
I was in the OR for the first day of my anesthesia rotation when suddenly the pain hit me. It was in my left flank, radiating to my back — so much pain I could hardly think. A flurry of tests later, my ultrasound showed good doppler flow, and my lab work was pristine. I had a cyst on my ovary, but this wasn’t new. Feeling silly, I apologized for wasting the ER doc’s time.
“Not so fast, I want to call gyne…”
Before I knew it, I was waking up from surgery — I had ovarian torsion. I don’t know who was more shocked; the Gyne resident who said it probably wasn’t a torsion, or me, who totally thought the same thing.
As medical students, we are loyal disciples of evidence-based medicine and our modern imaging technologies; my experience was a firsthand lesson into the limitations of our clinical investigations, and what it means for something to be a clinical diagnosis. We all learn in medical school that unilateral pelvic pain in a reproductive-aged female is torsion until proven otherwise, but what exactly is “proven otherwise”, and when can we reliably rule it out/diagnose it/ when should we suspect torsion?
Why this matters
- We aren’t that great at diagnosing it
-
-
- Ovarian torsion is a clinical diagnosis, yet there is a wide variety of presentations and no specific pathognomonic symptom constellation.
- Most of its clinical signs lack sensitivity and specificity.
-
- We miss a lot
-
-
- Most of the tests we have for torsion aren’t sensitive enough.
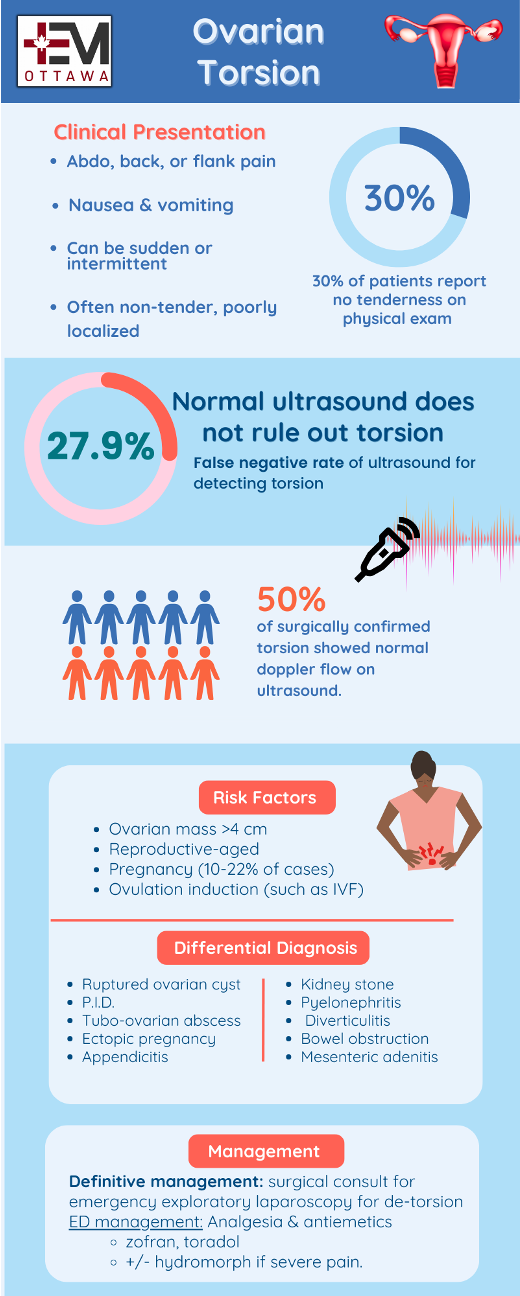
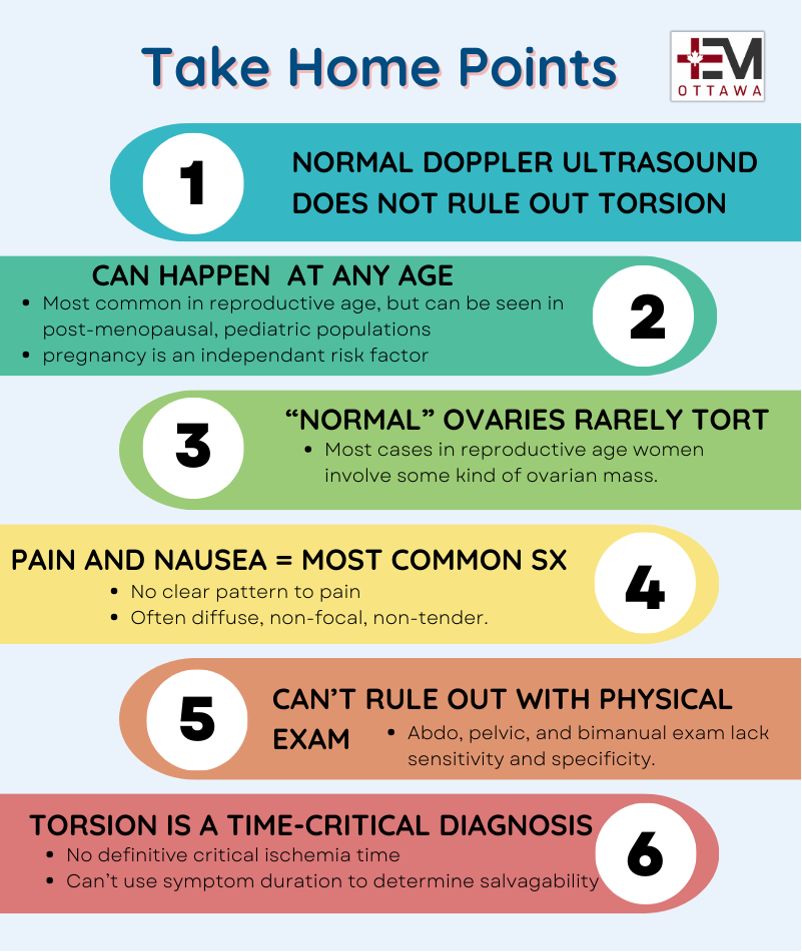
- Even ultrasound, our best option, has around a 27.9% false negative rate1 . We’d be freaking out if our best tests missed 27.9% of PEs.
-
- It’s rare, but not that rare:
- It’s still a time-sensitive, “life or limb” diagnosis
-
- Ovarian torsion is most common in reproductive-age women, and reproductive aged women generally want to keep their ovaries. A classmate on ObGyn at the time of my surgery said that upon hearing my case, the staff on call said she was coming in because “She’s 24, she needs her ovaries”. Can’t argue with that.
Background
Ovarian torsion occurs when the ovary twists around its suspensory ligaments, resulting in compression of the ovarian vessels. When the fallopian tube is also be involved in this twisting, this is termed adnexal torsion. This compression causes edema and ischemia, which are responsible for symptoms including severe pain and nausea, and can progress to necrosis if untreated.
The ovary has a dual vascular supply in both the ovarian and uterine arteries. In torsion, lymphatic and venous obstruction often occur first, causing edema and pain despite the presence of arterial flow.The main complication of ovarian torsion is the inability to salvage the ovary, which can have significant impacts on fertility.
Clinical Presentation
The classic clinical vignette of torsion is sudden-onset severe lower abdominal pain with nausea and vomiting. In reality, there is no reliable symptom pattern. While moderate to severe abdominal pain is the most common symptom, back and flank pain are also commonly reported. Only around 60% of patients report acute-onset, severe pain, and many patients may describe progressive onset or even episodic pain over a period of days to weeks, as seen in intermittent torsion5,6. Tachycardia secondary to pain and low-grade fever may sometimes be present. In pediatric populations, ovarian torsion may present as poor feeding, vomiting, irritability, and abdominal distension. Ultimately, while pain and nausea are the most sensitive signs of torsion, there is no consistent description of pain quality or radiation; it can be diffuse, non-focal, and is often non-tender.
Physical Exam
- Other than patients appearing uncomfortable, there are no consistent physical exam findings in torsion.
- Abdominal and pelvic exams for torsion lack both sensitivity or specificity, regardless of if they are whether performed by ER physician or ObGyn staff.7,8.
- Around 30% of patients will report no tenderness on abdominal or pelvic examination
- Bimanual exam is not useful for detecting masses less than 5 cm 6,11
While there are other benefits to doing pelvic exams in the ED, ruling out torsion is probably not one of them.
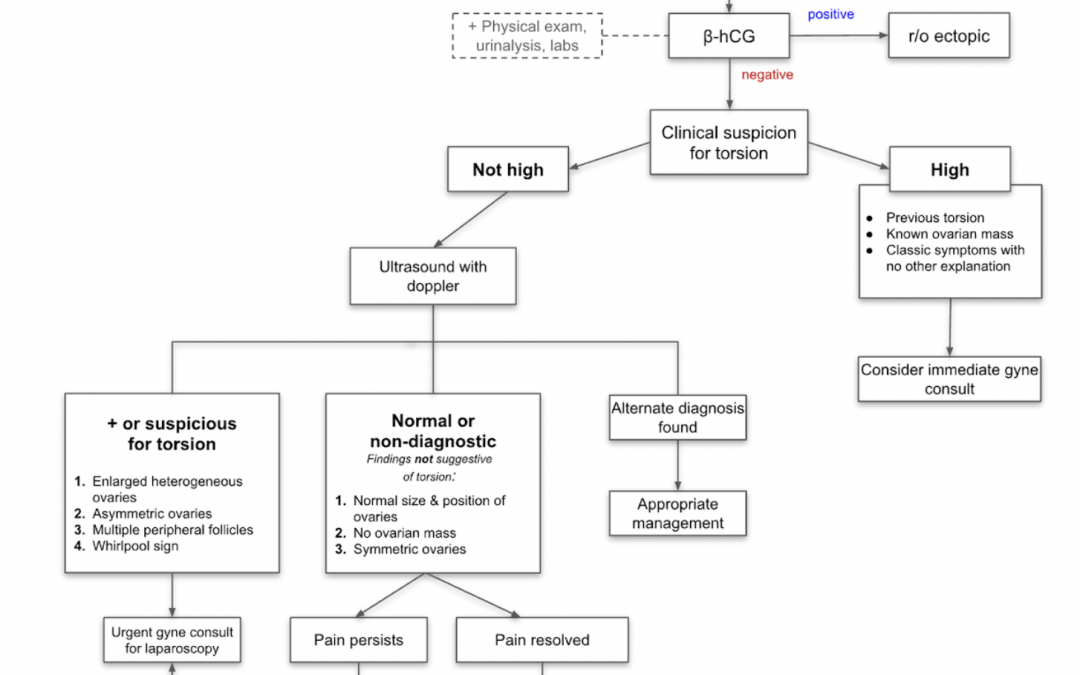
Investigations
The most important lab test in the workup of ovarian torsion is a beta-HCG to rule out an ectopic pregnancy. Otherwise, a CBC, basic metabolic panel, and urinalysis may be helpful in evaluating other causes, as well as serve as pre-op bloodwork.
Ultrasound
Transabdominal ultrasound with transvaginal views and doppler evaluation is the test of choice in the workup of suspected torsion. Ultrasound can be used to rule in the diagnosis of torsion, but can not reliably be used to rule it out. A 2014 study found that sonographers in a specialized ultrasound unit correctly diagnosed 72.1% of ovarian torsions, and missed 27.9% of them1. Estimates of false negatives increase to 50-70% when they include ultrasounds performed by populations such as physicians and medical residents. Don’t be reassured by good doppler flow; studies have showed that 50% of cases of surgically confirmed torsion showed normal doppler flow on ultrasound. 12
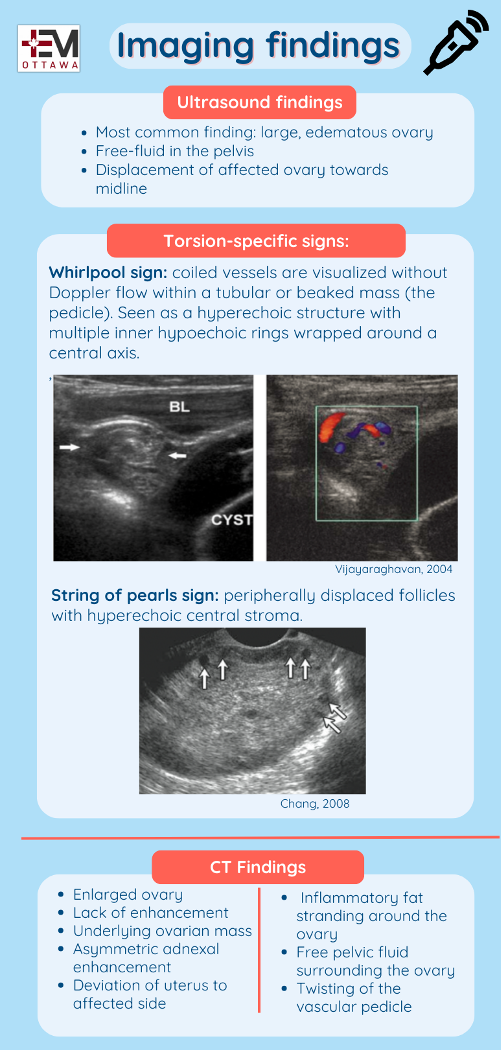
- Most common finding on ultrasound is a large, edematous ovary.
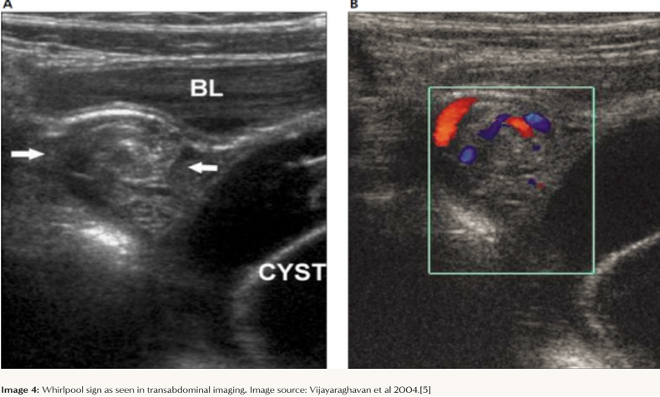
- The whirlpool sign, in which coiled or circular vessels are visualized without Doppler flow within a tubular or beaked mass (the pedicle), is pathognomonic for torsion.13
- Other signs include free fluid in the pelvis, displacement of the affected ovary towards the midline, and the “string of pearls” sign: peripherally displaced follicles with hyperechoic central stroma.
- Some additional resources on ultrasound can be found here and here
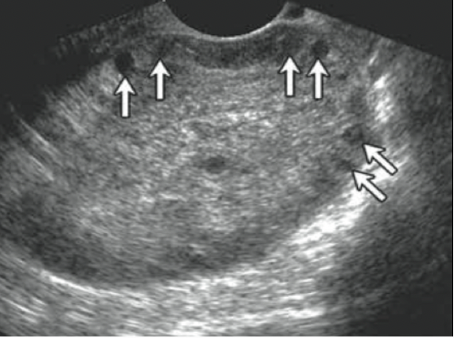
Ultrasound image showing the ‘string of pearls’ sign. 15
CT
While Ultrasound should always be the test of choice if torsion is suspected, there are still signs on CT with IV contrast that can suggest torsion; the most common being an enlarged ovary. This finding alone (with the correct clinical picture) is an indication for a ultrasound, if not already performed. Ofcourse, a CT may be helpful in ruling in other diagnosis such as appendicitis or nephrolithiasis.
CT findings of torsion16
- Enlarged ovary
- Underlying ovarian mass
- Lack of enhancement
- Asymmetric adnexal enhancement
- Deviation of uterus to affected side
- Inflammatory fat stranding around the ovary
- Free pelvic fluid surrounding the ovary
- Twisting of the vascular pedicle.
Management
- Definitive management is surgical consult for emergency exploratory laparoscopy for possible de-torsion
- Management in the ED is focused on supportive care:
- Analgesia +/- antiemetics: zofran, toradol, +/- hydromorph if severe pain.
What about critical ischemia time?
- While there is no definitive critical ischemia time for the ovary, ovarian torsion remains a time-sensitive diagnosis. Literature suggests a median of 3 days of symptoms (with a range of 0–60 days) to retain viability.2, 17 However, this is variable and assessed on a case-by-case basis; salvageability of the ovary should never be determined based on symptom duration alone.

References
- Rostamzadeh A, Mirfendereski S, Rezaie MJ, Rezaei S. Diagnostic efficacy of sonography for diagnosis of ovarian torsion. Pak J Med Sci. 2014 Mar;30(2):413-6. PMID: 24772154; PMCID: PMC3999021.
- Auer, J., R. Berent, and B. Eber. “Aortic dissection: incidence, natural history and impact of surgery.” Journal of Clinical and Basic Cardiology3.3 (2000): 151-154.
- . Pate JW, Richardson RL, Eastridge CE. Acute aortic dissection. Am J Surg 1976; 42: 395–404.
- Yuk, Jin‐Sung, et al. “A national population‐based study of the incidence of adnexal torsion in the Republic of Korea.” International Journal of Gynecology & Obstetrics 129.2 (2015): 169-170.
- White M, Stella J. Ovarian torsion: 10-year perspective. Emerg Med Australas 2005;17:231–237.
- Houry D, Abbott JT. Ovarian torsion: a fifteen-year review. Ann Emerg Med 2001;38:156–159. 3.
- Padilla, L A et al. “Accuracy of the pelvic examination in detecting adnexal masses.” Obstetrics and gynecologyvol. 96,4 (2000): 593-8. doi:10.1016/s0029-7844(00)00970-4
- Close, R J et al. “Reliability of bimanual pelvic examinations performed in emergency departments.” The Western journal of medicinevol. 175,4 (2001): 240-4; discussion 244-5. doi:10.1136/ewjm.175.4.240-a
- Padilla, L A et al. “Accuracy of the pelvic examination in detecting adnexal masses.” Obstetrics and gynecologyvol. 96,4 (2000): 593-8. doi:10.1016/s0029-7844(00)00970-4
- Close, R J et al. “Reliability of bimanual pelvic examinations performed in emergency departments.” The Western journal of medicinevol. 175,4 (2001): 240-4; discussion 244-5. doi:10.1136/ewjm.175.4.240-a
- Huchon C, Panel P, Kayem G, et al.. Does this woman have adnexal torsion? Hum Reprod 2012;27:2359–2364
- Nizar K, Deutsch M, Filmer S, et al.. Doppler studies of the ovarian venous blood flow in the diagnosis of adnexal torsion. J Clin Ultrasound 2009;37:436–439
- Chiou SY, Lev-Toaff AS, Masuda E, et al. Adnexal torsion: new clinical and imaging observations by sonography, computed tomography and magnetic resonance imaging. J Ultrasound Med 2007;26:1289–1301.
- Vijayaraghavan, S.B. (2004), Sonographic Whirlpool Sign in Ovarian Torsion. Journal of Ultrasound in Medicine, 23: 1643-1649. https://doi.org/10.7863/jum.2004.23.12.1643
- Chang, Hannah C et al. “Pearls and pitfalls in diagnosis of ovarian torsion.” Radiographics : a review publication of the Radiological Society of North America, Incvol. 28,5 (2008): 1355-68. doi:10.1148/rg.285075130
- Duigenan, S., Oliva, E., & Lee, S. I. (2012). Ovarian torsion: diagnostic features on CT and MRI with pathologic correlation. American Journal of Roentgenology, 198(2), W122-W131
- Ghandehari H, Kahn D, Tomlinson G, Glanc P. Ovarian torsion: time limiting factors for ovarian salvage. Emerg Med (Los Angel) 2015;5:5

Trackbacks/Pingbacks