
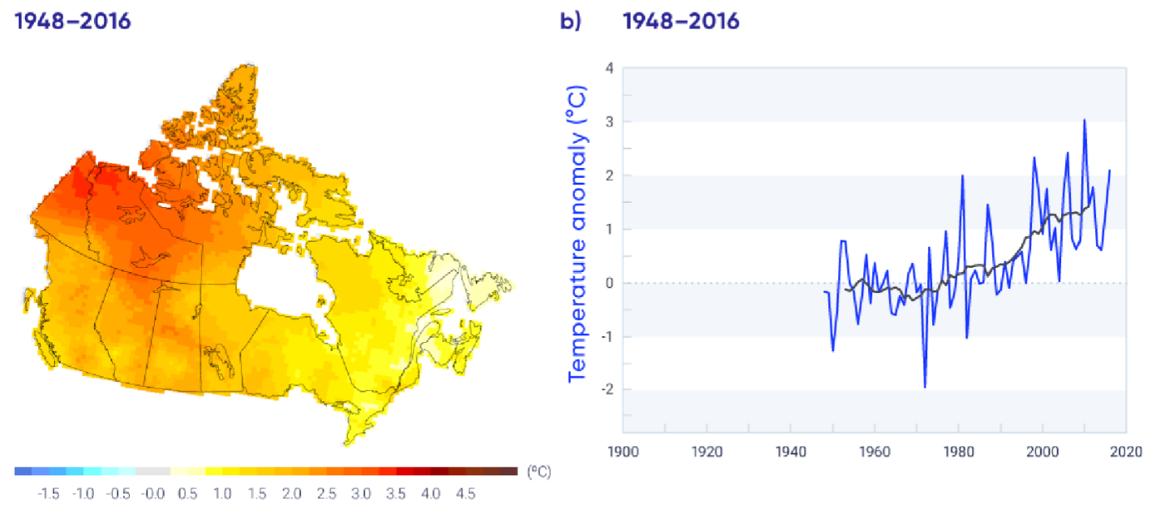
Global temperatures are increasing and are projected to continue warming. The rates of warming across out planet are not uniform. In Canada, the loss of snow and sea ice reduces the reflectivity of the surface leading to increased absorption of solar radiation and a faster rate of warming compared to more southern regions. As a result of this phenomenon, known as Arctic amplification [1], Canada’s rate of surface warming is more than double the global rate.
The effects of climate change on health are driven by evolving climate conditions manifested as surface temperature warming, extremes of precipitation, disastrous extreme events, and rising sea levels. These drivers modify key factors, such as the natural and built environments, and social determinants of health, that increase the vulnerability of individuals and populations at large. Consequently, people are exposed to more biological, psychosocial, chemical, and physical stressors such as, hotter temperatures, poor air quality, deficient nutrition, evolving infectious pathogens, and population displacement [2]. Ultimately these complex pathways lead to adverse health outcomes e.g., heat related illness, cardiopulmonary disease, transmissible infectious disease, and mental illness.
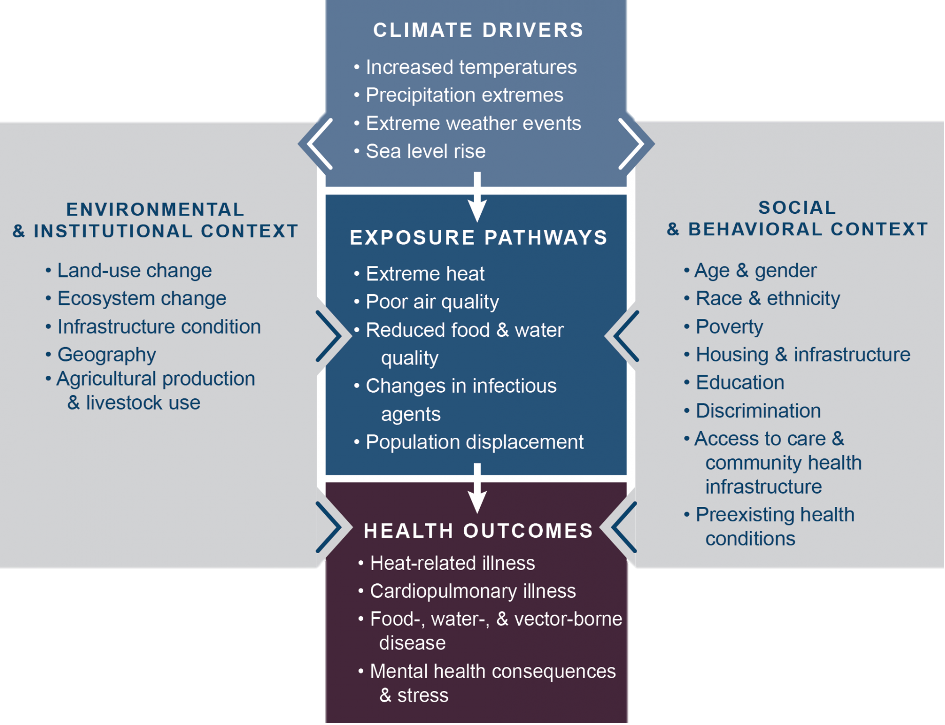
Adapted from [2]
How extreme heat affects the Emergency Department
Shengzhi et al. (2021) conducted a time-stratified case crossover analysis of a nationwide American nationwide healthcare claims database to quantify the association between ambient heat and ED visits [3]. They found that days of extreme heat were associated with a higher risk of ED visit for any cause, heat-related illness, renal disease, and mental disorders. Kegel et al. (2021) retrospectively analyzed the impact of temperature on ED volume and length of stay in two Canadian hospitals [4]. They found that higher 3-day mean temperatures were associated with higher daily ED volumes as well as longer median length of stay suggesting that a warming climate can impede emergency service provision by increasing the demand for and delaying timely care.
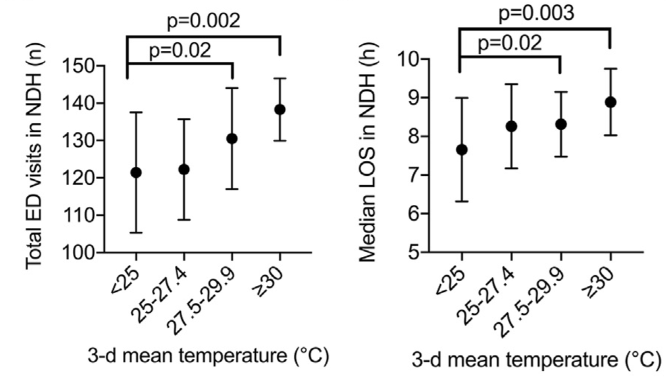
Figures adapted from [4]
The spectrum of heat related illness
Heat-related illnesses exist on a spectrum from relatively benign self-resolved problems to critical, life-threatening conditions. This section will review how to recognize and manage each of these diseases.
Heat Rash

Figure adapted from [6]
Also known as prickly heat or miliaria rubra, heat rash manifests classically as an intensely itchy vesicular rash on an erythematous base [5]. It usually appears on areas covered by clothes and is caused by sweat gland obstruction and inflammation. The rash usually develops within a few days of exposure to a warmer climate but can develop weeks later. It can generally be prevented by wearing light, loose fitting, clean, dry clothing and avoiding activities that cause excessive sweating [6]. The best treatment is to leave the hot environment and the rash will usually resolve within 2-3 days. If a patient is so symptomatic that they presented to the ED due to this rash, a short course of medium potency topical steroid can provide them some relief until the rash resolves.
Heat Cramps

Figure adapted from [7]
Heat cramps usually present as generalized, brief, intermittent large muscle group contractions usually occurring within the first few days of exertion in a hot environment. Athletes, construction workers, and agricultural workers are commonly affected. These cramps are typically caused by dehydration and salt depletion and are associated with hyponatremia and hypochloremia [5]. In contrast to exercise-associated muscle cramps that are typically focal, occurring during exercise, and relieved with passive stretching, heat cramps are diffuse, occur after exertion, and are relieved with oral salt solutions or electrolyte replacement. A litre or two of commercially available electrolytes solution should provide adequate replacement [8]. The associated electrolyte disturbances are mild and there is no association with rhabdomyolysis or renal damage.
Heat Edema
This problem typically presents as lower extremity swelling in older, non-acclimatized individuals after exposure to a warmer climate. It is caused by an interplay between cutaneous vasodilation in response to heat, increased hydrostatic pressure, and vascular leak leading to accumulation of interstitial fluid [8]. Differential diagnoses include congestive heart failure, DVT, cellulitis, or liver or kidney dysfunction, but a careful history and physical exam should help you make this diagnosis. The treatment is simply elevation and compression stockings. The edema should reverse with acclimatization to the warm environment. Diuretics are ineffective and should be avoided as they can worsen volume depletion.
Heat Syncope
With peripheral vasodilation you get orthostatic pooling of blood, which in combination with prolonged standing, and perhaps less-than-optimal cardiovascular fitness results in decreased central venous return, cardiac output, and cerebral perfusion causing loss of consciousness. It is important to consider and appropriately work-up alternative causes of syncope [5]. An ECG and basic bloodwork should be obtained at minimum. Heat syncope is a self-limited condition – patients recover completely with rest and oral rehydration [8]. On discharge, patients at risk should be instructed to move often, flex their larger leg muscles while standing, avoid prolonged standing, and to sit or lay down if they feel prodromal symptoms.
Heat Exhaustion
This moderate-severe heat-related illness is caused by volume depletion, either water or salt depletion, due to prolonged exposure to high ambient temperature with strenuous exertion. It can present as weakness, fatigue, thirst, headache, nausea, dizziness, and muscle aches. In severe cases, patients may be tachycardic with moderately elevated core temperatures. Importantly, their temperature should be less than 40 °C and there should be no major CNS dysfunction. Patients will often be hyponatremic, hypochloremic, have decreased urine sodium and chloride, and may have elevated CK, creatinine, and hepatic transaminase levels [5]. Treatment will depend on severity and degree of electrolyte derangement. More mild cases can be managed conservatively with rest and oral rehydration. However, in severe cases with more pronounced volume depletion and electrolyte derangement intravenous rehydration may be required. Start with a small bolus of normal saline then proceed with further volume replacement slowly based on their sodium levels to avoid rapid overcorrection.
Heat Stroke
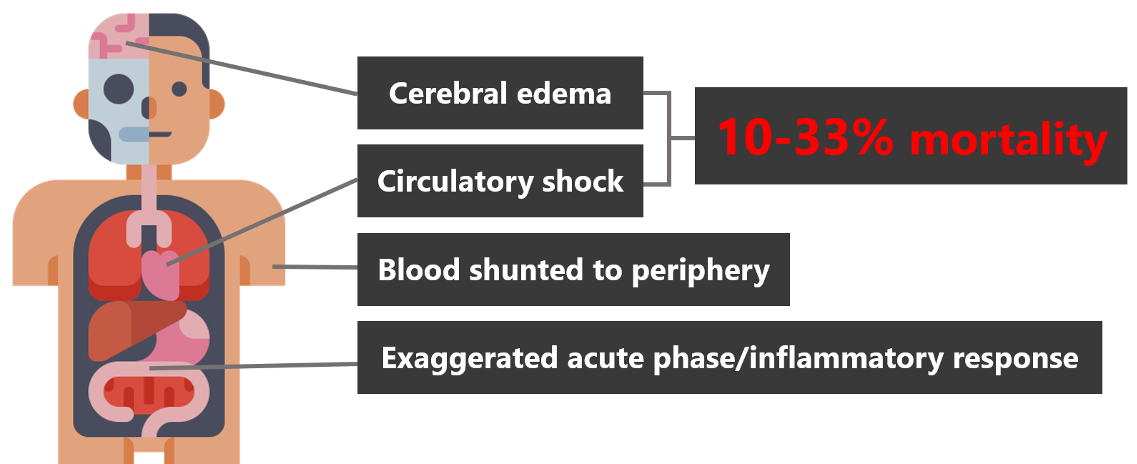
Heat stroke is a life-threatening emergency. It occurs when internal core temperatures rise above a critical level causing the body’s normal thermoregulatory mechanisms fail leading to core temperatures in excess of 40 °C and multisystem tissue and organ dysfunction. The hallmark of heatstroke and key to making the diagnosis is the presence of CNS dysfunction that’s to say altered mental status, seizure, or coma in addition to hyperthermia. The body responds to heat stress by shunting blood to the peripheral circulation to facilitate heat loss. This results in a 30% decrease in renal and splanchnic perfusion by [8]. It’s theorized that gastrointestinal tract hypoperfusion incites an exaggerated acute phase inflammatory response that progresses in a sequence like that seen in sepsis. Furthermore, at critical levels of hyperthermia, heat causes direct tissue injury, protein denaturation, and cell death via apoptosis and necrosis. This cascade of inflammation and tissue injury leads to circulatory shock with hypotension and cerebral edema with petechial hemorrhage resulting in a 10-33% mortality rate.
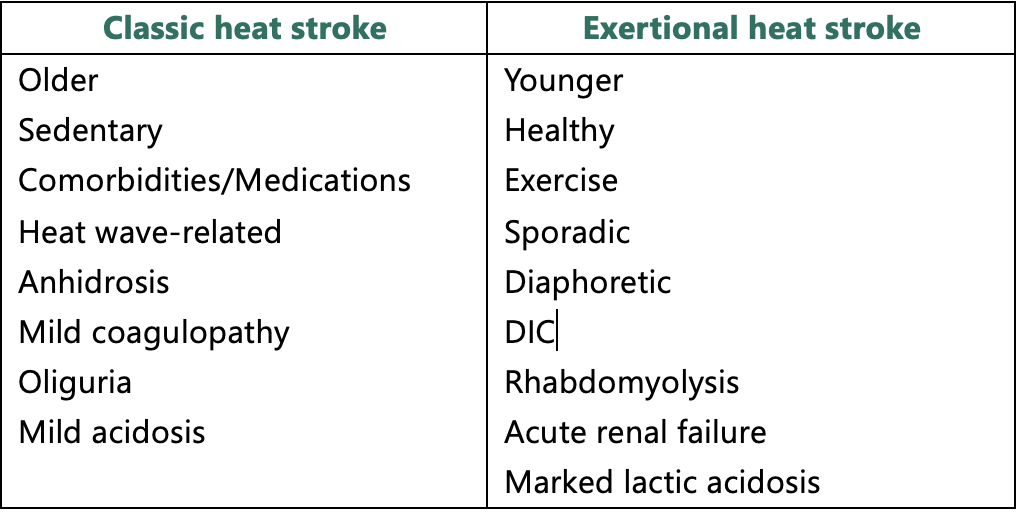
There are two categories of heat stroke: classic and exertional. Classic heatstroke results from passive exposure to high environmental temperatures. Exertional heat stroke results from pathologic hyperthermia during strenuous exercise. The table below contrasts the two types of heat stroke [5,8]:
Prescription medications and recreational drugs also play an important role in increasing risk for and precipitating heat-related illness. Broadly speaking, these drugs either increase endogenous heat production (e.g., sympathomimetics, α-adrenergic agonists, thyroid agonists) or compromise thermoregulatory mechanisms (e.g., β-blockers, CCBs, diuretics, alcohol, benzodiazepines) [8]. It is important to note that patients with these substances onboard will have ongoing heat production even after removal from the hot environment.
Heat stroke Management and Cooling Modalities
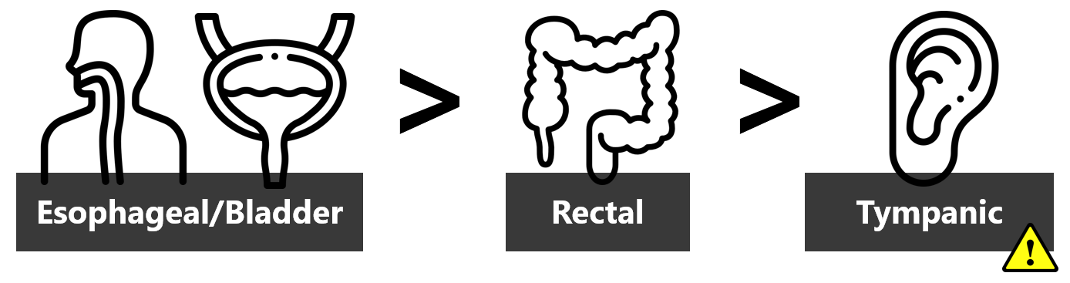
All patients who present altered with a temperature above 38 °C should have a core temperature measurement. This can be accomplished by tympanic, rectal, bladder, or esophageal measurement. Tympanic measurement may be the easiest, but it is the least accurate, does not allow continuous monitoring, and above certain temperatures some devices may display an error message or simply upward facing arrows instead of an actual temperature. A prospective ICU study compared these methods to pulmonary artery catheter-measured temperature and found that urinary bladder and esophageal measurement are the most reliable methods [9]. Within the ED, when managing these critically ill patients, who need continuous temperature monitoring, catheterization with a temperature-sensitive Foley should be a priority.
The gold standard for treating exertional heat stroke, in both the field and in-hospital settings, is cold water emersion. These patients can rapidly develop shock with multiple organ failure and rapid cooling reverses that process. This intervention should be initiated immediately and aggressively. Emersion cools at a rate to around 0.2 °C per minute and the target core temperature should be no less than 39 °C to avoid hypothermia [8]. If a specific emersion device, bathtub, or inflatable pool are not available, a disposable shroud may be used as a water container. A recent systematic review and meta-analysis compared emersion in cold water (at 14-17 °C), colder water (at 8-12 °C), and ice water (at 1-5 °C) and found no significant difference in rate of temperature reduction [10].

The TigerCat)® emersion device at The Ottawa Hospital consists of a plastic frame with a waterproof liner and attached spigot for easy drainage
This is the gold standard for exertional heat stroke and should be considered the first-line treatment. However, it does have significant limitations: it can be cumbersome to set up and can creates a water hazard that can threaten staff and equipment safety. Monitors will work when attached to a submerged patient; they can be finicky and prone to unsticking, however, patients need only be emersed for 10-20 minutes to achieve the target temperature. The tachyarrhythmias associated with heatstroke usually resolve with cooling, and cardioversion should be avoided until the myocardium is cooled [5].
Think of cold-water emersion as a high-acuity, low-opportunity procedure. It has specific indications for which it is the first-line, guideline-supported intervention and can be lifesaving but has significant pitfalls. Bearing in mind environmental limitations, cooling hyperthermic patients should not be delayed and emersion is the best way to do it. Often there may be an urge to intubate these patients as they will have severely decreased GCS and be very tachypneic. Intubation further delays cooling and will worsen hypotension threatening mortality. Once they’ve cooled to below 39 °C they should gradually wake up and their hemodynamics should improve.
The second-best cooling option, and perhaps the more practical option for intoxicated, very agitated patients, and older patients with classic heat stroke is a cooling blanket placed beneath the patient to control temperature via conductive and convective cooling. These systems are composed of a water tank with heater and cooler, compressor, and pump that circulates water through a blanket in contact with the patient’s skin. A bladder or esophageal probe is connected to the control unit and the device will adjust the temperature of the circulating water to achieve the programmed target temperature [11]. It cools about 0.05-0.1 °C per minute. For hyperthermic patients the device should be set to target a temperature of 38 °C.

The Blanketrol III® programmable hyper-hypothermia system used at The Ottawa Hospital
To improve the rate of cooling, these conductive and convective cooling methods should always be used in conjunction with evaporative cooling. Evaporative cooling consists of spritzing the patient with cool, not cold tap water and circulating air around them with fans. This is practically the easiest first-line cooling method but is the least efficacious. Used in combination with a cooling blanket, the rate of heat dissipation approaches that of emersion, but remains inferior.
While hyperthermic patients are being actively cooled, the next priority is volume resuscitation. Exertional heat stroke patients typically have a 4-6 L fluid deficit [8]. Optimizing hydration augments circulation and heat exchange. For heat stroke, start with 1-2 liters of normal saline. Patients blood pressures should improve with cooling. Further volume resuscitation should be guided by laboratory analyses. If the patient has severe, symptomatic hyponatremia, consider hypertonic saline. If rhabdomyolysis is present (and it probably will be), target urine output 2 mL/kg/hour. Continue monitoring for sings of pulmonary edema.
Adjunctive cooling methods include ice packs and cold IV fluids. These should not replace the cooling methods described above. Ice packs can be placed in the groin, axillae, and neck area. Care should be taken to check skin every 10-20 minutes and move them to prevent frostbite. If available cold IV fluids are beneficial, but resuscitation with room temperature fluid is adequate. Avoid bladder lavage as this somewhat cumbersome, would interfere with bladder temperature measurement, and is not very effective.
Antipyretics have no role in hyperthermia. Fever is a controlled process, whereas hyperthermia is thermoregulatory failure. Antipyretics will not help and if anything may be harmful. Anticholinergics and any other medications that increase endogenous heat production or compromise thermoregulatory mechanisms should be avoided. The only pharmacologic treatment recommended is a benzodiazepine of choice to help manage agitation and control shivering [8].
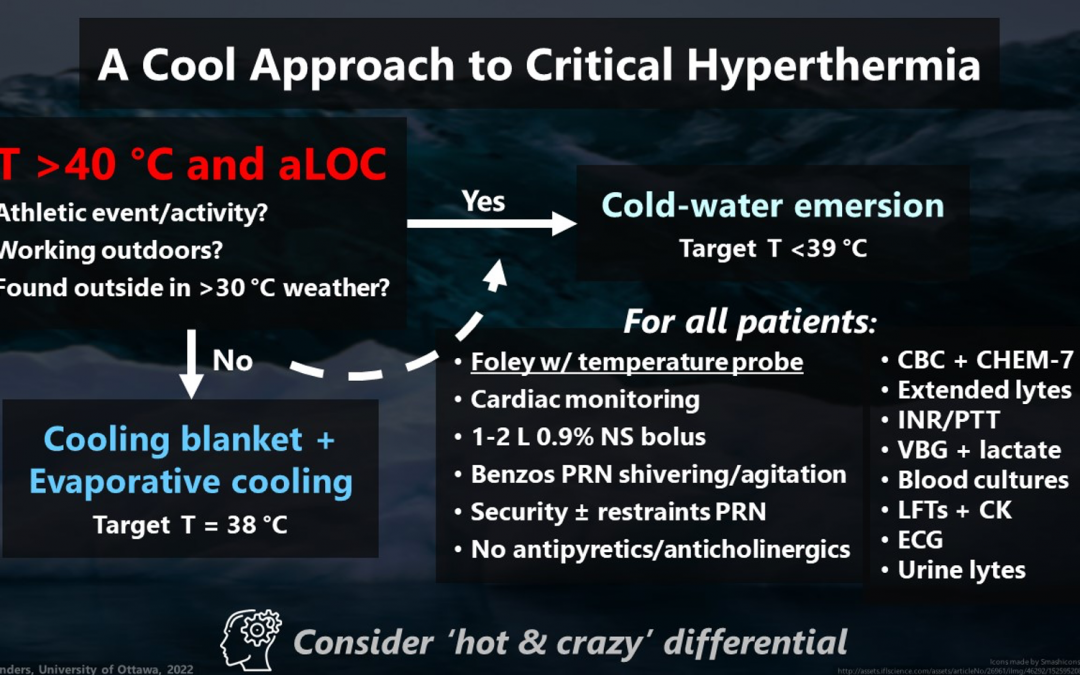
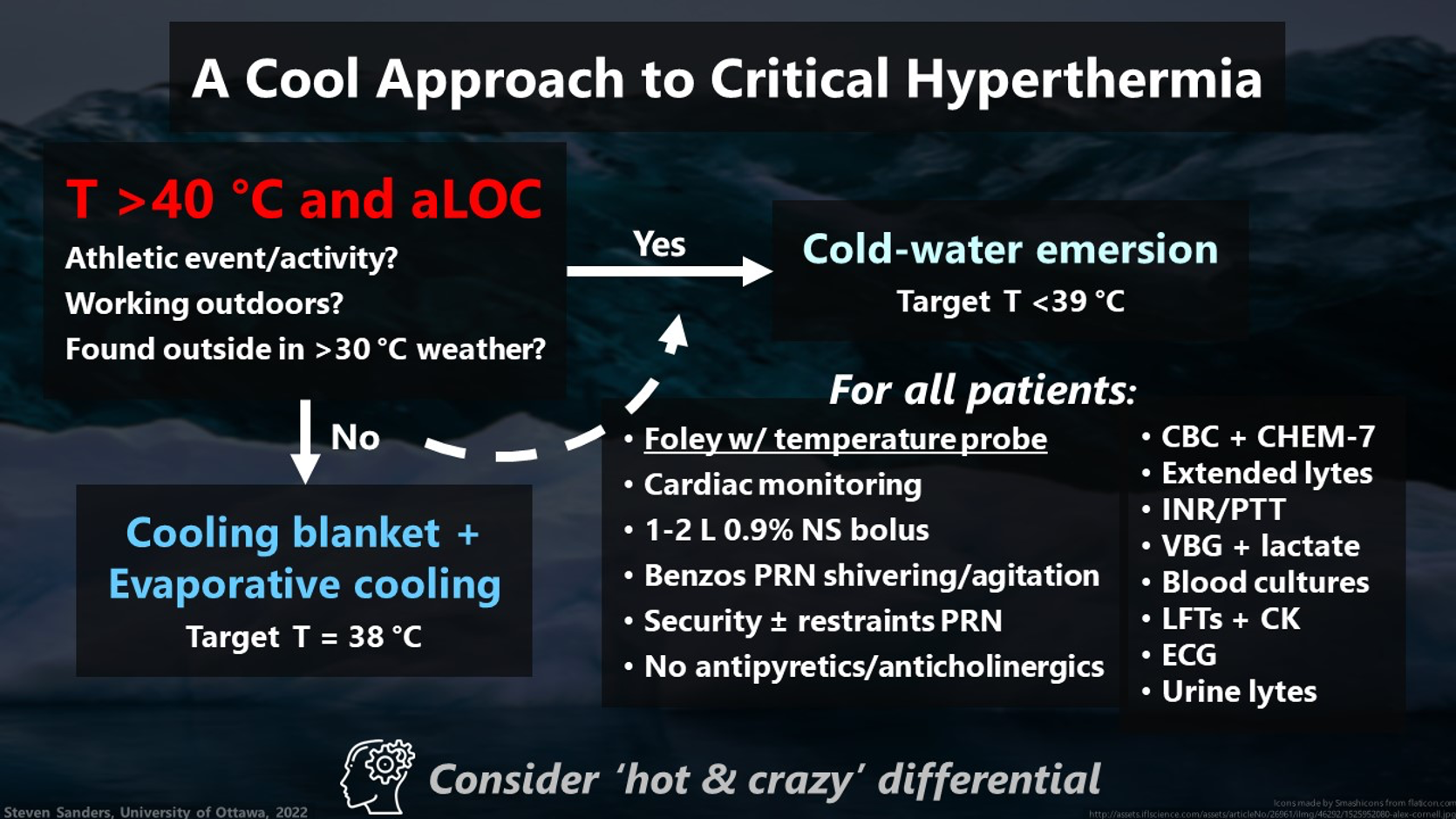
Proposed approach to the hyperthermic patient with altered mental status
A proposed initial approach to hyperthermia that places stronger emphasis on using cold-water emersion specifically for cases of exertional heat stroke is summarized below. If a patient presents hyperthermic i.e., core temperature >40 °C, measured ideally by bladder or rectal probe, and altered mental status strongly consider the diagnosis of heat stroke. If you have advanced notice from EMS or are told on handover that the patient was participating in an athletic event or activity, was working outdoors, or was found outside in over 30 °C weather, then there is a high probability for exertional heat stroke and cold-water emersion should be the first-line cooling modality targeting a core temperature no less than 39 °C.
If those features are absent, exertional heat stroke is less likely and classic heat stroke or a toxicologic cause are more likely. Again, consider cold-water emersion if you think the patient will tolerate it – it is most effective and it is fast. Otherwise, proceed with cooling via cooling blanket with a programmed target temperature of 38 degrees and evaporative cooling with cool water spray and fans.
All patients should have continuous core temperature monitoring with a bladder probe initiated as 1st priority, along with cooling. They should have cardiac monitoring, but this shouldn’t delay cooling. Rehydrate them and provide calming medications as needed. Having security at bedside will be helpful when they wake up, but struggling against restraints can generate more heat and worsen rhabdomyolysis. No antipyretics or anticholinergics. Initial investigations should include CBC with extended electrolytes, coagulation studies, VBG, lactate, LFTs, CK, an ECG, and urine electrolytes. Finally, it’s important to consider your complete ‘hot and crazy‘ differential and investigate and treat as indicated.
References
- https://changingclimate.ca/site/assets/uploads/sites/2/2020/06/CCCR_FULLREPORT-EN-FINAL.pdf
- https://health2016.globalchange.gov/climate-change-and-human-health
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9397126/
- https://www.wemjournal.org/article/S1080-6032(21)00086-7/pdf
- Rosen’s Emergency Medicine: Concepts and Clinical Practice, 10th Ed.
- https://dermnetnz.org/topics/miliaria
- https://www.mariespano.com/wp-content/uploads/2015/11/cramping.png
- Wilderness Medical Society Clinical Practice Guidelines for the Prevention and Treatment of Heat Illness: 2019 Update
- https://pubmed.ncbi.nlm.nih.gov/12577157/
- https://www.sciencedirect.com/science/article/abs/pii/S0300957220300289?fr=RR-2&ref=pdf_download&rr=75ed450138b9f015
- https://www.gentherm.com/en/medical/hyper-hypothermia/blanketrol-3
