
In our first part, we talked about the basics of mechanical ventilation and how to set up the ventilator for the busy ED doc! In part two, we discuss lung protective ventilation and go through a few cases to help solidify what we’ve learned. If you haven’t read part one – check it out here!
ARDS – Acute Respiratory Distress Syndrome
- What is ARDS? Really, this is not an ED diagnosis. But in general, think about this for patients you see with acute bilateral airspace disease (not related to cardiogenic pulmonary edema) and significant hypoxemia. ARDS is a state of lung inflammation resulting in non-compliant (stiff) lungs. ARDS patients are prone to ventilator-induced lung injury and barotrauma due to reduced compliance and the heterogenous nature of their disease- the non-diseased lungs are more compliant than the disease segments which means that different alveoli will tolerate changes in pressure and volume better than others –> some alveoli will not fill, some will fill quite well, some will overdistended
What is lung protective ventilation?
-
- Terminology used to describe modern-day mechanical ventilation of patients with lung parenchymal disease (pneumonia, pulmonary edema etc). The idea is LOW tidal volume ventilation (to reduce risk of ventilator-induced lung injury) and keeping specific pressure parameters to reduce the risk of barotrauma
- Components of lung protective ventilation:
- Tidal volume: 4-8mL/kg of ideal body weight
- Titrated PEEP (there are many ways to do this which are all debated and outside the scope of this document)
- FiO2 titrated to what is tolerable for patient’s physiology. Typically targeting O2 stats of 88-95%
- Plateau pressure <30cmH2O
- Driving pressure <15 cmH2O
- Permissive hypercapnia when needed (target pH 7.2 or higher)
- Components of lung protective ventilation:
- Terminology used to describe modern-day mechanical ventilation of patients with lung parenchymal disease (pneumonia, pulmonary edema etc). The idea is LOW tidal volume ventilation (to reduce risk of ventilator-induced lung injury) and keeping specific pressure parameters to reduce the risk of barotrauma
What is plateau pressure and what is driving pressure?
-
-
- Assume that you’re ventilating someone in volume control mode with ARDS and stiff lungs. You’re trying to give them 500mL/breath of tidal volume but every time you attempt this the alarms go off reading high pressure. Why do we care about high pressure? With stiff lungs, higher pressure runs the risk of barotrauma (e.g., pneumothorax). It is important to keep an eye on the pressure the lung is subjected to in order to reduce the risk of injury.
- The pressure alarm that is ringing off is the PEAK. PEAK pressure is more a measure of the resistance of the circuit/airway and conducting airways AND the elastic properties of the lung/chest wall, it is not necessarily the pressure that the alveoli are subjected to, which is the pressure we truly care about
- Peak pressure may be elevated due to high resistance, but this pressure is dissipated throughout the circuit and conducting airways such that by the time air reaches the alveoli the pressure the alveoli see is less than the peak pressure.
- How do we know the pressure the alveoli see? This is measured via Plateau pressure. Plateau pressure = pressure at the END OF INSPIRATION, measured during an inspiratory hold maneuver. To get a plateau pressure, on your vent, you will have to do an “inspiratory hold”- most vents will have a button specifically for this. Note, patients should be sedated, paralyzed, and fully ventilated, i.e. not spontaneously breathing, to get an accurate plateau.
- Keep plateau pressure <30cmH2O
- The pressure alarm that is ringing off is the PEAK. PEAK pressure is more a measure of the resistance of the circuit/airway and conducting airways AND the elastic properties of the lung/chest wall, it is not necessarily the pressure that the alveoli are subjected to, which is the pressure we truly care about
- Assume that you’re ventilating someone in volume control mode with ARDS and stiff lungs. You’re trying to give them 500mL/breath of tidal volume but every time you attempt this the alarms go off reading high pressure. Why do we care about high pressure? With stiff lungs, higher pressure runs the risk of barotrauma (e.g., pneumothorax). It is important to keep an eye on the pressure the lung is subjected to in order to reduce the risk of injury.
-
Driving pressure: Difference between the plateau pressure and the PEEP =<15cmH2O. this is the pressure driving air into the alveoli
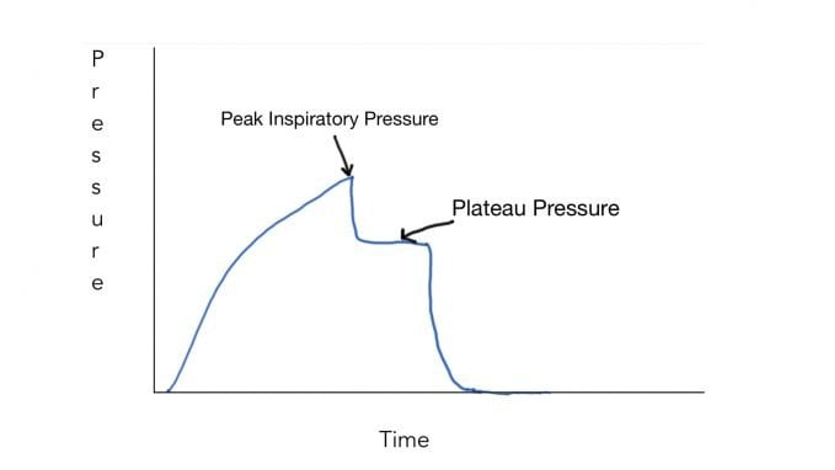
From Deranged Physiology
- This is a pressure-time curve in volume control mode showing the difference between peak pressure and plateau pressure (measured with an inspiratory hold maneuver), note how the two pressures are not the same. Peak pressure tends to overestimate the pressure the alveoli are exposed to! Plateau pressure is a function of lung compliance- where low compliance will elevate plateau pressure
“My patient’s high-pressure alarm won’t stop going off!”
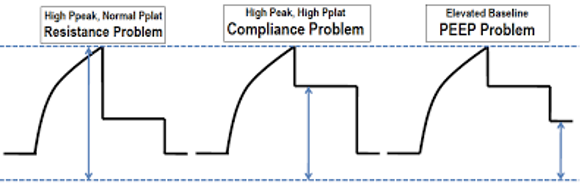
From Deranged Physiology
- Graphically, you can look at your Pressure time curve and use an inspiratory hold to determine if the patient which high ventilator pressures are attributable to a resistance problem (tube obstruction, bronchospasm), a compliance issue (ARDS, pneumonia, edema, penumothorax, or both.
- If you have High peak pressure but normal plateau pressures (plat <30cmH2O) this is a resistance problem:
- Kinked tube
- Mucus plug
- Dislodged tube
- Bronchospasm
- If you have both high peak pressure AND elevated plateau pressure you have. Compliance problem (a stiff lung)
- PTX
- Pulmonary edema
- Pneumonia
- Hemothorax, pleural effusion
- Abdominal compartment syndrome
- Atelectasis
Mechanical Ventilation of Specific Clinical Scenarios
- Understanding what a ventilator does and doesn’t do helps you understand how to mechanically ventilate your patient
- A ventilator does 2 things: 1) it oxygenates; 2) it ventilates. That’s it! So, if you can approach the vent by trying to break it down into those two categories you can help troubleshoot the vent.
- Below is a simplified way to approach oxygenation and ventilation, as of course there are several areas of nuance but those are beyond the scope of what we would normally do in the ED
- How to optimize oxygenation on a vent?
- Increase FiO2
- Optimize PEEP (notice how I don’t say increase)
- ^ First steps in the ED
- In the ICU:
- Optimize ventilatory settings/mode, optimize mean airway pressure, optimize PEEP
- Prone positioning
- Inhaled pulmonary vasodilators
- How to optimize ventilation on a vent?
- Recall minute ventilation = RR x tidal volume
- You can optimize ventilation by adjusting either your respiratory rate or your tidal volume
- ^ in the ED these are the things you should adjust
- In the ICU:
- Optimize ventilatory settings/mode
- Prone positioning
- Inhaled pulmonary vasodilators
Example Case 1
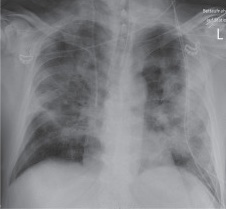
Consider a 55M who presents with COVID pneumonia and bilateral airspace disease. You intubate him and start AC/VC ventilation with settings: RR 15, FIO2 100%, PEEP 5cmH2O, flow 60L/min, and tidal volumes of 500mL. Despite this, he remains hypoxic with sats of 80% post-intubation.
Think through this case. How will you optimize this OXYGENATION in the ED?
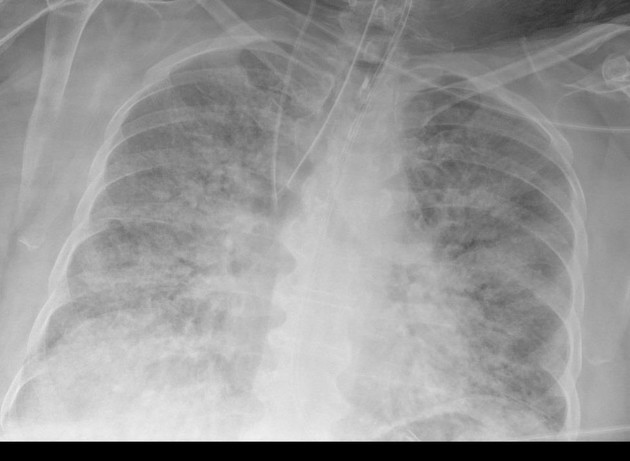
Image from radiopedia
Answer: INCREASE THE PEEP
- In this case the patient is already on 100% FIO2 so there is no room to work there. He has significant bilateral airspace disease so his alveoli are filled with pus/fluid and are thus not participating in gas exchange. 5cmH2O is likely not enough PEEP for him. He needs more end expiratory pressure to open up his airways
- You increase his PEEP to 10cm H2O and his sats improved to 94% and repeat CXR looks like the following: you can see how PEEP has opened up some lung parenchyma to participate in gas exchange
Example Case 2: 23F with no pmhx who presents altered level of consciousness with a suspected opioid overdose but is not Narcan responsive. RR is 4. She’s saturating OK on NRB but VBG shows CO2 >110. Her CXR is clear of any parenchymal disease. You elect to intubate her for airway protection and hypercarbic respiratory failure. Think about how you would adjust your ventilator settings for hypercarbia
—-
Answer: due to her opioid overdose she has low minute ventilation from low RR and hence her CO2 is through the roof. Minute ventilation=RR x tidal volume. By adjusting either of these variables will increase minute ventilation and reduce the CO2. Adjusting either is reasonable, you can also adjust both. I would opt to put her on :
- AC/VC: Tidal volume 500
- RR 20
- PEEP 5
- Fio2 100% (then adjust to sats)
- Flow rate 60L/min
- I would follow her VBGs q1h to ensure that I am improving CO2. If little or no improvement options would be to increase tidal volume or increase RR further.
COPD – Example Case
Example case 65F with COPD not on home O2. Presents with 3 days of URTI symptoms. She comes in with severe respiratory distress, wheezing, moving minimal air on exam, hypoxic requiring NRB with sats of only 85%, BP 90/70 HR 135 sinus, RR 35. You start neb of Atrovent and Ventolin, IV steroids, IV fluids and IV antibiotics quickly. Her CXR is unremarkable. Her initial VBG shows 7.25/85/32/50 lactate 3
Despite your treatment, one our later her VBG is 7.2/100/30/50 lactate 3.3. Her LOC is decreasing and you decide to intubate. Think about how you would ventilate this patient.
Answer (this is a long one) …
Much like the patient in the example prior, patients with COPDe will often be hypercarbic. But as you may have noticed, this patient was breathing at 35 (not RR of 4 like the last patient) so how the heck is her CO2 so high? Patients with COPD have significant airflow obstruction due to bronchospasm of the airways. They also have floppy, very compliant alveolar units which are prone to overdistention due to emphysema. With emphysematous destruction of alveoli, the lung loses its elastic recoil- thus even when overdistended with air the alveolar unit does not easily collapse back to its baseline volume. The combination of the properties of high compliance (overdistended alveoli without elastic recoil) and high resistance to airflow (due to bronchospasm) means that EXPIRATION is highly impaired. For these patients it takes significantly LONGER to expire the same volume of air as a normal lung. So even with a high respiratory rate they have impaired minute ventilation because air is simply not escaping as quickly as it should.
Your goals with intubation of the COPDer is to give them some rest as their respiratory muscles have been running a marathon, give them time to expire and blow off that CO2 and give time for all your meds (bronchodilators and steroids) to kick in. Paradoxically, you will likely require a LOWER respiratory rate than the respiratory rate the patient had on their own pre-intubation.
Why would this be? Consider this patient, her respiratory rate is 35 and yet her CO2 is climbing. Clearly her ventilation is ineffective. This information is important. It tells you that she has significant airflow obstruction such that a high respiratory rate is actually detrimental- she does not have enough time to expire fully. Paradoxically, a lower respiratory rate will actually be more effective at improving her minute ventilation by giving her time to fully expire.
I:E ratio= Inspiration time :expiration time ratio = time spent in inspiration : time spent in expiration. In a normal person this would be 1:2 or 1:3. For patients with obstructive lung pathology who require a prolonged expiratory time you’ll aim for I:E ratio of 1:4 or 1:5. This is adjusted by increasing inspiratory flow rate in volume control or Ti/Rise time in pressure control.
Initial settings:
- FiO2 100% then decreased to target sats 88-92%
- PEEP 5-10cmH2O
- I:E ratio 1:4 – 1:5
- Plateau <30 cmH2O driving pressure <15 cmH2O
- RR 12-15
- Follow VBG q1h and titrate accordingly. In COPD, ideally you want to have your PEEP set close to (but not exceeding) the patient’s own intrinsic or auto-PEEP in order to decrease the WOB. More on auto-PEEP below.
Breath stacking/Auto-PEEP
- Picture the patient above. You intubated them and put them on the settings listed. You go to see the next patient feeling victorious. You get called back an hour later by RN in a panic. Patient is now sating 80% on 100% Fio2, HR 140 sinus, BP 70/50, and pressure alarms are reading peak pressures >70. Norepi is now at 1.0mcg/kg/min.
- What is breath stacking?:
- In patients with airflow obstruction, a situation can develop such that there is not sufficient time to expire fully the air in the lung before another breath is taken in. This means that when the next breath is delivered the lung still has part of the previous tidal volume in it. This process continues and with each breath, more and more air accumulates in the lung resulting in over-distention and decreased CO2 clearance. As a result of this intrathoracic pressures can rise dramatically leading to decreased RV preload and can even lead to RA compression à massive hemodynamic collapse. Breathing stacking occurs on a ventilator but can also occur in an awake non-ventilated patient due to tachypnea in the setting of airflow obstruction.
- How to detect breath stacking:
- You can look on your ventilator!
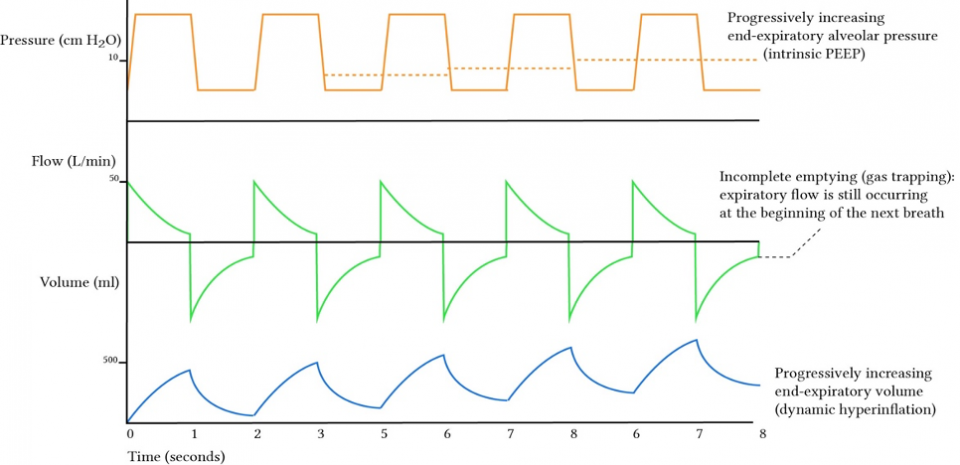
From Deranged Physiology
- The easiest visual way (IMO) is to look at the middle graph which is your flow curve. Above the x-axis is the inspiratory flow and below is the expiratory flow curve. In normal physiology, the green line on the expiratory flow cure should always return to the x-axis. This represents that flow has ceased i.e the pressure between the lung and the ventilator are equal, meaning air has been fully expired.
- If you notice the expiratory flow curve is not returning to the x-axis this means that the patient has not fully expired by the time the next breath is given. You can also see sequential volume increase at end-expiration (lower blue graph) or gradually increasing end-expiratory pressure (orange graph)
- You can also perform an end-expiratory hold maneuver– which is where you pause flow briefly at the end of expiration and measure the total pressure.
- This pressure is the TOTAL PEEP = Auto-PEEP + applied PEEP. Since you know the applied PEEP you set on your ventilator, this is subtracted from the total PEEP to give you the numeric value of the patient’s own auto-PEEP. On your vent there will be a button for “exp hold” to perform this maneuver.
How to manage auto-PEEP
- Drop the respiratory rate- more time is needed to expire! higher respiratory rates will limit the amount of exhalation time
- Increase I:E ratio
- Decrease Tidal volume- less volume delivered means less air can be trapped
- Sedate and paralyze the patient
- If all else fails- disconnect from the ventilator and manually bag with 100%FiO2 with LOW RR.
…And this brings us to Asthma
- Nothing scares an acute care physician and RT more than asthma. As a disclaimer, these patients are incredibly challenging to manage on a mechanical ventilator and always require an experienced multidisciplinary team. If you’re ever in a situation where you think you might have to intubate an asthmatic call for help very early, no one will fault you for that.
- Asthmatics are prone to severe auto-PEEP (way more so than COPDers) and tend to run into more issues with barotrauma and hemodynamic collapse. Ventilation of these patients is nuanced and individualized
- In general when ventilating an asthma:
- LOWEST PEEP possible. 0-5 (max). ZEEP (zero PEEP) has been proposed to avoid adding any additional pressure to the lung to avoid barotrauma
- High I:E ratio – 1:4 – 1:5 or more
- LOW RR 10-12 or LOWER. These patients need a very long expiratory time
- ACCEPT hypercapnia. Asthmatics can tolerate this well on a ventilator and as long as the pH can be controlled (>/= 7.2) accept really any level of CO2. You are trying to buy time for bronchodilators steroids and other therapy to work and reduce severe airflow obstruction.
- Accept high peak pressures. Ppeak will be very high in the asthmatic due to airway resistance. You will have to accept that but monitor closely the Pplat and driving pressure.
- Target saturation 88-94%
- Tidal volume 4-8mL/kg IBW
Obviously, this is not an inclusive guide, and as discussed before the management of the ventilated patient is full of nuance! But hopefully, this helps give you a starting guide that you can apply at the bedside!

THIS WAS SO GREAT