
As Emergency Physicians, we are all experts in saving lives, yet we are often least prepared for the moment when a patient is imminently dying. The hardest decision isn’t starting resuscitation; it’s knowing when it is non-beneficial and ensuring the patient is comfortable in their final hours. However, not everyone is necessarily comfortable or knows what to do when the discussion changes from ‘how do we save this patient’ to ‘how can we ensure they die comfortably’.
By the end of this post, you should be able to:
- Understand the key role of ED physicians in delivering end-of-life (EOL) care
- Recognize the signs of an imminently dying patient
- Develop an approach to manage the imminently dying patient
- Apply evidence-based strategies for pain, dyspnea, agitation, and other end-of-life symptoms
- Implement system and team-based approaches to ensure high-quality, patient-centered end-of-life care in the ED
Why should we care about end-of-life care in the ED?
A recent retrospective review in the United States analyzed data from a national electronic health records database over a 10-year period involving more than 96 million ED encounters. The results were extrapolated to estimate that deaths occurring in EDs accounted for approximately 11% of all deaths nationwide, and 33% of all those who died visited the ED within 1 month of death (Elmer et al., 2022).
- While Canadian data does not exist, we can expect it would follow a similar pattern
- A Canadian study showed 42% of deaths across Canada occur in hospital, with 80% of these being preceded by ED admission (Wilson et al., 2024)
- By the year 2050, the population of Canadians over the age of 85 is expected to double, with an overall 25% increase in total deaths nationwide (Diaconu et al., 2016)
- As the population expands and ages, we will continue to encounter more patients in the ED presenting near or at the end of life
What do patients want at the end of life?
Many patients have already thought about how they hope to experience the dying process:
- data from the ACCEPT study showed only 12% of the 278 patients surveyed preferred life prolonging care over comfort care (Heyland et al, 2013)
- in the United States, 70% of adults >75 years old reported a preference for comfort care over resuscitative care if they were actively dying (Bernacki & Block, 2014)
- a 2022 report in the Lancet described the “medicalization of death,” in which death is viewed as a medical issue instead of a natural life process, resulting in:
- prolonged deaths, with futile medical interventions in the final days
- a feeling of fear, avoidance, and delayed recognition of the dying phase
Early Goals of Care Discussions
The best way to ensure we are respecting patients’ and their families’ wishes is to initiate early goals of care (GOC) discussions, especially in the critically ill patient or those we expect could deteriorate. While many patients have had prior discussions with family members and have already decided on their GOC, sometimes ED physicians are the first healthcare providers to bring up this topic.
- the ACCEPT study showed 76% of Canadians had thought about end-of-life care but only 55% had discussed their preferences with their healthcare team (Heyland et al., 2013)
- only 30% of patient charts accurately reflected the wishes of those preferring end-of-life care
These conversations can be challenging, especially the scenario in which a family or a SDM is requesting aggressive treatment measures despite our professional opinion that doing so would be futile. For comprehensive guides to conducting GOC conversations, please refer to prior Grand Rounds summaries by Dr. Lucy Karp and Dr. Michael Wong.
Palliative Care, End-of-Life, and Imminent Death
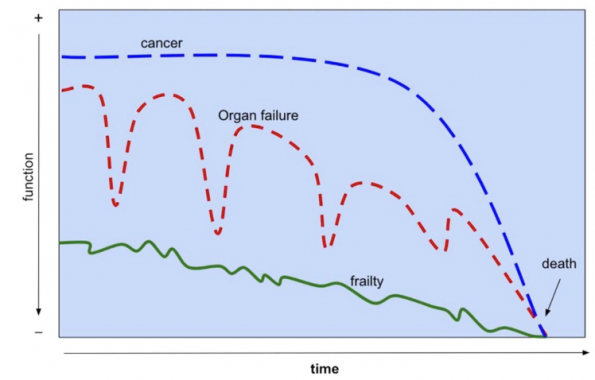
Adapted from Lunney JR, Lynn J, Foley DJ, et al. Patterns of Functional Decline at the End of Life. JAMA.2003;289(18):2387–2392.
Palliative care literature classically categorizes the dying process into different trajectories:
- a short period of rapid decline (often in the setting of advanced cancers)
- a slow decline of organ failure interspersed with episodes of severe exacerbation/illness
- a prolonged dwindling course of those with severe frailty or dementia
While the focus of this blog post is not on the role of palliative care in the ED, it is important to acknowledge that most of the guidance around end-of-life care in the ED is informed by the world of Palliative Medicine. For a detailed explanation of palliative care in the ED, please refer to part 1 and part 2 of palliative care in the ED.
For the purposes of this blog post, “imminently dying” will refer to patients in their final hours to days of life.
Signs of an Imminently Dying Patient
Predicting time until death can be fraught with uncertainty, even for the most experienced clinicians. Much of the research around clinical signs of imminent death and prognostication comes from palliative care literature.
A key study from Japan observed four main clinical signs in 100 terminally ill cancer patients admitted to a palliative care unit (Morita et al, 1998). The median time from onset to death was:
- Death rattle: 23 hours
- Respirations with mandibular movement: 2.5 hours
- Peripheral cyanosis: 1 hour
- Pulseless radial artery: 1 hour
Another study from 2014 identified 5 clinical signs with a high specificity and positive likelihood ratios for death within the next 72 hours (Hui et al., 2014):
- non palpable radial pulse
- mandibular/agonal respirations
- decreased urine output (<100mL/12hours)
- Cheyne-Stokes breathing
- death rattle
Note that these signs are highly specific, but not sensitive. This means that imminently dying patients will not necessarily display these signs; however, their presence can be highly informative. Additionally, most of this data comes from palliative care and oncology patient studies, and their prognostic accuracy has been less well validated in the ED. Nevertheless, these signs can help support our decision making and help us initiate urgent goals of care discussions and provide symptom-directed comfort measures.
“One of the most useful predictive tools is to get a sense of functional rate of change, ie. if someone has been declining over the past few weeks, you can assume the decline will likely continue (in the absence of a treatable reversible cause)”
– Dr. Lisa Fischer, Emergency and Palliative Care Physician
An Approach to Caring for the Imminently Dying Patient
In 2021, the American College of Emergency Physicians published set of national guidelines on the delivery of palliative care in the Emergency Department. The document covers all aspects of palliative care and includes a section on the medical management of refractory symptoms in this patient population. ACEP also a has a palliative care toolkit accessible on their website which includes instructions for ED physicians on screening patients who could benefit from early palliative care consultation, tips on how to hold concise but targeted goals of care discussions, and recommended medications/doses for end-of-life symptom management.
- Currently, there is no national Canadian ED-specific standard guideline on the management of imminently dying patients
- In 2020, a report was published in CJEM to address this gap in the literature (Hendin et al., 2020)
- There is also a recent expert review discussing this same topic, published in Clinics in Geriatric Medicine (Prachanukool et al., 2023)
The following section will discuss an approach to symptom management, drawing largely from the available literature with some input from local experts.
Step 1: Review medications
- Discontinue non-contributory medications
- Continue any medications that contribute to symptom management
Step 2: Treat current symptoms
- Ex: pain from a malignant wound or agitation from urinary retention
Step 3: Prepare to treat EOL symptoms
Pain
Subcutaneous analgesia is preferred over IV when possible as it has a longer half-life. For opioid-naive patients, a suggested approach is:
- Morphine 1-2mg SC/IV q30 mins PRN
OR
- Hydromorphone 0.2-0.4mg SC/IV q30 mins PRN
OR
- Fentanyl 12.5 – 50 mcg SC/IV q30 mins PRN
It is recommended to start with these doses but rapidly titrate the dose, frequency, or both as required. As the doses become large and frequent, some may start to feel uncomfortable or wonder if we are speeding up the dying process. That is not our goal, however sometimes this is an inevitable consequence of higher doses of analgesia required for effective symptom relief. This is the “double effect” doctrine, a common ethical dilemma encountered in the field of palliative medicine (Faris et al., 2021).
For patients already receiving opioid therapy, calculate their total daily (24 hour) dose and convert it to subcutaneous equivalents (see table below for conversions). The American College of Emergency Physicians (ACEP) recommends using 10-20% of the current total daily dose as a single dose for breakthrough pain (Loffredo et al., 2021). This can be titrated for refractory pain, increasing the dose by 50%, or increasing the frequency to every 15 minutes.
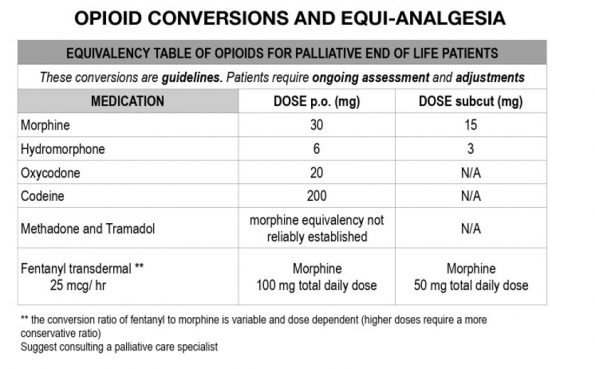
Table from Hendin et al., 2020
Dyspnea
Subjective difficulty breathing is common and one of the most distressing symptoms in the imminently dying patient. Dyspnea and a feeling of suffocation can lead to distress and anxiety, causing increased respiratory effort and oxygen consumption. Initial management includes:
- positioning the patient upright if possible
- discontinuing IV fluids
- use a fan or open window to increase air movement and reduce the sensation of dyspnea (Weissman, 2024). Cool air blowing on a person’s face reduces dyspnea by altering the brain’s perception of breathlessness (Schwartzstein et al., 1987)
Opioids are the pharmacologic treatment of choice for dyspnea.
- opioids relieve dyspnea by reducing the central perception of breathlessness
- opioids blunt the ventilatory response to rising hypercapnia and decrease excessive work of breathing (Hallenbeck, 2012)
- follow the same dosing strategy as outlined above for both opioid-naive patients and those on baseline opioid therapy
Should we provide supplemental oxygen?
- a 2010 multi-centre double-blind randomized control trial showed supplemental oxygen provided no additional symptomatic benefit over room air alone (Abernethy et al., 2010)
- it is reasonable to administer a therapeutic trial of oxygen up to 6L/min guided by symptom relief, not pulse oximetry readings
- Nasal cannula is preferred over a mask due to the risk of inducing or worsening agitation
Airway Secretions
Excessive secretions pooling in the airway cause the aforementioned “death rattle” that is observed in many patients at the very end of life. While this can be distressing for others in the room, we can educate family members that the sound is an indication that the patient’s muscles are relaxed, and the patient themselves is not likely to experience any distress (Hendin et al., 2020).
- Positioning the patient upright can help reduce this noise
- A 2023 systematic review and meta-analysis found no strong evidence to support the use of anticholinergic medications to treat the death rattle in dying patients (Taburee et al., 2023), however they are often commonly administered
- A suggested approach is glycopyrrolate 0.4mg SC/IV q4h PRN
Agitation/Delirium
Unless there is a very simple reversible cause of a patient’s agitation or delirium, at the very end of life the focus is on symptom control. Both the ACEP guidelines and Hendin et al. (2020) advise low dose subcutaneous haloperidol as first line treatment, titrated to effect. Second- or third-line agents may be necessary if haloperidol is ineffective, especially in scenarios where agitation or restlessness is directly contributing to patient discomfort. We should always keep in mind the goal of maximizing comfort and minimizing distress for loved ones in the room. A suggested approach is:
- Haloperidol 0.5mg – 1mg SC/IV q2h PRN
- If severe, add Methotrimeprazine (Nozinan) 12.5 – 25mg SC q4h PRN
- If severe, add Midazolam 0.5 – 1mg SC/IV q30 mins PRN
Nausea/Vomiting
Imminently dying patients may sometimes experience nausea and vomiting, attributed to factors such as gastrointestinal stasis, medication effects, metabolic derangements, or organ failure (Leach, 2019). A suggested approach is:
- Metoclopramide 5 – 10 mg SC/IV q4h PRN (C/I in complete bowel obstruction)
OR
- Haloperidol 0.5 – 1 mg SC/IV q4h PRN
Non-Pharmacologic Management
- Monitoring: discontinue cardiac monitoring, vitals, labs
- Mouth and Eye Care: hourly PRN moistening/drops for comfort
- To Feed or Not to Feed: oral nutrition can be continued if requested by the patient, so long as it does not place the patient at risk of additional complications
- Avoid feeding if the patient is drowsy or confused, to avoid aspiration risk
- Social Work: consider Social Work involvement to guide family members through the dying process
- Spiritual Care: as requested by patients/families
- Palliative Care: consider Palliative Care consultation if you are having difficulty with refractory symptom management at the end of life
- Environment: while our goal is to provide great end-of-life care for dying patients, the ED environment is often not conducive to this
- move the patient to a quieter area of the department, if possible, such as a room with closed doors for privacy
- dimming the lights and bringing in an extra chair or two for family members can be a nice touch
- Education: there is an opportunity here for ED physicians to educate family members as they will often have a lot of questions about what is considered “normal” at the end of life
- the ability to normalize a lot of the things they are seeing can help put them at ease
Step 4: Prepare for sudden emergencies
Apart from the symptoms discussed above, sudden emergencies can occur at the end of life, which can be quite distressing for both the patient and their family members.
- Seizures should be managed with benzodiazepines
- A common approach includes lorazepam 2 mg or midazolam 5 mg q5 mins PRN x 3 doses, both of which can be given IM or SC
- sudden catastrophic bleed or airway obstruction may occur in patients at high risk, such as those with mediastinal tumors, head/neck tumors, or fistulating pelvic tumors (Nauck et al., 2008)
- optimize patient comfort using a dissociative agent such as ketamine dosed at 4mg/kg IM or 1mg/kg IV
- have medications drawn up beforehand to ensure the team can intervene immediately
- keep dark towels in the room to reduce distress at the sight of blood
- these cases require clear communication with the patient and family members in advance
Step 5: Disposition planning
Even if death appears imminent and comfort measures are ordered, don’t forget about disposition planning.
- Consider arranging admission early so that the patient can be moved to a ward bed as soon as possible
- These patients are often prioritized for admission to provide patients and their families with a more suitable environment for end-of-life care
Systems-Level Strategies
Team Communication is essential when a patient is imminently dying in the ED; all team members must understand that the goals of care have shifted to a comfort-focused approach. This includes clear communication within the electronic order system. For example, PRN opioid orders should explicitly state “first line for pain and first line for dyspnea” to ensure symptoms are managed appropriately at the end of life.
Standardized comfort-care order sets help streamline care for imminently dying patients and reduce the risk of missing important steps. Using a consistent medication format ensures nursing staff are familiar with the protocol and can provide timely, effective care.
Interdisciplinary education and training for ED physicians, residents, nurses, and other team members can ensure everyone is equipped to provide high-quality end-of-life care.
Audit and feedback processes can help identify what we are doing well and where we can improve the experience for families of imminently dying patients in the ED. It’s important that any feedback be collected in a respectful and sensitive manner.
Take Home Points
- ED physicians play a pivotal role in caring for imminently dying patients
- Recognizing clinical signs of imminent death can be helpful, but these are not always present
- Symptom relief must be prioritized. Pain and dyspnea are the most distressing symptoms; treat with opioids and account for baseline opioid use
- Early disposition planning and non-pharmacologic strategies are essential components of providing comfort-focused care.
- System-level improvements such as institutional order sets and national ED-specific Canadian guidelines may enhance the quality and safety of end-of-life care in the ED
References
- Abernethy AP, McDonald CF, Frith PA, Clark K, Herndon JE 2nd, Marcello J, et al. Effect of palliative oxygen versus room air in relief of breathlessness in patients with refractory dyspnoea: a double-blind, randomised controlled trial. Lancet. 2010;376(9743):784–93.
- Alberta Health Services. Provincial Clinical Knowledge Topic: Care of the Imminently Dying (Last Hours to Days of Life), Adult – All Locations. Version 1.0. 2018 Jul 12.
- American College of Emergency Physicians. Palliative Care Toolkit [Internet]. Irving (TX): ACEP; c2024 [cited 2025 Nov]. Available from: https://www.acep.org/by-medical-focus/palliative-medicine
- Baylis J, Harris DR, Chen C, Ting DK, Clark K, Kwan A, et al. Palliative and end-of-life care education in Canadian emergency medicine residency programs: a national cross-sectional survey. Can J Emerg Med. 2019;21(2):219–25.
- Bernacki RE, Block SD. Communication about serious illness care goals: a review and synthesis of best practices. JAMA Intern Med. 2014;174(12):1994–2003.
- Caraceni A, Hanks G, Kaasa S, Bennett MI, Brunelli C, Cherny N, et al. Use of opioid analgesics in the treatment of cancer pain: evidence-based recommendations from the EAPC. Lancet Oncol. 2012;13(2):e58–68.
- Corli O, Floriani I, Roberto A, Montanari M, Galli F, Greco MT, et al. Are strong opioids equally effective and safe in the treatment of chronic cancer pain? A multicenter randomized phase IV “real life” trial. Ann Oncol. 2016;27(6):1107–15.
- Diaconu V, Ouellette N, Camarda CG, Bourbeau R. Insight on “typical” longevity: an analysis of the modal lifespan by leading causes of death in Canada. Demogr Res. 2016;35:471–504.
- Elmer J, Torres R, Aufderheide TP, Hess EP, Lindor RA, Marco CA, et al. Death and end-of-life care in emergency departments in the US. JAMA Netw Open. 2022;5(5):e2216273.
- Faris H, Dewar B, Dyason C, Dick DG, Matthewson A, Lamb S, et al. Goods, causes and intentions: problems with applying the doctrine of double effect to palliative sedation. BMC Med Ethics. 2021;22:141.
- Hallenbeck J. Pathophysiologies of dyspnea explained: why might opioids relieve dyspnea and not hasten death? J Palliat Med. 2012;15(8):848–53.
- Hendin A, Hartwick M, Healey A, Fischer L. Improving end-of-life care in the emergency department: development of a standardized approach to the imminently dying patient. Can J Emerg Med. 2020;22(5):626–8.
- Heyland DK, Barwich D, Pichora D, Dodek P, Lamontagne F, You JJ, et al. Failure to engage hospitalized elderly patients and their families in advance care planning. JAMA Intern Med. 2013;173(9):778–87.
- Hui D, Dos Santos R, Chisholm G, Bansal S, Bruera E. Clinical signs of impending death in cancer patients. Oncologist. 2014;19(6):681–7.
- Hui D, Hess K, dos Santos R, Chisholm G, Bruera E. A diagnostic model for impending death in cancer patients: preliminary report. Cancer. 2015;121(21):3914–21.
- Leach C. Nausea and vomiting in palliative care. Clin Med (Lond). 2019;19(4):299–301.
- Loffredo AJ, Chan GK, Wang DH, Goett R, Isaacs ED, Pearl R, et al. United States best practice guidelines for primary palliative care in the emergency department. Ann Emerg Med. 2021;78(5):658–69.
- Morita T, Ichiki T, Tsunoda J, Chihara S. A prospective study on the dying process in terminally ill cancer patients. Am J Hosp Palliat Care. 1998;15(4):217–22.
- Nauck F, Alt-Epping B. Crises in palliative care: a comprehensive approach. Lancet Oncol. 2008;9(11):1086–91.
- Prachanukool T, George N, Bowman J, Ito K, Ouchi K. Best practices in end of life and palliative care in the emergency department. Clin Geriatr Med. 2023;39(4):575–97.
- Sallnow L, Smith R, Ahmedzai SH, Bhadelia A, Chamberlain C, Cong Y, et al. Report of the Lancet Commission on the Value of Death: bringing death back into life. Lancet. 2022;399(10327):837–84.
- Schmidt-Hansen M, Bennett MI, Arnold S, Bromham N, Hilgart JS, Page AJ, et al. Oxycodone for cancer-related pain. Cochrane Database Syst Rev. 2022;6:CD003870.
- Schwartzstein RM, Lahive K, Pope A, Weinberger SE, Weiss JW. Cold facial stimulation reduces breathlessness induced in normal subjects. Am Rev Respir Dis. 1987;136(1):58–61.
- Taburee W, Dhippayom T, Nagaviroj K, Dilokthornsakul P. Effects of anticholinergics on death rattle: a systematic review and network meta-analysis. J Palliat Med. 2023;26(3):431–40.
- Wilson DM, Zhou YL, Bykowski KA, Fiore C, Heron J, Salas AS, et al. Examining the contemporary use of hospitals in Canada for palliative care purposes: a population-based study. J Palliat Med. 2024;27(2):192–200.

