

Mechanical ventilation has a lot of nuance associated with it, but a lot of reference guides focus on care in the ICU. There is certainly a need for more practical application for the ED doc or initial setup of patients on the vent. With both ER and ICU experience, this post acts as a quick summary guide, but is certainly not comprehensive. As with anything mechanical ventilation, there is a tonne of nuance.
This is a two-part series, with the first part focusing on basics of ventilator setup and physiology, and part 2 with a focus on lung protective ventilation.
Terminology and Concepts
PEEP (positive end-expiratory pressure) = EPAP (name for PEEP on a bipap machine)
-
- PEEP is an amount of pressure applied to the airway at the end of expiration. Why do this? On expiration, the elastic forces of the lungs result in net forces that want the alveoli to collapse. Pressure (PEEP) helps stent open collapsed airways. In patients suffering from pneumonia, atelectasis, pulmonary edema, aspiration, etc. the airways are filled with debris (fluid, protein, blood, pus) and because of this are ineffective at gas exchange – they’re filled with stuff, so oxygen can’t get in to participate in exchange. PEEP can help open these diseased alveoli to allow better flow to O2 into them in order to participate in gas exchange. This is why PEEP helps improve oxygenation. Too much PEEP however can lead to overdistention of the lung causing barotrauma.
— - CPAP (continuous positive airway pressure) – a constant pressure applied to the respiratory system during inspiration and expiration. Conceptually this does the same function as PEEP.
— - Inspiratory pressure (on a vent) = IPAP (on a BiPAP machine) = pressure support (on a vent in spontaneously breathing patients). This is the pressure delivered by a ventilator/BiPAP with each inspired Pressure support helps to ‘support’ each breath. By adding pressure, we reduce the amount of work the patient has to do to inhale, thus reducing the work of breathing. IPAP also helps overcome disease states of high resistance and low compliance – if you have very stiff lungs from ARDS you will need more pressure with each breath to get air in because the stiff lung is difficult to inflate.
— - Compliance= change in volume/ change in pressure. Typical HIGH compliance state = COPD- these lungs are damaged and suffer from emphysema where the alveolar units are baggy and floppy. It takes very little pressure to fill these lungs up. Typical LOW compliance state = ARDS- these lungs are stiff, it takes a lot of pressure to get a small amount of volume into these lungs
— - Resistance = change in pressure/ change in flow. Typical high resistance state = asthma where the alveoli are normal and non-diseased but the conducting airway (bronchioles) are constricted and very tight due to bronchospasm, smooth muscle hypertrophy and mucus plugging). The more constricted the more resistance to flow (remember flow is inversely proportional to radius^4)….ahhh math!
— - Plateau pressure (more on this below): this is the pressure in the airway at the END of inspiration. This is the pressure that the alveoli are exposed to. It is the pressure needed to open the alveoli and overcome the elastic recoil forces of the lung tissues and chest wall.
— - Peak pressure (more on this below): maximum pressure required to deliver a breath during inspiration. It is a summation of resistive forces to airflow and elastic forces of the lung tissue/chest wall
—
- PEEP is an amount of pressure applied to the airway at the end of expiration. Why do this? On expiration, the elastic forces of the lungs result in net forces that want the alveoli to collapse. Pressure (PEEP) helps stent open collapsed airways. In patients suffering from pneumonia, atelectasis, pulmonary edema, aspiration, etc. the airways are filled with debris (fluid, protein, blood, pus) and because of this are ineffective at gas exchange – they’re filled with stuff, so oxygen can’t get in to participate in exchange. PEEP can help open these diseased alveoli to allow better flow to O2 into them in order to participate in gas exchange. This is why PEEP helps improve oxygenation. Too much PEEP however can lead to overdistention of the lung causing barotrauma.
Modes and Types of Breath
- There is no one ventilator mode that is ‘the best’, save for some very nuanced cases. In the ED you can ventilate your patients in any controlled mode. What IS important is to understand that in each mode you have dependent and independent variables – that is things you control and things that are the consequence of the parameters you set as well as the underlying disease state of the patient. By understanding these variables you can titrate your vent settings to effectively ventilate the patient
- On that note, I spent the first two years of residency assuming there is a standard set of vent settings …. This is not true at all! All vent settings are individualized! This is why Rosen’s doesn’t give you a set of numbers to memorize as “standard vent settings”. It doesn’t exist folks.
Types of breaths – *Fundamental Concept*
Understanding modes starts with understanding the different types of breaths that can be delivered- controlled, assisted, or supported.
- Controlled breaths: the ventilator does all the work. The ventilator gives a set number of breaths per minute with set parameters for each of those breaths.
- Assisted breaths: the patient initiates the breath which is sensed by the ventilator. The ventilator then kicks in and performs most of the work delivering a full ventilator breath. In this way the patient can set their own respiratory rate, but the ventilator settings can determine the amount of volume given or the pressure used to force in a breath. You can imagine in a patient who is weak, fatigued or aLOC they may not be able to get the volume of air they need with each breath, so this is a way to for them to ‘breathe’ on their own but the vent is making sure their minute ventilation is adequate.
- Supported breaths: Here the patient does most of the work with some help from the ventilator.
Controlled modes
- Controlled modes deliver controlled/assisted breaths. These are modes in which the ventilator performs all of the work to deliver a breath. Set a specific respiratory rate and that guarantees that every minute we will have a certain number of full mechanical breaths delivered to the patient.
Volume control Mode aka AC/VC or VC
- In this mode you are targeting a set VOLUME to be delivered to the patient with each breath.
- Parameters you must set:
- Tidal volume (in general target 6-8mL/Kg of IDEAL BODY WEIGHT)
- FiO2- start at 100% and titrate down to an appropriate oxygen saturation
- PEEP –5-10cmH2O is a good starting point for most patients
- Respiratory Rate –variable based on the pathology; start at 12-18 breaths/min
- Inspiratory flow rate -(will discuss more when talking about I:E ratio, in general just leave at the default vent settings)
- What does VC mean?
- It means that if we set a specific RR and tidal volume, e.g 12 R breaths per min and 500mL tidal volume, that 12 times per minute the patient will get 500mL of tidal volume. Their minute ventilation will therefore be 6L/minute.
- AC:VC vs VC ….. oh man more terms
- Strict volume control (old school vents) will give ONLY what you set on the ventilator- i.e if you set 12 breaths per min at 500mL the patient gets only 12 breaths in that minute and 500mL per breath
- Assist control (AC) means that at a minimum the patient will get your set parameters (e.g 12 breaths per min at 500mL per breath) BUT the patient can spontaneously breathe above that set rate such that then each time the patient breaths the ventilator will deliver a FULL ventilated breath (500mL) … as an example, you set your vent at 12 breaths per min at 500mL per breath. But the patient is breathing at 16 breaths per minute. So your ventilator will synch its mandatory 12 breaths per minute with the patient’s needs by sensing that the patient is trying to take a breath. When the patient takes a breath, the machine realizes this and delivers a full tidal volume (500mL breath). For the 4 additional breaths per minute, the machine will also sense these and deliver a full tidal volume 500mL breath. However, if for some reason the patient is now sedated for a procedure and breathes at 6 breaths/minute, the machine will automatically deliver 12 breaths per minute at 500mL each breath.
- We almost always use ACV rather than VC when doing volume control ventilation (it is quite rare to use strict VC mode)
- What can we not control in VC modes?
- PRESSURE! Your vent will deliver your set tidal volume at the cost of doing it at whatever inspiratory pressure is necessary. Remember, too high pressure however can be damaging to the lung. Sudden changes to the circuit/lung resistance (mucus plug, bronchospasm) or the lung compliance (pulmonary edema, pneumothorax) will result in PRESSURE changes but not necessarily a change in volume, as this is a set parameter. Hence changes to your patient are reflected in changes in pressure (dependent variable) NOT volume (independent variable)
Pressure Control aka PC or AC/PC
- If volume control sets a volume at the cost of unknown pressure then pressure control is the opposite. Here we set an inspiratory pressure and the dependent variable will be the volume delivered. The nice thing about PC is that we know the pressure applied to the lung so we can limit pressure injury, but we have to closely monitor the volume. In this mode, changes to the resistance of the circuit (mucus plug) or compliance of the lung (pulmonary edema) will result in LOSS OF VOLUME but the pressure will remain constant.
- Pressure control settings
- Tidal volume- again 6-8 cc/kg IBW
- RR
- PEEP
- FiO2
- Inspiratory pressure – in general start with 15-20cmH2O and assess if this provides adequate volumes for your patient
- Inspiratory Time- how quickly inspiration occurs. 1 to 1.5seconds
- A nice thing about pressure control is you determine your peak pressure. For example, a patient with inspiratory pressure of 20cmH2O and a PEEP of 10cmH2O will have a PEAK pressure of 30cmH2O
- Once again there is strict PC and AC/PC. AC/PC like AC/VC allows the patient to breath spontaneously getting a full ventilator breath each time where as strict PC will only give as many breaths per minute as you set.
Spontaneous Modes
Pressure support/CPAP
- Probably the easiest to conceptualize. You have a patient spontaneously breathing for whom you can deliver CPAP to help stent open the airways. At the same if your patient has increased work of breathing or perhaps is weak and needs ‘support’ for each breath you can ADD inspiratory pressure a.k.a pressure support (PS)! Now think about it for a second, if you have one pressure applied during inspiration and a set pressure on expiration what is that called …… BIPAP! So PS/CPAP can be thought of as using ‘CPAP’ or ‘BIPAP’ depending on if you use pressure support or not.
Not confused enough? ..Here comes SIMV (Synchronized Intermittent Mandatory Ventilation)
- Admittedly this would be highly uncommon to use in the ED for patients given that we typically are doing RSI intubations and patients don’t hang around in the ED for long
- But SIMV is the combination of PS/CPAP and a controlled mode. SIMV can be either volume or pressure-controlled just as we have discussed above PLUS you can set a pressure support
- SIMV is used for patients who can spontaneously breathe but are not strong enough or awake enough to meet their minute ventilation needs; it can also be used in the patient without spontaneous respiration but at this point, it is simply acting as a controlled mode
- The ventilator will give a mandatory number of breaths per minute that are fully ventilator breaths – i.e at the volume or pressure you set; You pick a respiratory rate, and the ventilator will try to synchronize its mandatory delivered breaths with the patient’s effort to deliver those full machine breaths when the patient wants to take a breath. The patient can breathe spontaneously between these breaths (with or without pressure support), however the volume of spontaneous breaths is determined only by the patient effort (patient-driven) not by machine settings i.e. the spontaneous breaths are not full mechanical vent breaths.
- What do you set:
- You will pick to either put them on volume or pressure control settings
- Pressure support
- I wouldn’t spend much time learning about SIMV. This is not really a mode for the ED
And just to be more confused …… there are MANY different modes than what is listed above- PRVC, VC+ APRV Bilevel PAV etc etc … while all are used with some frequency in the ICU setting, these modes require a very specialized understanding of mechanical ventilators and respiratory physiology as well some require more invasive monitoring. These are not modes you should be reaching for in the ED.
So do I pick volume or pressure mode? In the ED for those minutes to hours the patient is in our resus room, the answer is it doesn’t matter. Understanding what variables you choose and don’t choose in each mode is much much much more valuable and important. If you are interested in the subtle nuance of VC vs PC here is a link to deranged physiology. Bottom line, in the ED pick one you’re familiar with and know how to use. Leave more advanced vent settings for when the patient is in the ICU/when the respiratory therapist is around to titrate the vent.
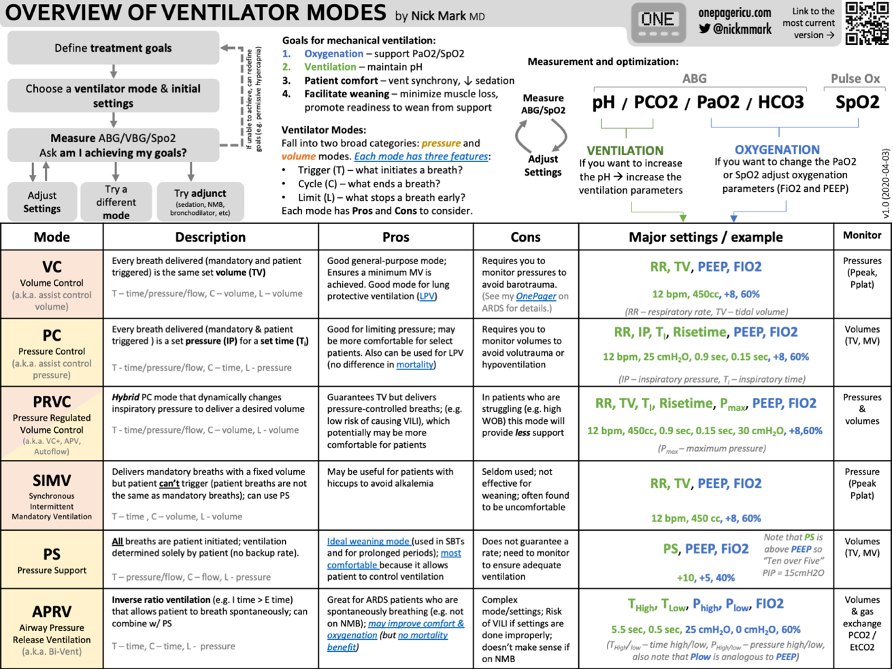
Taken from ICU one pager
*APRV and PRVC are modes you would not use in the ED, however, you may commonly see PRVC in the ICU setting and less so APRV. PRVC is a combo of PC and VC which adjusts the inspiratory pressure each breath titrated to give a specific volume (if there is an increase in resistance or compliance suddenly the ventilator can adjust itself to keep the tidal volume consistent).
What are ‘standard’ settings?
- I tried to discover this for years only to find out it doesn’t exist … mechanical ventilation is titrated to the patient. But alas you have exams to take so on the exam you write:
- Volume control:
- RR 12-18
- FiO2 100% then titrated to sats of 94-98%
- PEEP 5-10 cmH2O
- Tidal volume 4-8mL/kg IBW (just say 6 on your exam)
- Inspiratory flow rate 60-100L/min…. for most patients 60L/min as a starting point is good
- Pressure control:
- RR 12-14
- PEEP 5-10 cmH2O
- Inspiratory pressure 15-20 cmH2O
- FiO2 100% then titrate to sats 94-98%
- Inspiratory time 1-1.5 seconds
Ventilator Waveforms
- Analysis of waveforms are beyond the scope of this, but important to take note of. Waveforms are different based on the mode of ventilation. You will notice a pressure vs time curve on the top; a flow vs time curve in the middle and a volume vs time curve on the bottom.
Typical waveforms in volume control ventilation modes:
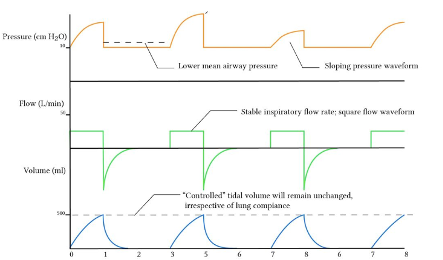
Image from Deranged Physiology
Typical waveforms in pressure-controlled ventilation modes:
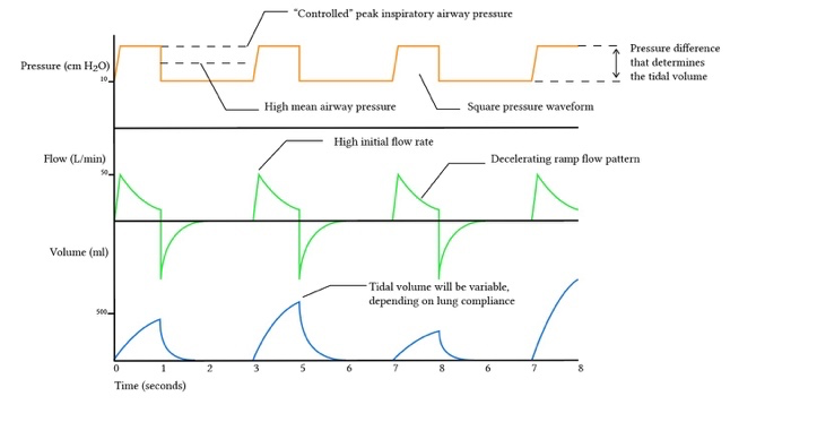
Image from Deranged Physiology
Typical waveforms in SIMV modes:
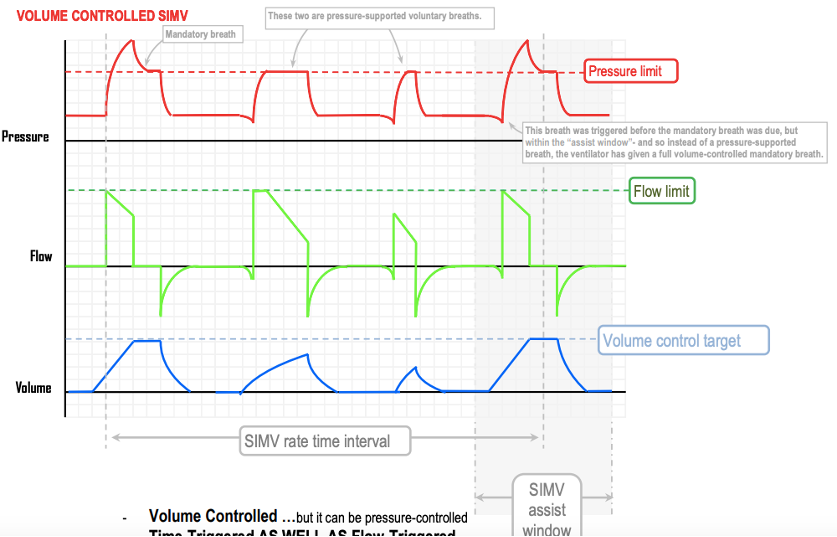
Image from Deranged Physiology
Check out part two on lung protective ventilation strategies!

Hello very well written valuable info. Can we improve metabolic acidosis by vent settings.