations within the department, creating distinct waiting areas for patients with different acuity levels or separate rooms for those awaiting test results. This physical separation promotes social fairness, and literature supports the notion that it not only improves efficiency but also enhances patient satisfaction. We can also improve our design to effectively communicate our triage process to patients, ensuring they are not caught off guard when others appear to be moving ahead in line.
Summary
Waiting is an emotional experience and the length of time a patient waits doesn’t matter as much as we think it does. Rather, how the patient feels during their wait process should hold equal importance. While considerable knowledge exists regarding the psychology and science of waiting in other domains, we have made minimal efforts to harness this understanding and improve the waiting experience in our own departments.
Patients are satisfied when their perceived level of care exceeds their expectations. And this perception is impacted by what’s happening around them, how we interact and communicate with them. We can impact how patients perceive their waits through:
- Effective communication
- Peak-end rule: end on a high note as the memorable moments (ie. during physician-patient encounter) heavily impacts overall patient experience
- Evidence-based design solutions: biophilic designs, natural lighting, minimize noise
- Geriatric interventions
- Consideration of neurodiversity within our population
Unoccupied time feels longer than occupied time. We should identify patient-centered strategies and actively engage patients in their own care. Some strategies include:
- Cell phone charging stations
- Positive distractions: entertainment, TV, magazines
- Patient-facing digital platforms: pre-visit questionnaires, technological solutions
- Leverage dual response: reinforcing a sense of progress by having patients move through the physical space, such as a dedicated area for receiving results.
Pre-process time feels longer than in-process time. The upfront wait often feels worse and we should aim to front-load our assessments and workup. Working with our nursing colleagues and physician administrators, we can improve on various system-level changes including:
- Medical directives
- Provider-in-triage
- Fast track zones
Uncertain waits are longer than known, finite waits. Uncertainty around wait times can further exacerbate patient anxieties in an already stressful situation. We can both communicate and predict wait times effectively. Some strategies include:
- Asking patient end-users themselves what they prefer
- Predictive wait times using forecasting methods and AI algorithms
- Clear communicated displays that cater to a diverse audience
Unfair waits feel longer than equitable waits. People strive for social fairness, and often value fairness more than efficiency. Multiple parallel lines can promote anxiety and frustration. We can mitigate this by:
- Communicating the triage process more effectively (ie. sicker patients are seen first)
- Eliminate the perception of parallel lines by implementing physical separations within the ED
DeClerq, Katherine. “Ontario Er Wait Times for Hospitals Reach Record High in September.” Toronto, 9 Nov. 2022, toronto.ctvnews.ca/average-ontario-er-wait-times-for-admitted-patients-reach-new-yearly-high-in-september-1.6145262. Drummond, Alan, et al. “CAEP Position Statement on Violence in the Emergency Department.” Canadian Journal of Emergency Medicine, vol. 23, no. 6, 2021, pp. 758–761, https://doi.org/10.1007/s43678-021-00182-z. Gupta, Sahil, et al. “Trends in the Role of Security Services in the Delivery of Emergency Department Care.” Canadian Journal of Emergency Medicine, vol. 25, no. 1, 2022, pp. 43–47, https://doi.org/10.1007/s43678-022-00406-w. Spechbach, Hervé, et al. “Patients’ Time Perception in the Waiting Room of an Ambulatory Emergency Unit: A Cross-Sectional Study.” BMC Emergency Medicine, vol. 19, no. 1, 2019, https://doi.org/10.1186/s12873-019-0254-1. Sonis, Jonathan D, et al. “Emergency Department Patient Experience.” Journal of Patient Experience, vol. 5, no. 2, 2017, pp. 101–106, https://doi.org/10.1177/2374373517731359. Zelmer, Jennifer. “Transforming Care and Outcomes with Digital Health Through and Beyond the Pandemic.” NEJM Catalyst, 31 May 2022. Abdulwahid, Maysam Ali, et al. “The Impact of Senior Doctor Assessment at Triage on Emergency Department Performance Measures: Systematic Review and Meta-Analysis of Comparative Studies.” Emergency Medicine Journal, vol. 33, no. 7, 2015, pp. 504–513, https://doi.org/10.1136/emermed-2014-204388. Calder-Sprackman, Samantha, et al. “Availability of Emergency Department Wait Times Information: A Patient-Centered Needs Assessment.” Emergency Medicine International, vol. 2021, 2021, pp. 1–6, https://doi.org/10.1155/2021/8883933. Walker, Katie, et al. Visualising Emergency Department Wait Times; Rapid Iterative Testing to Determine Patient Preferences for Displays, 2022, https://doi.org/10.1101/2022.03.30.22273211. Smith, Matt. “New Checkout Experience Seeks to Eliminate the Wait and Add Options at the Register.” Walmart Corporate Affairs, 30 June 2020, corporate.walmart.com/newsroom/2020/06/30/new-checkout-experience-seeks-to-eliminate-the-wait-and-add-options-at-the-register. Swanson, Ana. “What Really Drives You Crazy about Waiting in Line (It Actually Isn’t the Wait at All).” The Washington Post, 25 Nov. 2021, www.washingtonpost.com/news/wonk/wp/2015/11/27/what-you-hate-about-waiting-in-line-isnt-the-wait-at-all/. References
