
According to WHO and CDC: more than nine people die every minute from injuries or violence, and 5.8 million people die every year. It is the leading cause of death in people 1-44 years of age in developed countries (unintentional injuries, homicide, suicide).
The most common cardiac rhythm in Traumatic Cardiac Arrest (TCA) is pulseless electrical activity (PEA). Patients in medical cardiac arrest often have a detectable dysrhythmia. The problem is that TCA is often treated in a similar or identical fashion to medical cardiac arrest (compressions, epinephrine, fluids) despite the known differences in pathophysiology.
Cardiac Physiology
Cardiac output is the volume of blood pumped by the heart per minute. This is calculated by multiplying HR x SV (SV is dependant on preload, contractility and afterload). The pathophysiology of traumatic cardiac arrest is highly variable depending on the mechanism of injury and the structures that are injured.
When trauma patients lose effective cardiac output, it is due to critical hypovolemia and loss of preload, obstructive cariogenic shock (cardiac tamponade, tension hemothorax/pneumothorax), critical hypoxemia, or a neurogenic shock due to a catastrophic CNS injury.
Reversible Causes of Traumatic Cardiac Arrest
Hypovolemia
The loss of blood volume (leading to hypovolemic shock) is common in both penetrating and blunt trauma. This adversely affects tissue perfusion causing shock. It is why the prioritization of blood in these patients is so critical.
Hypoxemia
Resulting from any injury that adversely affects respiratory gas exchange. Very commonly this is a product of tension hemothorax/pneumothorax; where increased intrathoracic pressure decreases subsequent venous return to the heart.
Cardiac Tamponade
Blood rapidly accumulates in the pericardial sac, thereby limiting adequate ventricular filling and leading to obstructive shock.Remember, there may be a concurrent medical condition (which may have preceded the traumatic injury), which should be considered and addressed.
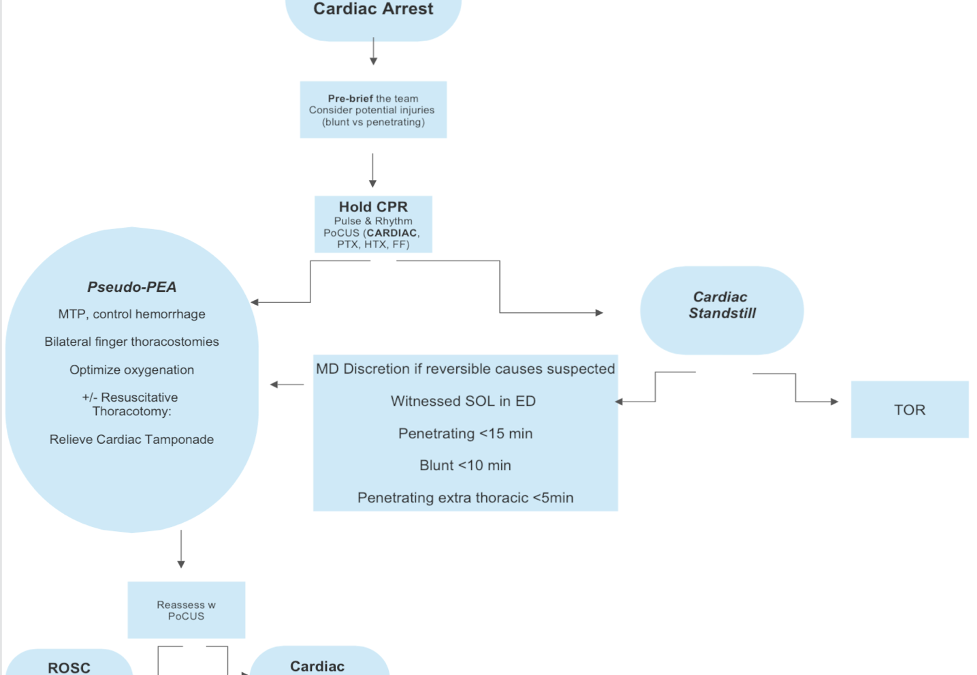
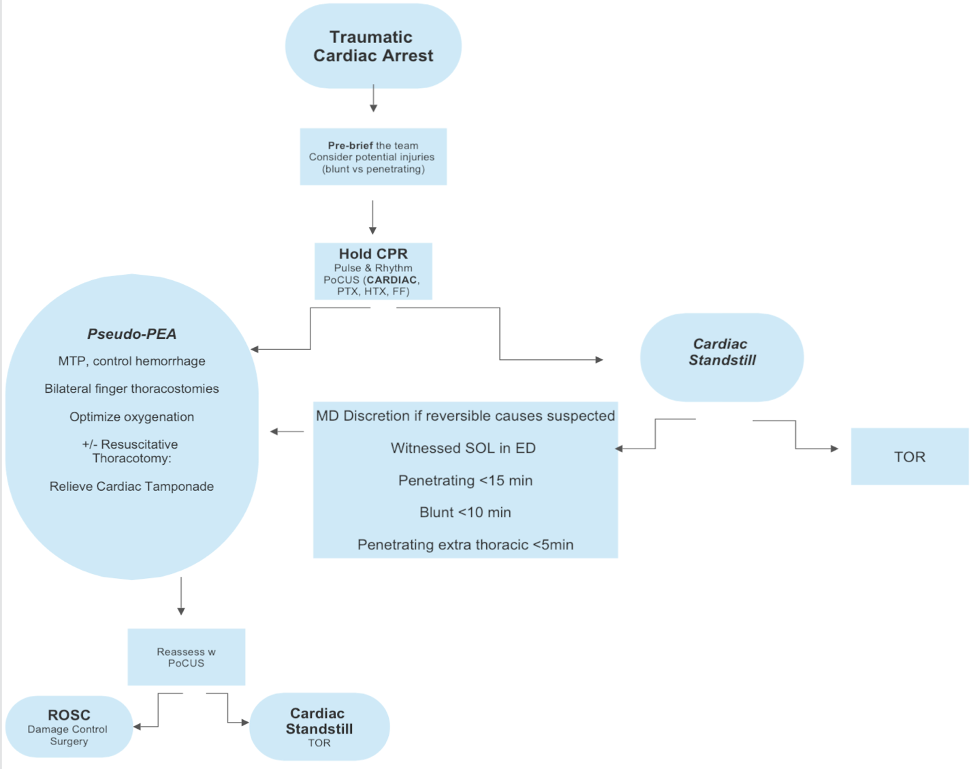
Goals in Traumatic Cardiac Arrest
- Ensure adequate oxygenation (importantly, avoid hypoxic episodes)
- Hypovolemia
- Massive transfusion
- Hemorrhage Control
- Obstructive
- Relieve tension hemo/pneumothorax
- Relieve cardiac tamponade
- Neurogenic
- Minimize cord injury/optimize perfusion
- Pseudo PEA
- Identify reversible causes of hemodynamic collapse
A Systematic review (SHoC investigators) of 8 studies involving 710 cases of TCA identified that all patients presenting in cardiac standstill were subsequently declared dead. They concluded that in patients with traumatic cardiac arrest without cardiac activity on POCUS, there is a near negligible chance of survival to hospital discharge. The study was limited by small sample size and therefore unable to make practice recommendations for termination of resuscitation based solely upon the absence of cardiac activity on POCUS, but it certainly echos clinical experience.
A systematic review looking at prognostic factors associated with survival to discharge, in patients in TCA:
- 53 studies (primarily retrospective and observational) involving 37 528 pts
- Identified that cardiac motion on PoCUS was the most important factor for survival with OR 33.91
Role of Chest Compressions
In medical cardiac arrests, High quality chest compressions result in approximately 25% baseline cardiac output in euvolemic patients. Patients in traumatic cardiac arrest, however, are often in hypovolemic or obstructive shock and have significantly lower cardiac output, so chest compressions are unlikely to have any significant impact on their cardiac output
Its been suggested that compressions may displace clot or worsen injury (chest wall, pulmonary, visceral). Compressions cause delay to potentially life saving treatment, and increase provider risk.
“CPR should be de-emphasized with the emphasis placed on correcting reversible causes of cardiac arrest” (ILCOR)
Bottom line:
No role for chest compressions in traumatic cardiac arrest (unless you suspect a treatable underlying medical etiology of their arrest)
Role of Epinephrine
As the trauma patient deteriorates, they have a massive catecholamine release (epinephrine, norepinephrine), causing widespread vasoconstriction until it reaches maximum levels. We know that epinephrine increases aortic diastolic pressure which increases coronary perfusion pressure, so in hypoxic traumatic cardiac arrest, epinephrine may be reasonable if oxygenation is addressed.
In hypovolemic or obstructive TCA, there is no obvious physiologic benefit to epinephrine, and the utilization of vasopressors may actually worsen their hemodynamics.
Bottom Line:
Consider the use of epinephrine if you suspect an underlying medical condition (based on historical features or shockable rhythms in field or on presentation to ED) and proceed with concurrent management of medical cardiac arrest and subsequent injuries. Do not prioritize epinephrine in TCA resuscitations otherwise
Intubation
Hypoxic traumatic cardiac arrest is rare outside of head, neck, facial injuries. Those patients require prompt ventilation and oxygenation. Do not delay addressing alternative reversible causes of arrest to intubate the TCA patient otherwise.
Remember that positive pressure ventilation causes a decrease in cardiac output, and most commonly traumatic arrest patients are in hemorrhagic/obstructive shock. PPV may worsen their pathophysiological process. An important consideration here is to resuscitate before intubating if time and current ventilation strategy permits.
Resuscitative Thoracotomy
The role of Resuscitative Thoracotomy
- Relieve cardiac tamponade
- Repair significant cardiac injuries
- Control massive pulmonary bleeding
- Relieve pneumothorax/hemothorax
- Repair aortic injuries
- Aortic cross clamping
Guidelines
- The WEST guidelines place a focus on the duration of CPR/arrest.
- The EAST guidelines focus on patient factors for survivability
The European Resuscitation Councilguidelines were published in 2021, and their traumatic cardiac arrest guidelines specifically address physiologic standpoint
Some of their recommendations, with regards to TCA:
- Focus on immediate simultaneous treatment of reversible causes
- TCA is different than MCA, which is addressed in their algorithm
- Use US to identify underlying cause of arrest and subsequent resuscitative measures
- Treating reversible causes takes priority over chest compressions
- Control hemorrhage
- Don’t pump an empty heart
BOTTOM LINE
- Do not delay addressing potentially reversible etiologies of arrest
- Hypovolemia and ongoing blood loss
- Penumothorax/hemothorax
- Cardiac tamponade
- No role for chest compressions
- De-emphasize epinephrine
- Carefully select patients to continue resuscitation on, to only those who may have reversible causes of their arrest
References
American College of Surgeons Committee on Trauma. Advanced Trauma Life Support : Student Course Manual. Tenth ed. American College of Surgeons 2018.
Atiksawedparit et al.: Effects of prehospital adrenaline administration on out-of-hospital cardiac arrest outcomes: a systematic review and meta-analysis. Critical Care 2014 18:463.
Burlew CC, Moore EE, Moore FA, Coimbra R, McIntyre RC Jr, Davis JW, Sperry J, Biffl WL. Western Trauma Association critical decisions in trauma: resuscitative thoracotomy. J Trauma Acute Care Surg. 2012 Dec;73(6):1359-63. doi: 10.1097/TA.0b013e318270d2df. PMID: 23188227.
Fierro NM, Dhillon NK, Yong FA, et al. No resuscitative thoracotomy? When to stop chest compressions after prehospital traumatic cardiac arrest. Am Surg. 2022;88(10):2464-2469.
Harris T, Masud S, Lamond A, Abu-Habsa M. Traumatic cardiac arrest: a unique approach. Eur J Emerg Med. 2015;22(2):72-78.
Khalifa A, Avraham JB, Kramer KZ, et al. Surviving traumatic cardiac arrest: Identification of factors associated with survival. Am J Emerg Med. 2021;43:83-87.
Lalande E, Burwash-Brennan T, Burns K, Harris T, Thomas S, Woo MY, Atkinson P. Is point-of-care ultrasound a reliable predictor of outcome during traumatic cardiac arrest? A systematic review and meta-analysis from the SHoC investigators. Resuscitation. 2021 Oct;167:128-136. doi: 10.1016/j.resuscitation.2021.08.027. Epub 2021 Aug 23. PMID: 34437998.
Lott C, Truhlář A, Alfonzo A, et al. European Resuscitation Council Guidelines 2021: Cardiac arrest in special circumstances. Resuscitation. 2021;161:152-219.
Nolan, J.P., Sandroni, C., Böttiger, B.W. et al. European Resuscitation Council and European Society of Intensive Care Medicine guidelines 2021: post-resuscitation care.Intensive Care Med 47, 369–421 (2021). https://doi.org/10.1007/s00134-021-06368-4
Seamon, Mark J. MD; Haut, Elliott R. MD, PhD; Van Arendonk, Kyle MD; Barbosa, Ronald R. MD; Chiu, William C. MD; Dente, Christopher J. MD; Fox, Nicole MD; Jawa, Randeep S. MD; Khwaja, Kosar MD; Lee, J. Kayle MD; Magnotti, Louis J. MD; Mayglothling, Julie A. MD; McDonald, Amy A. MD; Rowell, Susan MD, MCR; To, Kathleen B. MD; Falck-Ytter, Yngve MD; Rhee, Peter MD, MPH. An evidence-based approach to patient selection for emergency department thoracotomy: A practice management guideline from the Eastern Association for the Surgery of Trauma. Journal of Trauma and Acute Care Surgery 79(1):p 159-173, July 2015. | DOI: 10.1097/TA.0000000000000648
Smith JE, Rickard A, Wise D. Traumatic cardiac arrest. J R Soc Med. 2015;108(1):11-16.
Tran A, Fernando SM, Rochwerg B, Vaillancourt C, Inaba K, Kyeremanteng K, Nolan JP, McCredie VA, Petrosoniak A, Hicks C, Haut ER, Perry JJ. Pre-arrest and intra-arrest prognostic factors associated with survival following traumatic out-of-hospital cardiac arrest – A systematic review and meta-analysis. Resuscitation. 2020 Aug;153:119-135. doi: 10.1016/j.resuscitation.2020.05.052. Epub 2020 Jun 9. PMID: 32531405.
Watts S, Smith JE, Gwyther R, Kirkman E. Closed chest compressions reduce survival in an animal model of haemorrhage-induced traumatic cardiac arrest. Resuscitation. 2019;140:37-42.
Wongtanasarasin W, Thepchinda T, Kasirawat C, Saetiao S, Leungvorawat J, Kittivorakanchai N. Treatment outcomes of epinephrine for traumatic out-of-hospital cardiac arrest: a systematic review and meta-analysis. J Emerg Trauma Shock. 2021;14(4):195-200.
Yamamoto R, Suzuki M, Hayashida K, et al. Epinephrine during resuscitation of traumatic cardiac arrest and increased mortality: a post hoc analysis of prospective observational study. Scand J Trauma Resusc Emerg Med. 2019;27(1):74.

Trackbacks/Pingbacks