
Introduction
Emergency health care places paramedics and healthcare providers are at the intersection of complex ethical considerations and legal obligations when addressing acute behavioural disturbances. The need for immediate treatment or physical/chemical restraint without patient consent can be challenging and requires a deep understanding of the legal frameworks that guide these decisions. This article examines the intricate interplay of consent, capacity, documentation, and the applicable legal statutes – the Health Care Consent Act (HCCA), the Mental Health Act (MHA), and the Ambulance Act with its embedded Basic Life Support Patient Care Standards (BLS-PCS) – in guiding the actions of prehospital healthcare providers in Ontario during critical situations.
Two Scenarios, One Complex Landscape
To better illustrate the complexities of this landscape, we will explore two distinct cases: the first involving Sarah, a 30-year-old woman in the midst of a severe mental health crisis, and the second concerning an elderly woman, Mrs. Jones, who resides in a Long-Term Care Home (LTCH) with advanced dementia and a lack of capacity. In both cases, the application of legal statues, professional judgment, and meticulous documentation are essential to ensure appropriate care while respecting the rights and safety of the individuals involved.
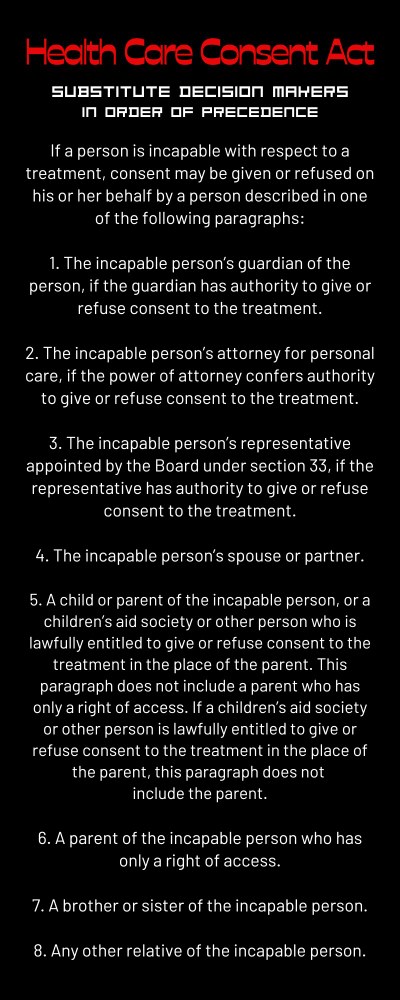
“A person may be incapable with respect to some treatments and capable with respect to others.”
– Health Care Consent Act
Case 1: Sarah’s Crisis and the Interplay of HCCA, MHA and Documentation
Paramedics are called to a residential address where Sarah is in acute distress. She is emotionally labile, agitated, and posing a safety risk to herself, threatening to commit suicide. Sarah’s deteriorating mental state and self-endangering behaviour necessitate immediate intervention, but she is not cooperative with the assessment or recommendation to come to the hospital. Paramedics determine that an emergency exists, and that Sarah’s life and health are in immediate danger if they do not intervene. Sarah’s refusal to cooperate with the recommended plan prompts a crucial assessment of her capacity to provide consent or refusal of treatment. Sarah has a Glasgow Coma Scale (GCS) score of 15; however, her fragmented responses and inability to grasp the risk at hand present a challenging decision for the paramedics. Her case falls within the purview of both the Health Care Consent Act (HCCA) and the Mental Health Act (MHA).
Under the HCCA, paramedics can assist in providing the right care for Sarah by engaging a substitute decision-maker (SDM) to provide consent for treatment and transportation, since Sarah is not capable of understanding the risks of refusing care and therefore cannot provide an informed refusal that would meet the standard and be defensible if there was a negative outcome. A typical SDM would be a spouse, parent, adult child, or sibling. If an SDM is not available to provide consent, paramedics may treat and transport without consent because an emergency exists and the delay to obtaining consent will endanger Sarah’s life and health. Alternatively, under the MHA, police have the authority under Section 17 to apprehend, and transport to hospital, individuals who pose an acute safety risk to themselves or others as a result of mental illness. In this case, by collaborating with the SDM and the police, paramedics provide appropriate and safe treatment and transportation for Sarah without her consent but in compliance with the law and her best interests.
The importance of documentation cannot be overstated in this context. Treating and transporting patients without consent can leave the paramedic vulnerable to allegations of misconduct, unethical, unprofessional, and even illegal activity. Comprehensive and accurate documentation of Sarah’s condition, the determination that an emergency exists, the assessment of her capacity, attempts to contact an SDM for consent, the involvement of law enforcement under MHA Section 17, and the rationale behind any treatment or restraint administered is vital. This documentation not only supports the decision-making process but also ensures that critical information follows the patient, facilitating continuity of care and effective communication among healthcare providers.
Case 2: Ethical Dilemmas in Long-Term Care and the Role of Documentation
Transitioning to the case of the elderly woman in the Long-Term Care Home, we encounter a different facet of the consent and capacity challenge. Paramedics are called to the Long-Term Care Home where Mrs. Jones, an elderly lady with a history of dementia and cognitive decline, is experiencing an acute behavioural disturbance. Staff report that she is normally confused at baseline, but over the past 24 hours there has been a marked change. She has become increasingly resistant to care, agitated, hallucinating, and febrile. Mrs. Jones refuses assessment and swings out defiantly when paramedics attempt to check her blood sugar.
Recognizing that fever and delirium herald a serious medical concern, and that Mrs. Jones does not have capacity to understand the risks of refusing care, paramedics speak with her daughter who is her SDM. Her daughter consents to transportation to the hospital, after discussion about the risks of physical and chemical restraint. Many Long-Term Care Homes have dedicated healthcare providers (doctors, nurse practitioners, nurses, etc.) who can assist in decisions regarding the care of patients who are assessed as lacking capacity. Paramedics inquire if there are any PRN (as needed) sedatives ordered by the Long-Term Care Home physician for Mrs. Jones in these situations. Nurses provide Olanzapine 2.5mg PO as per their PRN standing order. Paramedics prepare a small dose of sedation to be given IM if needed. Mrs. Jones is gently coaxed onto the stretcher and transported to the hospital. In this case, the HCCA provides legal authority for treatment and transportation without consent of the patient, as the daughter acts as the SDM and balances her mother’s best interests, goals of care, sedation, and the use of force, among other considerations.
“When treating without the consent of the patient, thorough and meticulous documentation is ESSENTIAL”
In this context, documentation serves as a crucial tool to capture the daughter’s informed decisions as the SDM, the reasoning behind her choices, and the measures taken to provide care consistent with the HCCA. This documentation not only supports the daughter’s role but also ensures that healthcare providers have a clear understanding of the patient’s history and preferences, enabling them to deliver care that aligns with both the law and the patient’s well-being.
The Basic Life Support Patient Care Standards
The BLS-PCS references both the HCCA and MHA as statutes that paramedics (and all healthcare providers) are legally obliged to comply with. While the HCCA and MHA address the majority of situations involving consent, capacity, and mental health, the BLS-PCS embedded within the Ambulance Act offers additional guidance for paramedics in emergency situations. The BLS-PCS independently authorizes paramedics to use physical restraint without consent if a patient becomes violent during transportation.
Navigating the Legal Frameworks and Documenting the Journey
When treatment is provided without the consent of the patient, thorough and meticulous documentation is essential. Documenting assessments, decisions, communications with patients and their SDMs, as well as the rationale behind treatment and restraint, ensures that the journey of patient care is well-documented and transparent. This documentation not only benefits patients and providers in individual cases but also contributes to the continuous improvement of protocols and practices within the emergency healthcare system.
Conclusion
The intricate narratives of Sarah’s crisis and Mrs. Jones’ situation underscore the complex interplay between ethics, legality, compassionate care, and documentation in the realm of acute behavioural disturbances. Paramedics, healthcare providers, and law enforcement officers shoulder the responsibility of making critical decisions under difficult circumstances, always prioritizing patient welfare and respecting the law. The HCCA, MHA and BLS-PCS collectively provide essential guidance for navigating these challenges.
As healthcare providers navigate the delicate terrain of consent, capacity, documentation, and acute behavioural disturbances, their unwavering dedication to patient well-being and the principles of informed, responsible care shines as a beacon of compassion and professionalism within the realm of emergency healthcare. The meticulous documentation they provide ensures that patient information follows the individual, enabling seamless care transitions and supporting the overarching goal of delivering optimal care in complex and dynamic situations.

