
The North American opioid crisis is rapidly expanding, resulting in unprecedented levels of harm and strain on the healthcare system. The opioid epidemic is not new to ED providers across the country, but the true extent of harm is quite shocking.
In Canada, there has been 40,642 apparent opioid toxicity deaths and 39,435 opioid-related hospitalizations between January 2016 and June 2023, equating to an average of 22 deaths and 17 hospitalizations each day in Canada. [3] Ontario alone witnesses an average of 7 opioid-related deaths a day. [37] The COVID-19 pandemic exacerbated this crisis, with Canada experiencing a 91% increase in opioid overdose deaths in the first 2 years of the pandemic. While these numbers are already quite concerning, they only capture deaths directly attributed to overdose, omitting the ones from secondary harm caused by soft tissue infections, endocarditis, and physical injury.
A major factor contributing to the crisis is the ever-shifting and increasingly toxic multi-drug supply. North America has borne witness to four overlapping “waves” of opioid supply shifts: the widespread proliferation of prescription opioids, followed by heroin’s rising dominance; then the emergence of illicitly manufactured fentanyl (IMF); and, most recently, a polysubstance crisis ushering in new generations of highly potent synthetic adulterants.

Over the past couple years, xylazine, popularly referred to as “tranq”; has made its way into the illicit opioid drug supply of North America, amplifying the already devastating opioid overdose crisis. There has been a recent surge in attention and concern about xylazine in the media in Canada and the United States, highlighting the urgent need for awareness and action.
Fentanyl mixed with xylazine is known by the street names of “sleep-cut”, “zombie drug”, and “tranq dope” and poses significant risks and challenges to public health and safety.
In this post, we will explore the origins and properties of xylazine, its prevalence in the illicit drug supply, the signs and symptoms associated with xylazine toxicity, the pathophysiology and mechanism of action, management strategies for “tranq dope” overdoses, xylazine-associated wounds and finally, discuss considerations for risk reduction and prevention.

[38] Ontario Drug Policy Research Network. (2024, January). Opioid Mortality Summary 2023 Q3 [PDF]. Retrieved from https://odprn.ca/wp-content/uploads/2024/02/OCC_Opioid-Mortality-Summary-2023_Q3-January-2024.pdf
Origins and Properties of Xylazine
Xylazine, is an alpha-2 agonist that was discovered and developed in 1962 by Bayer in Germany. It was initially explored for its potential as an antihypertensive medication. However, due to significant adverse effects, including hypotension, bradycardia, and CNS depression, xylazine failed to gain approval from the FDA for human use. Instead, in the early 1970s, it received FDA approval exclusively for veterinary medicine applications.
In this field, xylazine is widely used in the treatment of animals in veterinary medicine. It acts as a potent sedative with analgesic and muscle relaxant properties to facilitate various procedures.
Xylazine is available in liquid form and sold under the brand names of Rompun®, Anased®, XylaMed, and more directly through pharmaceutical distributors catering to veterinarians. However, it is also available for purchase at low prices on other internet sites in liquid and powder form, often with no association to the veterinary profession nor requirements to prove legitimate need. Despite not being FDA approved, to this day, xylazine remains unregulated under both the Controlled Substances Act (CSA) in the USA and the Controlled Drugs and Substances Act (CDSA) in Canada.
Given its availability, low price, and psychoactive effects, xylazine is being used as an adulterant and cutting agent in street drugs like fentanyl to increase bulk, enhancing profit for traffickers. Some customers intentionally seek out fentanyl mixed with xylazine for longer-lasting effects than fentanyl alone, while many are completely unaware that it’s being cut into their supply. Thus, xylazine or xylazine-containing drugs are being injected, ingested, and smoked.
Prevalence of Xylazine in the Ilicit Drug Market
Its emergence in the illicit drug market was first noted in Puerto Rico in the early 2000s, later spreading to the US and Canada.
It appeared in the US during the mid-2010s, notably in Philadelphia, which is widely recognized as the epicenter of the current crisis. Its prevalence increased throughout the 2020s, spreading and wreaking havoc to the rest of the country soon after. In the most recent data, more than 90% of unregulated fentanyl samples in Philadelphia contain xylazine, making it the most common adulterant in the drug supply there. Today, the DEA reports that they have seized xylazine and fentanyl mixtures in 48 of the 50 states.
Many recently published studies indicate that xylazine has been increasingly implicated and found in illicit drug-related deaths across the US and often in combination with fentanyl. Xylazine presents a significant challenge to both the US healthcare system and its users, due to the limited information available on the drug and the absence of an approved antidote.
Recognizing its escalating role in overdose deaths nationwide and its inherent challenges, the White House Office of National Drug Control declared, in April 2023, the combination of fentanyl and xylazine as an emerging threat to the USA, marking the first such designation in U.S. history. [4] This prompted the release of a National Response Plan, in July 2023, to address the emerging threat of fentanyl mixed with xylazine.
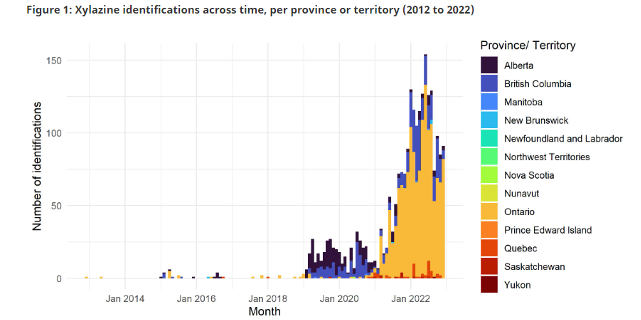
Xylazine began to proliferate in Canada around 2019, its prevalence is generally low, but has since increased in drug samples submitted to the Drug Analysis Service (DAS). In 2020, only 198 samples from six provinces contained Xylazine, the majority from B.C. and Alberta. By 2022, over 2,300 samples from eight provinces and one territory tested positive for Xylazine, marking an increase of more than 1000% over three years. With time, prominence has shifted from west to east, and is now greatest in Ontario.
The emergence of Xylazine in Canada.” Accessed: Feb. 03, 2024. [Online]. Available: https://www.canada.ca/en/health-canada/services/publications/healthy-living/emergence-xylazine-canada.html
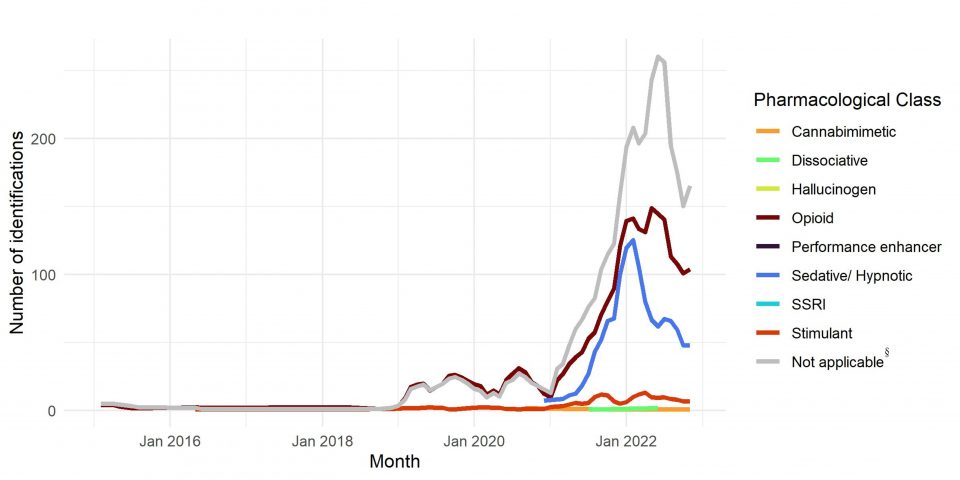
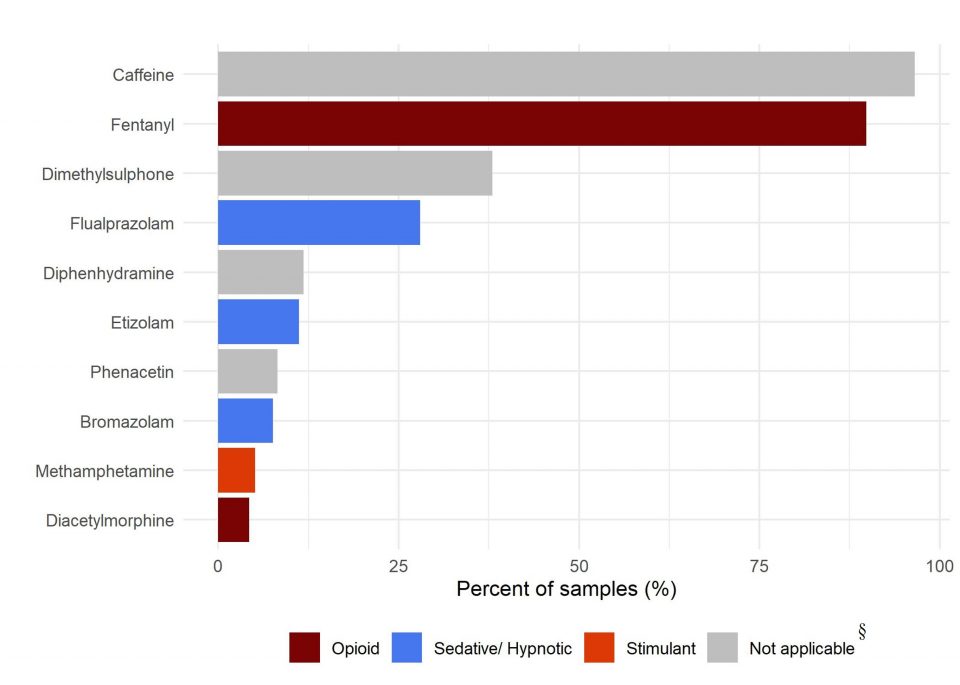
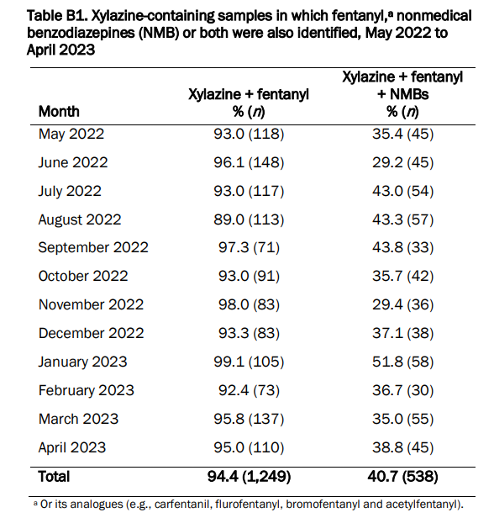
Xylazine is rarely identified alone and commonly appears alongside opioids, nonmedical benzodiazepines, or both, with fentanyl being the most common opioid and flualprazolam, bromazolam, or etizolam being the most common nonmedical benzodiazepines. In Canada, between May 2022 and April 2023, up to 99% of xylazine-containing samples also contained fentanyl, while up to 52% contained both fentanyl and benzos. Finally, from the latest data in Canada, the proportion of fentanyl samples that also contained xylazine is now around 9%, which is still a significant number.
“The emergence of Xylazine in Canada.” Accessed: Feb. 03, 2024. [Online]. Available: https://www.canada.ca/en/health-canada/services/publications/healthy-living/emergence-xylazine-canada.html
“The emergence of Xylazine in Canada.” Accessed: Feb. 03, 2024. [Online]. Available: https://www.canada.ca/en/health-canada/services/publications/healthy-living/emergence-xylazine-canada.html
“The emergence of Xylazine in Canada.” Accessed: Feb. 03, 2024. [Online]. Available: https://www.canada.ca/en/health-canada/services/publications/healthy-living/emergence-xylazine-canada.html
Toronto
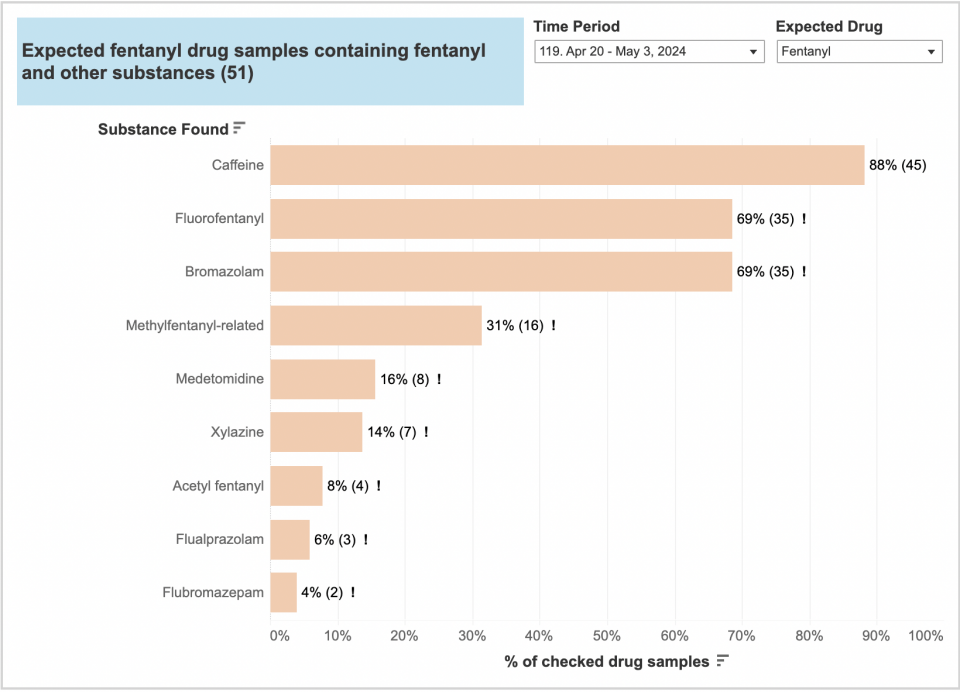
When looking at the data provided by Toronto’s drug checking supply between December 30th, 2023 and February 23rd, 2024 for expected fentanyl drug samples; 16% was found to contain xylazine, 14% contained dexmedetomidine and 43% contained bromazolam.
This simply highlights how there is a wide variety of adulterants in the opioid drug supply, which implies significant risk to public health and safety, as well as challenges when it comes to the management of overdoses. While this isn’t specific data from Ottawa’s drug supply, it is a good representation of how contaminated the opioid drug supply is in Ontario.
Expected fentanyl drug samples containing other substances from December 30, 2023 to February 23, 2024:
“Graphs,” Toronto’s Drug Checking Service. Accessed: May. 16, 2024. [Online]. Available: https://drugchecking.community/
Limitations:
While this data is valuable, there are limitations.
Our primary source of data on illegal drugs in Canada is the Drug Analysis Service (DAS). Unfortunately, the samples analyzed may not fully represent what’s actually circulating on the market, as certain substances may not be reported if they aren’t controlled under the Controlled Drugs and Substances Act. As xylazine is not a controlled substance, its testing and reporting in enforcement-submitted samples is not systematic nor complete, and thus subject to underreporting. This lack of data makes it challenging to assess the true extent of the illicit opioid market and predict future trends accurately. [5]
Signs and Symptoms of Xylazine Toxicity
Unfortunately, there is limited knowledge on xylazine toxicity in humans, so our data primarily stems from case reports and case series in the literature. Systematic reviews, such as Ruiz-Colon et al.’s and Ball et al.’s, shed light on this, identifying 43 and 98 cases of xylazine intoxication respectively, spanning several decades and countries. These reviews highlighted that the most common types of exposure were either unintentional or intentional misuse and abuse as an adulterant.
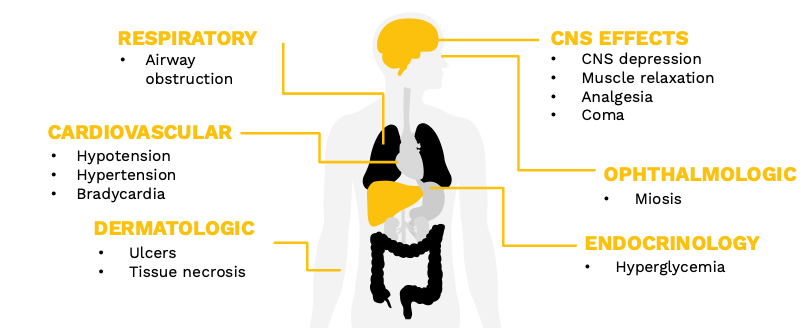
In the literature, acute xylazine intoxication is described to cause the following symptoms:
- CNS depression
- Muscle relaxation
- Analgesia
- Coma
- Airway obstruction or respiratory depression
- Bradycardia
- Hypotension
- Hypertension
- Hyperglycemia
- Miosis
Finally, skin ulcers and tissue necrosis are described in chronic xylazine use. [8] [9] [10]
Unfortunately, due to its use as an adulterant to opioids and the dynamic nature of the contaminated illicit drug supply, various substances with distinct toxidromes may coexist, and identifying xylazine toxicity can become quite challenging. However, what makes xylazine unique is that it causes a much more pronounced CNS depression leading to prolonged sedation and notable cardiovascular effects, which wouldn’t be expected in simple opioid or benzodiazepine overdoses.
Pathophysiology and Mechanism of Action of Xylazine
Normal Physiology:
The noradrenergic system has various functions throughout the central and peripheral nervous systems. One of its major roles is the “fight or flight” response. In the central nervous system, it also classically operates in promoting wakefulness and arousal.
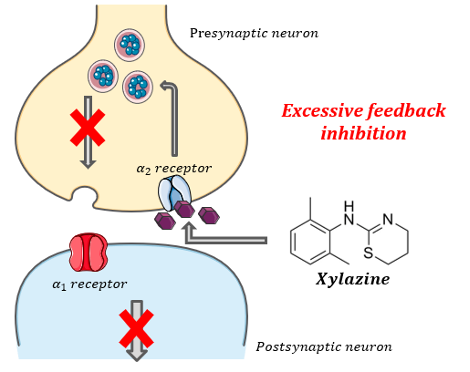
In simplified normal physiology of the central nervous system, norepinephrine is released from the presynaptic neuron and acts on alpha-1 receptors located on postsynaptic neurons regulating alertness, blood pressure, and heart rate. In situations where there is too much catecholamine in the synapse and increased sympathetic effect, norepinephrine binds to alpha-2 receptors on the presynaptic neurons creating a negative feedback mechanism to inhibit its release. This helps maintain homeostasis within the CNS and regulate sympathetic effect.
There are 3 alpha-2 receptor subtypes throughout the central and peripheral nervous system: alpha-2a, -2b, -2c. The activation of central presynaptic alpha-2a and 2c subtypes mediate the effects of sedation and analgesia. While the alpha-2b subtype, mainly located in vascular smooth muscles, mediates vasoconstriction and hypertension. Finally, there are also alpha 2a receptors in the pancreas that mediate glucose control.
Xylazine pharmacology and mechanism of action:
Xylazine is an α2-receptor agonist in the same drug class as clonidine and dexmedetomidine. It is structurally similar to these drugs and shares some of their clinical effects. While the pharmacology of xylazine is well-established in animal species, human studies are scarce and its mechanism is not well understood.
The proposed mechanism is that xylazine has a high affinity to central presynaptic alpha-2 receptors, causing excessive feedback inhibition of norepinephrine, which leads to profound CNS depression, analgesia, muscle relaxation and cardiovascular effects of hypotension and bradycardia.
Alone, xylazine is not believed to affect the respiratory rate like opioids do, but the profound CNS depression and muscle relaxation that it does cause can result in airway obstruction and blunted hypoxic reflex.
Like a clonidine overdose, it’s also believed to act on peripheral vascular alpha 2b-receptors which can cause transient hypertension. The hypotension that can sometimes follow is due to the centrally mediated effects. Finally, activation of alpha 2a receptors in the pancreas inhibiting insulin release is thought to be the mechanism responsible for hyperglycemia seen in some intoxication cases.
Xylazine is an ɑ2–receptor agonist causing inhibition of central noradrenergic system:
As xylazine is nearly always found in the presence of fentanyl and sometimes nonmedical benzodiazepines, further research is needed to determine the correlation between vital sign changes and clinical effects specifically for “tranq dope”. The combination of opioids and xylazine likely potentiates life-threatening CNS and respiratory depression, as their effects may be overlapping or synergistic. However, the exact mechanism of xylazine in these cases is unclear and remains elusive. [11] [12]
Pharmacokinetics:
The pharmacokinetics of xylazine in humans has not yet been determined. While it is well-established in veterinary medicine, extrapolating these findings directly to humans is challenging. Animal studies and case reports suggest that parenteral xylazine onset is typically within 30 minutes. Although the effects in animals typically last around 4 hours, human case reports document durations to be more than 8 hours, and in some cases as long as 72 hours.
Management of Suspected Tranq Dope Overdoses
Given the constant evolution and increasingly complex illicit drug supply, we are never going to be 100% sure of what we are dealing with in the emergency department.
However, when overdose presentations are not in keeping with typical opioid use and present with prolonged CNS depression, poor or partial response to naloxone, bradycardia, and hypo or hypertension, xylazine should be added to our differential diagnosis, along with other alpha-2 agonists like dexmedetomidine that share similar effects, and are now also contaminants surfacing in the illicit opioid drug supply in Ontario.
At this time, there are no standardized treatment algorithms recommended in the literature for xylazine exposure, and further research is needed to improve the care for these patients. As of June 2023, there are no specific antidotes for xylazine intoxication approved by the FDA. Reversal agents used in animals, such as tolazoline and atipamezole, have not been studied in humans for this purpose.
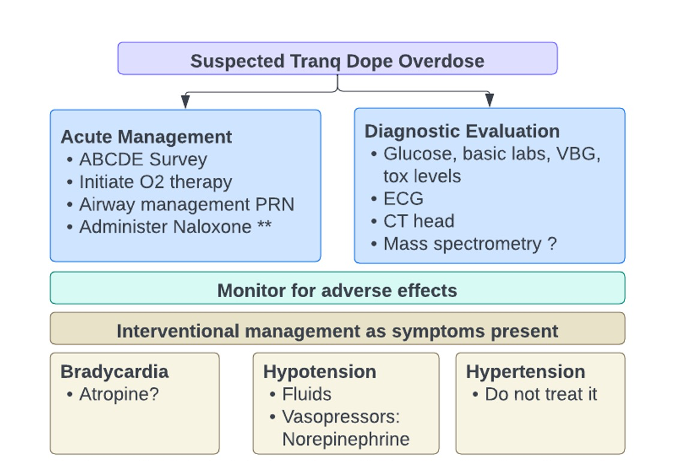
In the acute setting, the approach to the management of suspected tranq overdose involves providing the best supportive care possible, monitoring for adverse effects, and interventional management as symptoms present. Evaluating this patient is similar to any other intoxication. The initial priority is establishing and maintaining an airway and ensuring adequate breathing and circulation.
In light of the contaminated drug supply, our workup should remain broad and include a glucose, basic laboratories, osmols, VBG, tox levels, and an ECG. Alternative causes of the presentation that may require additional investigations or more advanced imaging, should also remain on differential diagnosis.
Most current testing available for Xylazine detection, such as advanced urine assays or serum levels, would not provide real-time assistance with the care of an intoxicated patient in the ED and is not a priority.
Naloxone:
Since xylazine is usually found with fentanyl in the illicit drug supply, naloxone should absolutely be given to treat any coexisting opioid toxidrome even if it is not expected to reverse the specific effect of xylazine such as the prolonged sedation. It is often stated that “naloxone is ineffective in xylazine intoxication” which propagates misinformation that it shouldn’t be used in patients with suspected Tranq Dope overdose. However, some of the life-threatening effects are related to the fentanyl, and adequate reversal of the opioid-induced respiratory effects remains a priority in the management.
The goal of naloxone administration is not a normal level of consciousness, but adequate ventilation. In the absence of signs of opioid withdrawal, there is no maximum safe dose. Providers should use the lowest effective dose reversing respiratory depression to avoid precipitating withdrawal in patients with opioid dependence, while titrating upward every few minutes until a desirable respiratory rate (RR >12) or sats (>90%) are achieved. [9] There are no guidelines in the literature on dosing and it remains a judgment call by the treating physician tailored to the patient. However, if a clinical effect does not occur after 10 mg, the diagnosis should be reconsidered
When it comes to the CNS depression aspect of the toxidrome, high-dose naloxone use to reverse the profound sedation caused by xylazine is theoretically plausible given its similar structure and mechanism of action to clonidine but, unfortunately, its efficacy has not been studied. [9] It’s also rare to see an isolated xylazine overdose, since it is commonly found in combinations with opioids, nonmedical benzodiazepines, or both, which plays a role in the sedation and wouldn’t respond to naloxone for this purpose. Additionally, precipitating an opioid withdrawal is also a concern.
Airway and Breathing:
Since patients with “tranq dope” (xylazine-fentanyl) overdose can present with significant sedation and respiratory depression, supportive airway management and monitoring is important. Clinicians should be prepared to intubate if the patient can’t protect their airway or respiratory depression isn’t reversed by naloxone.
Hypertension
When it comes to hemodynamic instability, hypertension is typically of short duration and is often followed by hypotension. This means that, in most patients, hypertension treatment is unnecessary and may be harmful. [35]
Hypotension
Within the existing literature, hypotensive patients from xylazine exposure usually responded well to IV fluids and the use of pressors was less frequent. [9] [8] However, if hypotension persists despite appropriate fluid resuscitation, vasopressors may be needed. Norepinephrine should be the preferred first-line agent given xylazine’s mechanism of action in the central nervous system.
Bradycardia
In xylazine toxicity, bradycardia is a common symptom and typically will not respond to atropine as evident in the literature due to its mechanism of action. [9] [11] However, when consulting toxicology experts, Dr. Margeret Thompson (the medical director of Ontario Poison Centre) and Dr. Alexandra Hamlin (Toxicology fellow in Calgary), they both stated that they would still trial atropine if faced with an unstable bradycardic patient despite the variable evidence since there is little adverse effects associated with this drug.
Xylazine-associated Wounds
Although abscesses and wound development have been a common complication of injection drug use for decades, xylazine-associated wounds seem to represent a unique clinical entity. The first published literature of this issue is from Puerto Rico in the early 2010s and at that time, researchers found that people using xylazine had a higher prevalence of skin ulcers compared to those who did not use it (38.5% vs. 7%). [14]

[15] R. Ehrman-Dupre, C. Kaigh, M. Salzman, R. Haroz, L.-K. Peterson, and R. Schmidt, “Management of Xylazine Withdrawal in a Hospitalized Patient: A Case Report,” J. Addict. Med., vol. 16, no. 5, p. 595, Oct. 2022, doi: 10.1097/ADM.0000000000000955.
There has since been an increase in case reports of skin manifestations and infections related to xylazine use documented in the literature. In these case studies, the patients reported limited cutaneous complications until the recent addition of a new substance, “tranq dope”, to their drug supply.
Pathophysiology:
The proposed mechanism is thought to be mediated by the direct vasoconstrictive effect of xylazine activating peripheral alpha-2b receptors in the vascular smooth muscles. In addition to vasoconstriction, central effects of xylazine leading to hypotension and bradycardia results in lower tissue oxygenation. Thus, chronic use of xylazine can lead to decreased perfusion, impaired wound healing, necrosis, and a higher chance of severe soft tissue infections.
However, the true pathophysiology of these wounds remains unclear and is likely multifactorial. In addition to this proposed mechanism, there have been multiple other postulated causes including the direct cytotoxic effect of the drug, the hyperglycemic effects, increased frequency of injection or use, and tissue compression during periods of prolonged sedation. Finally, these wounds occur in people who use drugs, many of whom experience a lack of housing, chaotic lifestyles, and limited access to medical care, which can worsen their prognoses.
Clinical Presentation:
A diagnosis of xylazine-associated wounds is largely based on clinical suspicion. They are unique and distinct from typical injection-related skin and soft tissue wounds for two key reasons:
- They are reported to develop not only at injection sites but also in areas distant and irrespective of them. They are even reported in patients who use but do not inject the drug.
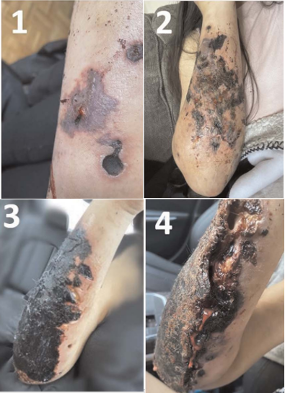
- They have a unique appearance and progression. These wounds are most commonly noted on the posterior forearms or lower legs and are described as jagged, angulated ulcers often with areas of eschar and necrosis formation.
- They usually appear as small round dark purple lesions with irregular borders and intact skin, and often progress to merge. They then harden into a dry adherent eschar and necrotic tissue. They can progress into deep ulcers reaching full thickness and expose tendons and bone. [16]
R. McFadden et al., “Xylazine-associated Wounds: Clinical Experience From a Low-barrier Wound Care Clinic in Philadelphia,” J. Addict. Med., vol. 18, no. 1, p. 9, Feb. 2024, doi: 10.1097/ADM.0000000000001245.
While these wounds generally lack classic signs of infection and are more necrotic in nature, some can progress, leading to extensive necrosis and secondary infections including cellulitis, deep space infection, osteomyelitis and sepsis.
Treatment:
Although there is a lack of data-driven recommendations or standardized approaches, from collective clinical experience published in the literature, treatment should follow basic wound care with wound cleansing and use of nonadherent gauze for the wound bed. Daily dressing changes with layered dressings are optimum. Keeping the wound moist, clean, and covered at all times is imperative to help prevent infection.
The wounds should also be evaluated for potential secondary infection. Antibiotic selection for secondary infection should cover MRSA and GAS coverage may need to be considered depending on the extent of the wound and clinical status of the patient.
In cases of advanced wounds with severe necrosis, significant infections, or sepsis, as seen in the case reports in the literature, advanced therapies with IV antibiotics, surgical debridement, surgical reconstruction, or amputation may be required. 11-12] [15] [17-20]
Risk Reduction and Prevention
In the emergency department, our responsibility in risk reduction and harm prevention is crucial, particularly in light of the ongoing opioid crisis exacerbated by potent adulterants like xylazine, which pose a significant threat to public health and safety.
Following discussions about xylazine infiltration in the illicit opioid drug supply in Canada with Dr. Lisa Bromley, the medical director of the substance use program at the Ottawa Hospital, here is the key insight and expert opinion she wished to share:
“Opioid Agonist Treatment is highly protective against opioid-related overdose death, whether the opioids used contain xylazine or not. The ED can play a huge role in improving access and rapid induction on to life-saving OAT for patients.”
While managing patients with opioid use disorder may become more complex with the presence of xylazine, it’s important to acknowledge the stark reality that studies have repeatedly shown that the one-year mortality rate in patients who present to the emergency department surviving an opioid overdose is as high as 5%. In these individuals, initiation of opioid agonist therapy is associated with decreased all-cause and opioid-related mortality compared with no medication treatment. Despite the overwhelming evidence on life-saving interventions for opioid use disorder, prescribing rates from ED remain frighteningly low.
Dr. Max Zworth, PGY4 Emergency Medicine in Ottawa, delivered an excellent grand-rounds presentation last year on OAT, bringing forward these issues, emphasizing that we can safely and easily initiate treatment in the emergency department. In his post, he provides a simple, easy-to-follow algorithm for prescribing this potentially life-saving medication to patient in your ED, particularly suboxone, which is considered the first line treatment for opioid use disorder. “Tranq dope” overdoses are still fentanyl overdoses and patient could potentially benefit from initiation of OAT. Generally, patients presenting to ED after a “tranq dope” overdose would fall under the suboxone macro dosing pathway of the algorithm.
Finally, the following recommendations should be considered to improve counselling from ED after overdose visits:
- Provide naloxone kits on discharge
- Refer patients to supervised consumption sites for supplies, overdose prevention and drug checking, in Ottawa specifically:
- The Trailer at Shepherds of Good Hope: 230 Murray Street, Hours: 7 days a week, 24 hours a day
- Sandy Hill Community Health Centre: 221 Nelson Street, Hours: Monday to Friday, 8am to 6pm (last call at 5pm)
- Somerset West Community Health Centre: 55 Eccles Street, Hours: 7 days a week, 9am to 4pm
- Ottawa Public Health: 179 Clarence Street, Hours: Monday to Friday, 9am to 5pm
- Counsel patients who inject drugs on safer injection techniques (counsel patients who inject drugs on safer injection techniques).
- Counsel patients on the signs and symptoms of local and systemic infection since they can often be confused with dope sickness/withdrawal.
Conclusions
- “Tranq dope” is an emerging public health threat in Canada:
- Xylazine mixed with fentanyl (tranq dope) is a critical and emerging public health concern in Canada
- It is associated with the following symptoms:
- Severe central nervous system and respiratory depression
- Significant cardiovascular effects
- Potentially disfiguring and life-threatening wounds
- The literature is limited
- Despite all the attention that it has been getting in the media, the literature is limited.
- More research is needed to help us better understand xylazine’s effect and care for patients exposed to it.
- Management of suspected tranq dope overdose:
- There are no clear guidelines and treatment resolves around supportive care and symptom management.
- Naloxone should absolutely be given to reverse coexisting opioid toxidrome.
- Atropine may be considered for unstable bradycardia.
- Consider initiating OAT from the ED after opioid overdose visits, regardless of contaminants like xylazine.
As emergency medicine physicians, we are in the position to join the battle and help blunt the curve of the increasingly complex opioid crisis.
Refernces
[1] J. Hoffman, “Tranq Dope: Animal Sedative Mixed With Fentanyl Brings Fresh Horror to U.S. Drug Zones,” The New York Times, Jan. 07, 2023. Accessed: Feb. 03, 2024. [Online]. Available: https://www.nytimes.com/2023/01/07/health/fentanyl-xylazine-drug.html
[2] wikifry, “This dog is a cow-magnet,” r/pics. Accessed: Mar. 29, 2024. [Online]. Available: www.reddit.com/r/pics/comments/2vkkgw/this_dog_is_a_cowmagnet/
[3] “Opioid- and stimulant-related harms — Canada.ca.” Accessed: Feb. 25, 2024. [Online]. Available: https://health-infobase.canada.ca/substance-related-harms/opioids-stimulants/
[4] J. Hoffman, “White House Designates Animal Sedative as an ‘Emerging Drug Threat,’” The New York Times, Apr. 12, 2023. Accessed: Feb. 03, 2024. [Online]. Available: https://www.nytimes.com/2023/04/12/health/tranq-dope-xylazine.html
[5] “The emergence of Xylazine in Canada.” Accessed: Feb. 03, 2024. [Online]. Available: https://www.canada.ca/en/health-canada/services/publications/healthy-living/emergence-xylazine-canada.html
[6] Canadian Centre on Substance Use and Addiction (CCSA). (2022, July). “CCSA-CCENDU Drug Alert: Xylazine.” [Online]. Available: https://www.ccsa.ca/sites/default/files/2022-07/CCSA-CCENDU-Drug-Alert-Xylazine-2022-en.pdf. Accessed: March 17, 2024
[7] “Graphs,” Toronto’s Drug Checking Service. Accessed: Mar. 08, 2024. [Online]. Available: https://drugchecking.community/
[8] “Opioid overdoses involving xylazine in emergency department patients: a multicenter study.” Accessed: Feb. 16, 2024. [Online]. Available: https://www.tandfonline.com/doi/epdf/10.1080/15563650.2022.2159427?needAccess=true
[9] “Xylazine poisoning: a systematic review.” Accessed: Feb. 16, 2024. [Online]. Available: https://www.tandfonline.com/doi/epdf/10.1080/15563650.2022.2063135?needAccess=true
[10] K. Ruiz-Colón, C. Chavez-Arias, J. E. Díaz-Alcalá, and M. A. Martínez, “Xylazine intoxication in humans and its importance as an emerging adulterant in abused drugs: A comprehensive review of the literature,” Forensic Sci. Int., vol. 240, pp. 1–8, Jul. 2014, doi: 10.1016/j.forsciint.2014.03.015.
[11] J. D’Orazio, L. Nelson, J. Perrone, R. Wightman, and R. Haroz, “Xylazine Adulteration of the Heroin–Fentanyl Drug Supply,” Ann. Intern. Med., vol. 176, no. 10, pp. 1370–1376, Oct. 2023, doi: 10.7326/M23-2001.
[12] B. N. Papudesi, S. V. Malayala, and A. C. Regina, “Xylazine Toxicity,” in StatPearls, Treasure Island (FL): StatPearls Publishing, 2024. Accessed: Mar. 05, 2024. [Online]. Available: http://www.ncbi.nlm.nih.gov/books/NBK594271/
[13] S. Ayub et al., “Xylazine in the Opioid Epidemic: A Systematic Review of Case Reports and Clinical Implications,” Cureus, Mar. 2023, doi: 10.7759/cureus.36864.
[14] J. C. Reyes et al., “The Emerging of Xylazine as a New Drug of Abuse and its Health Consequences among Drug Users in Puerto Rico,” J. Urban Health Bull. N. Y. Acad. Med., vol. 89, no. 3, pp. 519–526, Jun. 2012, doi: 10.1007/s11524-011-9662-6.
[15] R. Ehrman-Dupre, C. Kaigh, M. Salzman, R. Haroz, L.-K. Peterson, and R. Schmidt, “Management of Xylazine Withdrawal in a Hospitalized Patient: A Case Report,” J. Addict. Med., vol. 16, no. 5, p. 595, Oct. 2022, doi: 10.1097/ADM.0000000000000955.
[16] R. McFadden et al., “Xylazine-associated Wounds: Clinical Experience From a Low-barrier Wound Care Clinic in Philadelphia,” J. Addict. Med., vol. 18, no. 1, p. 9, Feb. 2024, doi: 10.1097/ADM.0000000000001245.
[17] A. Dowton et al., “Recognition and Treatment of Wounds in Persons Using Xylazine: A Case Report From New Haven, Connecticut,” J. Addict. Med., vol. 17, no. 6, pp. 739–741, Dec. 2023, doi: 10.1097/ADM.0000000000001198.
[18] L. Wallace, “A Case Of Skin Necrosis Caused By Intravenous Xylazine Abuse,” J. Hosp. Med., Accessed: Feb. 24, 2024. [Online]. Available: https://shmabstracts.org/abstract/a-case-of-skin-necrosis-caused-by-intravenous-xylazine-abuse/
[19] “Xylazine Wound Care Guide by nextdistro – Issuu.” Accessed: Feb. 03, 2024. [Online]. Available: https://issuu.com/nextdistro/docs/xylazine_wound_care_pdf
[20] S. V. Malayala, B. N. Papudesi, R. Bobb, and A. Wimbush, “Xylazine-Induced Skin Ulcers in a Person Who Injects Drugs in Philadelphia, Pennsylvania, USA,” Cureus, vol. 14, no. 8, p. e28160, doi: 10.7759/cureus.28160.
[21] Canadian Centre on Substance Use and Addiction (CCSA). (2023, July). “CCENDU bulletin: Update on Xylazine in the unregulated drug supply.” [Online]. Available: https://www.ccsa.ca/sites/default/files/2023-07/CCENDU-bulletin-update-on-Xylazine-in-the-unregulated-drug-supply-en.pdf. Accessed: March 17, 2024.
[22] “Human Xylazine Overdose: A Comparative Review with Clonidine, Phenothiazines, and Tricyclic Antidepressants.” Accessed: Mar. 07, 2024. [Online]. Available: https://www.tandfonline.com/doi/epdf/10.3109/15563658108990293?needAccess=true
[23] R. Gupta, D. R. Holtgrave, and M. A. Ashburn, “Xylazine — Medical and Public Health Imperatives,” N. Engl. J. Med., vol. 388, no. 24, pp. 2209–2212, Jun. 2023, doi: 10.1056/NEJMp2303120.
[24] N. Chhabra et al., “Notes From the Field: Xylazine-Related Deaths – Cook County, Illinois, 2017-2021,” MMWR Morb. Mortal. Wkly. Rep., vol. 71, no. 13, pp. 503–504, Apr. 2022, doi: 10.15585/mmwr.mm7113a3.
[25] T. Hu et al., “Initiation of opioid agonist therapy after hospital visits for opioid poisonings in Ontario,” CMAJ, vol. 195, no. 49, pp. E1709–E1717, Dec. 2023, doi: 10.1503/cmaj.231014.
[26] S. L. Kacinko, A. L. A. Mohr, B. K. Logan, and E. J. Barbieri, “Xylazine: Pharmacology Review and Prevalence and Drug Combinations in Forensic Toxicology Casework,” J. Anal. Toxicol., vol. 46, no. 8, pp. 911–917, Oct. 2022, doi: 10.1093/jat/bkac049.
[27] K. L. Sue and K. Hawk, “Clinical considerations for the management of xylazine overdoses and xylazine-related wounds,” Addiction, vol. n/a, no. n/a, doi: 10.1111/add.16388.
[28] R. A. Torruella, “Xylazine (veterinary sedative) use in Puerto Rico,” Subst. Abuse Treat. Prev. Policy, vol. 6, no. 1, p. 7, Apr. 2011, doi: 10.1186/1747-597X-6-7.
[29] Drug Enforcement Administration (DEA). (2022, December). “The Growing Threat of Xylazine and its Mixture with Illicit Drugs.” [Online]. Available: https://www.dea.gov/sites/default/files/2022-12/The%20Growing%20Threat%20of%20Xylazine%20and%20its%20Mixture%20with%20Illicit%20Drugs.pdf Accessed: March 17, 2024.
[30] “Xylazine (Tranq): Here’s What You Need to Know About the New Street Drug Taking Over Philly,” Substance Use Philly. Accessed: Feb. 03, 2024. [Online]. Available: https://www.substanceusephilly.com/tranq
[31] New York State Department of Health, “Xylazine Use in New York State,” Albany, NY, USA, January 2022. Available: https://www.health.ny.gov/publications/12044.pdf
[32] M. Z. Seliga Rebecca, “Buprenorphine: A guide for ED providers,” EMOttawa Blog. Accessed: Mar. 04, 2024. [Online]. Available: https://emottawablog.com/2023/03/buprenorphine-a-guide-for-ed-providers/
[33] G. A. Recovery, “Drug Overdose Symptoms | Drug Addiction Treatment Georgia,” Georgia Addiction Treatment Center. Accessed: Mar. 29, 2024. [Online]. Available: https://georgiaaddictiontreatmentcenter.com/2020/06/25/drug-overdose-symptoms/
[34] UpToDate. (2024, Feb.). Acute opioid intoxication in adults. [Online]. Available: https://www.uptodate.com/contents/acute-opioid-intoxication-in-adults?sectionName=MANAGEMENT&search=xylazine%20overdose%20managemen&topicRef=6509&anchor=H13&source=see_link#H13. Accessed: March 17, 2024.
[35] UpToDate. (2024, Feb). Clonidine, xylazine, and related imidazoline poisoning. [Online]. Available: https://www.uptodate.com/contents/clonidine-xylazine-and-related-imidazoline-poisoning?search=clonidine%20intoxi&source=search_result&selectedTitle=1%7E150&usage_type=default&display_rank=1. Accessed: March 17, 2024.
[36] Goldfrank, L. R., Flomenbaum, N. E., Lewin, N. A., Nelson, L. S., & Howland, M. A. (2011). Goldfrank’s Toxicologic Emergencies. 9th ed. McGraw-Hill Education Medical.
[37] Marx, J. A., Walls, R. M., Hockberger, R. S., & Gausche-Hill, M. (2021). Rosen’s Emergency Medicine: Concepts and Clinical Practice. 10th ed. Elsevier.
[38] Ontario Drug Policy Research Network. (2024, January). Opioid Mortality Summary 2023 Q3 [PDF]. Retrieved from https://odprn.ca/wp-content/uploads/2024/02/OCC_Opioid-Mortality-Summary-2023_Q3-January-2024.pdf
[39] Ontario Drug Policy Research Network (ODPRN). (n.d.). OCC Opioid and Suspect Drug-Related Death Data. [Online]. Available: https://odprn.ca/occ-opioid-and-suspect-drug-related-death-data/. Accessed: March 17, 2024.
