

In general, the public perception of CPR is filled with inaccuracies, and recently the New Yorker wrote about the Hidden Harms of CPR. In the article, Dr. Sunita Puir, a palliative care doctor, talks about how it is an “open secret in medicine that CPR is brutal and rarely effective,” yet how the public seems woefully unaware of this reality.
Watch the entire Grand Rounds here
In the article, Dr. Puir talks about difficult goals of care conversations she’s had and how her failure to accurately depict the reality of CPR has led to codes that are familiar to all of us. The “slow code,” where everyone walks over to the patient at a leisurely pace, the short code where only a round or two of CPR are provided, and the code that is so brutal and inhumane that you feel sick. Reading this article, I started thinking about my own experiences discussing goals of care in the emergency department.
So I want you all to imagine a case. You’re working an evening shift, and you’re in an environment that has become all too familiar; it’s busy, bed blocked, the ambulance bay is full, and CT completion is taking hours.
An 85-year-old male presents in what appears to be a COPD exacerbation. He looks unwell but not critical, you mostly just notice that he looks frail. A scan of his chart shows that he has COPD on home O2, and lung cancer for which he is on second-line treatment. He lives at home with his wife, and today he is there today with his daughter. Following some investigations and treatment you go in and explain to them that he is going to require admission to hospital. I want you to all think for a second, is this a patient you would discuss code status with?
I saw this patient at the beginning of my second year of residency, partially because it was a busy shift, but mostly because I didn’t know if I should say anything or even what I would say – I didn’t say anything at all. I didn’t discuss code status, I didn’t discuss what he would want if things got worse. Instead, I called medical oncology and continued with my shift.
Well, things did get worse. A few hours later the medical oncology resident came and told me that the patient was in respiratory distress, and asked us to help with intubation. Following intubation, he arrested, and after 20 minutes of rib cracking and blood spurting-CPR, he died a painful death.
What struck me most about his family’s reaction was not how upset they were, of course I was expecting that, but how absolutely shocked they were that this could have happened. I remember thinking, “there’s no way that anyone would have chosen to die like this”.
So, everything that went wrong in that scenario is the basis for this post.
Decoding Code Status: Conversations That Matter in the Emergency Department
The goal of this post is to do better than I did. To be better at these difficult conversations, in the challenging environment that we work in. It’s to provide a framework for shared decision-making conversations around goals of care that bridge the gap between what patients know about themselves and their values, and what we know about resuscitation.
First, I want to go over the public’s perception of CPR and resuscitation methods, and contrast that with the “open secret” in medicine about the reality of these therapies. I then want to convince you of something I’ve learned and reflected upon since that shift, which is that emergency room physicians should be the ones having this conversation. Lastly, and most importantly, I want to provide you with a framework for these conversations. Not just the easy conversation on the ward or in the ICU that can take place over a few days, but the fast and critical conversation in the emergency department, as well as the conversation when there are differing opinions with patient or family mebers, and the legal implications of that.
Public’s Perception of CPR vs Reality
First of all, as we’ll talk about, the public is heavily influenced by the CPR that they see on TV. So let’s see what we’re up against:
These depictions of CPR – where Tom Cruise is able to get up and resume fighting the bad guys moments after arresting influence the public’s perception of the success of CPR. In fact, studies have shown that people believe CPR is successful 59% in hospital, and anywhere between 40-60% out of hospital. Research has also shown that this is heavily influenced by television, where on average, patients survive CPR 68.9% of the time. Being trained in CPR or having friends or family who are in medicine did not influence people’s perception on the effectiveness of CPR.
So, what is the reality of CPR?
Locally here in Ottawa, survival to hospital discharge for those with in-hospital cardiac arrest is about 25%.
For out-of-hospital cardiac arrest in Canada, the rates of survival to hospital discharge are between 3.9-7.1%.
As we all know, rates are negatively influenced by conditions like frailty, terminal illness, and progressive organ failure. Of course, this is just survival, and neurologic sequalae following cardiac arrest is high, with studies quoting rates of disability in patients who survive in hospital CPR ranging from 30-50%.
So now we know that there is this huge gap between what patients believe about CPR, vs what we know to be true. And we have to find a way to bridge this gap.
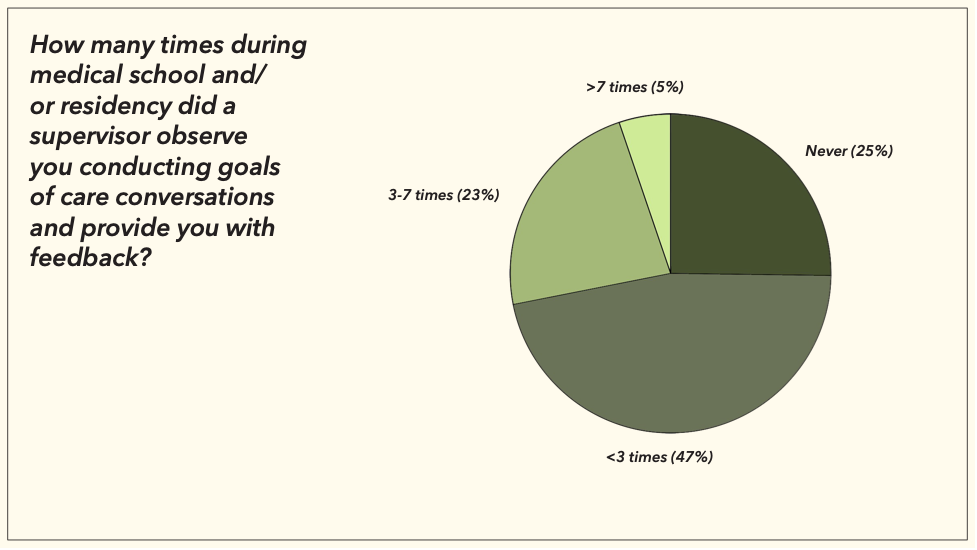
And no one has really told us how to bridge that gap. I surveyed the staff and residents here at The Ottawa Hospital, and out of the 79 respondents, very few had received any feedback on their own goals of care conversations during medical school and residency.
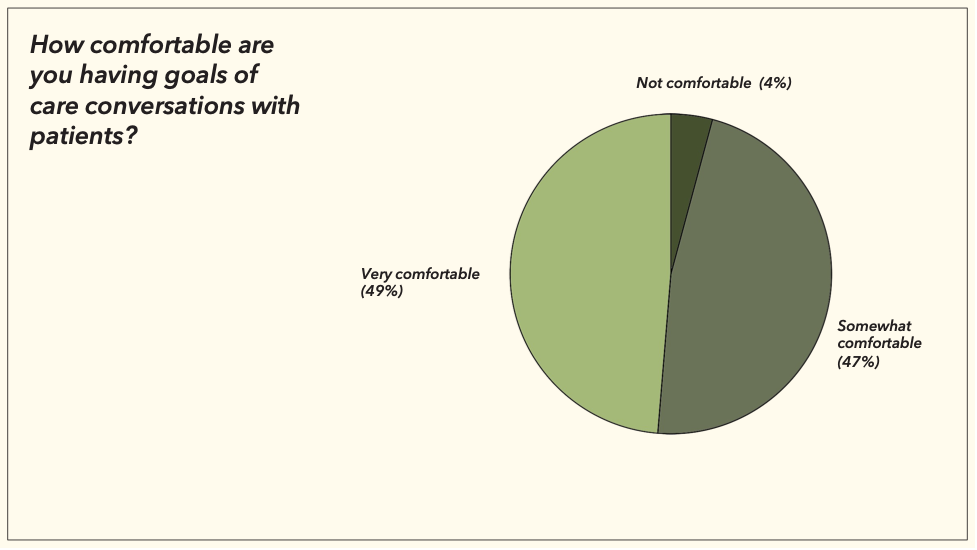
Unsurprisingly, this lack of direct feedback translated into discomfort for some around having goals of care conversations:
This was also reflected in a study done by Dr. Sanders et al, that showed only four out of 17 emergency medicine residents interviewed had had formal education on how to have code status conversations, and residents often felt insufficiently prepared for these discussions.
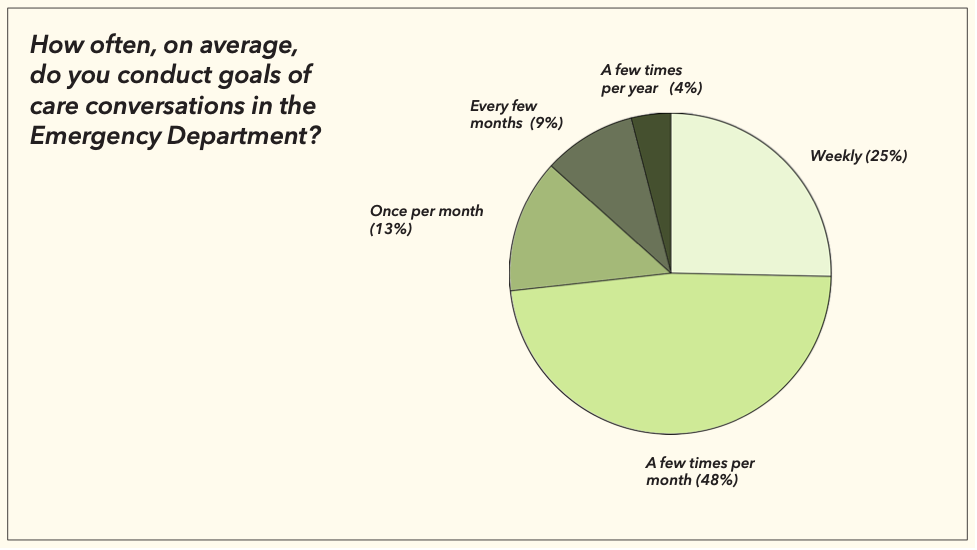
But despite the lack of training, and our relative discomfort around goals of care, these are conversations that we are having all the time. 25 percent of the respondents reported having goals of care conversations weekly, and another 50 percent are having them a few times a month.
ED Physicians should be the ones having goals of care conversations
I now want to convince you that in many cases, emergency room doctors should be the ones having these difficult conversations.
But before we do that, let’s look at another example of CPR from TV shows (for context, the main character, Meredith Grey, has had a hypothermic arrest, but she is now normothermic, and has been in asystole for 20 minutes):
Shortly after this, Dr. Grey spits out her ETT tube, is up, walking and talking and joking around, and goes on to operate within the week.
So why should it be emergency room physicians who are convincing patients that Grey’s Anatomy isn’t real life? The reason is threefold: disposition, moral injury, and because we have no other choice.
Disposition
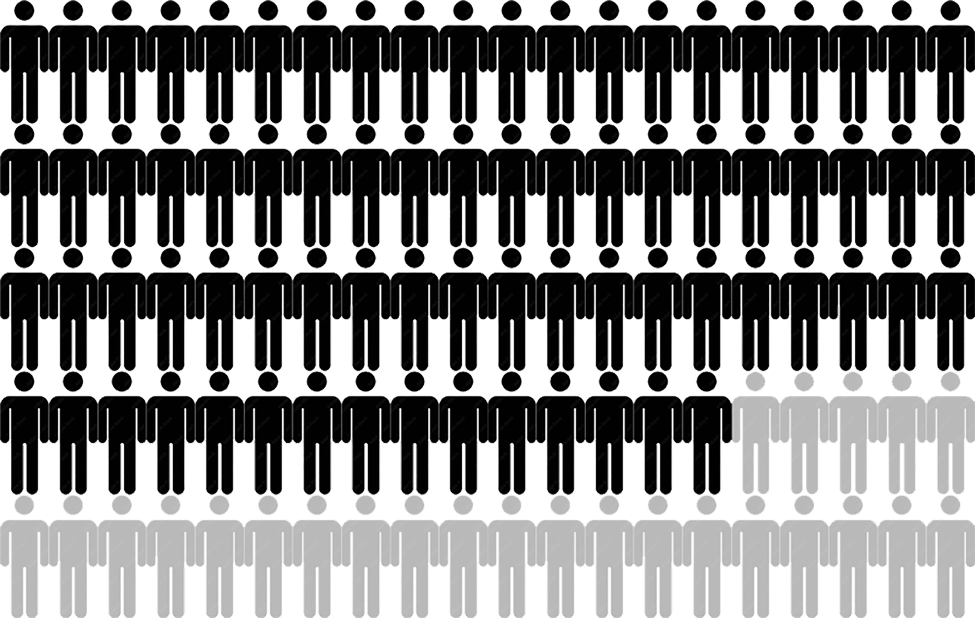
As emergency room physicians, the disposition of patients is our responsibility. Studies have shown that 75% of patients will visit an emergency department within the 6 months before death, and that initiating a palliative care consult from the ED, where appropriate, results in an average of 4 fewer days in hospital, and fewer deaths in hospital. This represents a huge potential for intervention. We have the power, as ED physicians to alter the trajectory of these patient’s admissions.
More importantly, Canadian data has shown that 88% of older adult patients admitted to hospital with a serious illness prefer less aggressive and more comfort-orientated end-of-life care plans that does not include CPR. However, this is only documented in 30% of their charts. By having these conversations early, in the ED, we have the potential to not just alter their admission trajectory, but also impact the way these patients live and die.
Moral Injury
The second reason relates to moral injury. Moral injury, as we’ve all heard many times since COVID-19, is when we feel we’ve violated our conscience or moral compass by taking part in, witnessing, or failing to prevent an act that disobeys our own moral values or personal principles.
To explain this, I want to go back to the story of my bad code conversation. When I was running the code on a patient who I fully knew had no benefit of improving, subjecting him to a painful death, I thought and ruminated about that death afterwards. Even though this was an elderly man, with end-stage organ failure and cancer, I couldn’t get his last moments out of my head. It is likely that most of you reading have stories or moments that are similar.
The reason why this feels so wrong is because we have a duty to provide patients with treatment that is in their best interests. In fact, we took an oath saying we would do exactly that. This goes back to the pillars of medical ethics, non-maleficence, and beneficence. Ultimately, we incur moral injury in these cases because we know, even if our patients don’t know, that in most cases, CPR is of not just of no benefit to them, but actually results in harm.
No other choice
Finally, as our population ages, access to primary care diminishes, and bed blocking worsens, it will be more likely that that patient codes in your department. So like it or not, it is our conversation to have. it will be our moral injury to bear if you’re left performing a resuscitation you know to be futile.
Fortunately, I think that we, as emergency physicians, are expert communicators. We practice and demonstrate our unique communication skills on a daily basis. We have the ability to rapidly synthesize unorganized information into a differential, to reassure a benign chest pain, and to break bad news minutes after meeting a patient. So even if the family doctor or the oncologist hasn’t, we should feel empowered to have this conversation, and not to shrug it off to the junior resident who has been up all night.
It is our clinical obligation to correctly disposition the patient, it will be our moral injury to bear if we don’t, and I think we have the potential to be excellent at it.
Framework for Goals of Care Discussions in the ED
Now that I’ve convinced you that it’s us – ED physicians – who should be having these conversations, let’s look one last time at what we’re up against:
So how exactly do you convince your patient that after a few precordial thumps you won’t be up solving medical mysteries like Dr. House?
Although there is a lot of literature on how to have these conversations, there is very little literature that is specific to the emergency department. In fact, a systematic review published in Emergency Medicine Australia in 2019 looking at primary evidence on goals of care conversations in the emergency department found that there was no evidence for how emergency conversations differ from those in other settings.
Fortunately, there is an abundance of literature on goals of care conversations in general, and many expert opinions on how these models can be modified for the emergency department.
After going through the literature, I’ve come up with a model based primarily on three sources. One is an article from the Annals of Emergency Medicine, created by ED and palliative care physicians, that is based on having succinct, effective conversations around intubation in the ED – but I’ve adapted it for general goals of care. The second source is from Healthcare Quarterly, created by physicians from University of Toronto, London Health Sciences, and University of Western, that focuses on fulfilling your legal and ethical obligation and documentation. The last source I used is the expert opinion of a TOH ICU doctor, Dr. Gianni D’Egidio.
This model is an amalgamation of their work.
| STEP 1: CHART REVIEW | DO: Become a medical expert on your patient, understand their illness, their treatment and recent admissions to hospitalLook for previous GOC conversations, documentation of SDM |
DOCUMENT:
Opinions of other providers Indicators of end-organ damage Indicators of severe disease |
It is critical to understand a patient’s illness and their treatment to date. See if you can find an advanced care conversation documented in the chart. You should become a medical expert on your patient.
| STEP 2: Express urgency, elicit understanding | SAY:
xxx is sick, and we need to act quickly I wish we had met under different circumstances Can you tell me what brought you here today? What do you understand about what happened today? |
DOCUMENT:
Patient/family members understanding of factors contributing to ED visit |
This is when you first sit down with the patient and their loved one. You want to explain the severity of the situation, while at the same time gleaning insight into their understanding of things.
| STEP 3: Determine capacity of patient or determine SDM | DO:
Asses capacity SAY: “Who is the substitute decision maker for X?” |
DOCUMENT:
If patient does not have capacity Who is the SDM |
This post won’t touch on capacity determination, but in the emergency department in times of critical illness it’s often the substitute decision-maker we’re having this conversation with since the patient is regularly too sick to partake.
| STEP 4: Ask for permission, then express severity of situation | SAY:
I’m afraid I have some bad news, is it okay if I share with you? X is very sick I’m afraid I have some bad news, can I explain what I think is going on? X is having trouble breathing I’m worried things could progress quickly I’m concerned things will get worse, and it is possible he could die |
DOCUMENT:
That you explained the severity of the situation |
Asking for permission can feel awkward and clunky, but it’s important because it allows the patient or loved one to have some control in an out-of-control scenario. The sign posting here is key, you want to be sure that you are adequately expressing the severity of the situation.
| STEP 5: Ask about living will/advanced care plan | SAY:
“Do you have a living will?” “Has X ever created an Advanced Care Plan?” |
DOCUMENT:
Presence or absence of a living will |
This step is crucial in determining if the patient or their substitute decision-maker has previously expressed wishes, and often gives you an idea of how the rest of the conversation might go.
| STEP 6: Align yourselves as a team, explain roles | SAY:
“We need to work together to decide on the best plan forward” “have you ever talked about what he would want in this situation?” “Your role, as his SDM is to express X’s values, goals and beliefs, my role, is to provide medical therapies that improve X’s condition for the better, while taking into account those values and goals, together, we will make a plan that is in X’s best interests” |
DOCUMENT:
That you explained the role of SDM |
In this step, you use language that frames yourself as a team, such as “we” statements. But the essential part of this step is explaining roles. We often fail to accurately explain the roles of the substitute decision-maker. When we fail to do this, it centres the SDM in the conversation, rather than the patient, and it forces the responsibility and the weight of these decisions on the SDM. Often, it makes loved ones feel like are the ones who are “pulling the plug,”. Instead, the role of the substitute decision-maker is to act on prior expressed wishes, or to act in the best interests of the loved one. By explaining this to our patients and their substitute decision-makers, we alleviate some of that burden.
| STEP 7: Assess values/goals | SAY:
When you think about the future, is there anything you worry about?
Is there anything we should know about your personal/cultural or spiritual background to help us provide you with the best possible care?
How might he feel if treatments today led to: inability to return to his favourite activites/home/inability to care for himself as much as he does?
What abilities are so crucical that he wouldn’t consider life worth living if he lost them?
How much would he be willing to go through for the possibility of more time?
Are tehre states he would consider worse than dying? |
DOCUMENT:
Goals/values of patient |
This is the point of the conversation where you provide a few leading questions, and then allow the patient or their loved one to speak. Primarily here, you should be listening, and allowing silence. Silence can be awkward, but if there is silence, a good rule of thumb is only to speak again if you are asked a question, if they speak, or if they look at you.
| Step 8: Summarize | SAY:
What I heard is that X considered ___ most important, and that treatments that results in ___ are unacceptable. Did I get that right? |
Summary is key to ensure you’re both on the same page before moving on to the next, and most important part.
| Step 9: Recommendation | SAY:
Based on what you’ve shared, we will provide intensive treatment focused on comfort
Based on what you’ve shared, we will provide him with antibiotics and fluids to treat his infection.
Based on what you’ve shared with me, about how he was afraid of being in pain at the end of his life, we will provide intensive treatment with the goals of getting his breathing to a state that is comfortable with him, providing him with antibiotics, and controlling his pain.
Unfortunately, CPR, and intubation will not alter the fact that your dad is dying, and there is nothing that you or I can do that will change that. These types of therapies will only result in more harm than good, and so it’s not something we can provide.
|
DOCUMENT:
Proposed intervention Which therapies will not be provided |
Here, you want to provide a recommendation and relate it back to their goal. The primary focus here should be highlighting what you WILL do. In all patients, it’s a good idea to express that you will treat their pain and make them comfortable and then tailor the rest to your specific scenario, whether that includes fluids, antibiotics or full resuscitation.
But, importantly, you have to tell the patient, and document in the chart, what therapies will not be provided.
Recommendations in Goals of Care Conversations
I want to take a minute to speak about recommendations as they relate to goals of care. We should be providing a recommendation in all cases, even when the family sees eye to eye with you, or if they have a good understanding of how infrequently CPR works. And the reason is the same as why it is important to explain roles, because it lessens the burden of the family. Goals of care conversations should never be a menu of decision options, but rather a partnership between clinicians and patients where the result is a treatment that is in the patient’s best interest.
In a move away from paternalism in medicine, providing a recommendation has, at times, been criticized as “playing God” But I strongly disagree with that, because we’re not making decisions about who lives and who dies, what we’re doing is using our medical expertise to make decisions about what therapies we know work, and which ones don’t. By using this model of shared decision making, the patient or loved one acts as an expert in their values and wishes, you act an as expert in medicine, and together you make the decision.
And I think this is well highlighted in a commentary written by Dr. Ouchi, who is a Harvard palliative and ED doc and the author of the Annals of Emergency medicine model I referenced earlier. He had the experience of his father having a massive stroke unexpectedly. He sat down to have a goals of care conversation with the intensivist, and upon sitting down the doctor said to him “would your dad want a trach and a PEG tube at age 70?” Dr. Ouchi said that although he is a physician with expertise in this area, he had no idea how to answer this question as the only son of his father. By engaging in shared decision-making, Dr. Ouchi writes, we also share the burden of the responsibility of this decision.
Withholding Resuscitation
The legislation in Ontario was recently changed to allow physicians to refuse, or withdraw from life-saving treatment. This followed a medical malpractice suit that came to the Ontario Superior Court of Justice in 2019 known as Wawrzyniak v. Livingstone.
Elizabeth Wawrzyniak is the daughter of Douglas DeGuerre, an 88-year-old, comorbid man who was admitted to Sunnybrook ICU after a bilateral above-knee amputation secondary to gangrenous infection.
He survived his short ICU stay post-operatively but then developed delirium, necrosis over his surgical sites, and cardiovascular instability. His physicians, Dr. Livingstone and Dr. Chapman, an ICU and internal medicine doctor, noted his decline and made the decision that CPR would not benefit him, and wrote a DNR order on his chart. They attempted to call his daughter to let her know but she was unavailable. Later that evening, his daughter showed up to the hospital and noted him to be in respiratory distress. She called her father’s medical team over for help who began providing breaths, but when Dr. Chapman arrived he requested the team to stop and explained that further resuscitation was of no benefit. Mr. DeGuerre died a short time later while his daughter, who was a nurse, attempted to resuscitate him by herself.
Ms. Wawrzyniak then filed a 2.2 million dollar suit for negligence and malpractice against Dr. Chapman and Dr. Livingston. The case reached the Ontario superior court of justice in 2019 where the allegations were dismissed. The judge ultimately ruled that A physician’s decision to withhold resuscitative measures is not “treatment” and therefore does not require the patient or SDM’s consent. So, just like you don’t need consent to withhold a transfusion for a hemoglobin of 100, or withhold a norepi drip for a MAP of 80, you don’t need consent to withhold CPR for a patient dying of a terminal illness.
Following this, the CPSO updated their policy to reflect this ruling.
The bullet-point version of the policy is that:
- When risk of harm associated with resuscitation outweighs benefits, resuscitation can be withheld
- Before making this decision, consider the wishes and values of the patient
- Tell patient/SDM about what care you will provide
- All attempts should be made to tell patient that resuscitation will be withheld prior to writing the order, but in cases where the patient’s condition is too critical, you can withhold resuscitation and inform the family afterwards.
So what if it still doesn’t work? What if you have an angry family member or patient who still don’t agree with you?
The CPSO says that the physician may still continue with the order to withhold resuscitative measures, but must continue to support the patient and/or SDM by:
- Clarifying any misunderstanding
- Emphasizing what treatment will be provided
- Offering support services (palliative, social work, spiritual care)
- Facilitating a second opinion, where appropriate
- Offering consultation with an ethics committee, where appropriate
Another important resource is your colleagues, both in the ED and ICU, who can provide a second opinion.
In the end, there are many ways to have this conversation, and like intubation, central lines and chest tubes, these conversations involve micro-skills that need to be tuned with time and practice. But, my hope is that all emergency physicians feel empowered to have these conversations. If we do, and even if we don’t do it perfectly, our patients will be better off, our department and hospital will be better off, and we will be better off. Ultimately, I believe that engaging in these conversations will lead to better job satisfaction, improved patient outcomes, and less burnout.
References
- Erath A, Shipley K, Walker LA, Burrell E, Weavind L. Code status at time of rapid response activation — impact on escalation of care? Resuscitation Plus. 2021;6:100102. doi:10.1016/j.resplu.2021.100102
- Pintova S, Leibrandt R, Smith CB, Adelson KB, Gonsky J, Egorova N, et al. Conducting goals-of-care discussions takes less time than imagined. JCO Oncology Practice. 2020;16(12). doi:10.1200/jop.19.00743
- White DB, Evans LR, Bautista CA, Luce JM, Lo B. Are physicians’ recommendations to limit life support beneficial or burdensome? American Journal of Respiratory and Critical Care Medicine. 2009;180(4):320–5. doi:10.1164/rccm.200811-1776oc
- You JJ, Fowler RA, Heyland DK. Just ask: Discussing goals of care with patients in hospital with serious illness. Canadian Medical Association Journal. 2013;186(6):425–32. doi:10.1503/cmaj.121274
- Sibbald R, Chidwick P, Handelman M, Cooper A. Checklist to meet ethical and legal obligations to critically ill patients at the end of life. Healthcare Quarterly. 2011;14(4):60–6. doi:10.12927/hcq.2011.22652
- Ouchi K. A decision with Love. JAMA Neurology. 2021;78(10):1175. doi:10.1001/jamaneurol.2021.2758
- Wawrzyniak v. Livingstone, 2019 ONSC 4900 (CanLII) [Internet]. 2019 [cited 2023 Oct 18]. Available from: https://thaddeuspope.com/images/Wawrzyniak_v_Livingstone_ONT_Sup_Ct_2019_unilateral_DNR.pdf
- Time to talk [Internet]. 2023 [cited 2023 Oct 17]. Available from: https://choosingwiselycanada.org/Serious-Illness-Conversations/
- George N, Bowman J, Aaronson E, Ouchi K. Past, present, and future of palliative care in emergency medicine in the USA. Acute Medicine & Surgery. 2020;7(1). doi:10.1002/ams2.497
- Sinai Health System. Goals of Care Module [Internet]. Sinai Health System; [cited 2023 Oct 17]. Available from: http://goalsofcaremodule.com/
- [Internet]. [cited 2023 Oct 18]. Available from: https://www.pcdm.ca/goc
- Decision-making for end-of-life care [Internet]. [cited 2023 Oct 17]. Available from: https://www.cpso.on.ca/en/Physicians/Policies-Guidance/Policies/Decision-Making-for-End-of-Life-Care
- Downar J, Close E, Sibbald R. Do physicians require consent to withhold CPR that they determine to be nonbeneficial? Canadian Medical Association Journal. 2019;191(47). doi:10.1503/cmaj.191196
- Hall CC, Lugton J, Spiller JA, Carduff E. CPR decision-making conversations in the UK: An integrative review. BMJ Supportive & Palliative Care. 2018;9(1):1–11. doi:10.1136/bmjspcare-2018-001526
- Jones GK, Brewer KL, Garrison HG. Public expectations of survival following cardiopulmonary resuscitation. Academic Emergency Medicine. 2000;7(1):48–53. doi:10.1111/j.1553-2712.2000.tb01891.x
- Mierendorf SM, Gidvani V. Palliative care in the emergency department. The Permanente Journal. 2014;18(2):77–85. doi:10.7812/tpp/13-103
- Di Bari M, Chiarlone M, Fumagalli S, Boncinelli L, Tarantini F, Ungar A, et al. Cardiopulmonary resuscitation of older, inhospital patients: Immediate efficacy and long-term outcome. Critical Care Medicine. 2000;28(7):2320–5. doi:10.1097/00003246-200007000-00023
- van Gijn MS, Frijns D, van de Glind EM, C. van Munster B, Hamaker ME. The chance of survival and the functional outcome after in-hospital cardiopulmonary resuscitation in older people: A systematic review. Age and Ageing. 2014;43(4):456–63. doi:10.1093/ageing/afu035
- Ouchi K, Lawton AJ, Bowman J, Bernacki R, George N. Managing code status conversations for seriously ill older adults in respiratory failure. Annals of Emergency Medicine. 2020;76(6):751–6. doi:10.1016/j.annemergmed.2020.05.039
- Daubman B-R, Bernacki R, Stoltenberg M, Wilson E, Jacobsen J. Best practices for teaching clinicians to use a serious illness conversation guide. Palliative Medicine Reports. 2020;1(1):135–42. doi:10.1089/pmr.2020.0066
- Sanders S, Cheung WJ, Bakewell F, Landreville JM, Rangel C, D’Egidio G, et al. How emergency medicine residents have conversations about life-sustaining treatments in critical illness: A qualitative study using inductive thematic analysis. Annals of Emergency Medicine. 2023; doi:10.1016/j.annemergmed.2023.03.018
- Ouchi K, George N, Schuur JD, Aaronson EL, Lindvall C, Bernstein E, et al. Goals-of-care conversations for older adults with serious illness in the emergency department: Challenges and opportunities. Annals of Emergency Medicine. 2019;74(2):276–84. doi:10.1016/j.annemergmed.2019.01.003
- Hanning J, Walker KJ, Horrigan D, Levinson M, Mills A. Review article: Goals‐of‐care discussions for adult patients nearing end of life in emergency departments: A systematic review. Emergency Medicine Australasia. 2019;31(4):525–32. doi:10.1111/1742-6723.13303
- Dunlay SM, Strand JJ. How to discuss goals of care with patients. Trends in Cardiovascular Medicine. 2016;26(1):36–43. doi:10.1016/j.tcm.2015.03.018
- [Internet]. 2017 [cited 2023 Oct 18]. Available from: http://www.bcehs.ca/our-research-site/Documents/cardiac_arrest_annual_report_2016_2017.pdf
- [Internet]. 2022 [cited 2023 Oct 17]. Available from: https://canroc.org/
- Heyland DK. Failure to engage hospitalized elderly patients and their families in advance care planning. JAMA Internal Medicine. 2013;173(9):778. doi:10.1001/jamainternmed.2013.180
- Heart and Stroke Canada [Internet]. [cited 2023 Oct 18]. Available from: https://www.heartandstroke.ca/-/media/pdf-files/canada/2017-position-statements/final-en-addressingcardiacarreststatement-nov-2019.Ashx?Rev=388eeef4069747dcb4ab6353d36b3f7b%26hash=9e27a3232e8f908e45e115b0b9dcc9d5
- Meaney PA, Bobrow BJ, Mancini ME, Christenson J, de Caen AR, Bhanji F, et al. Cardiopulmonary resuscitation quality: Improving cardiac resuscitation outcomes both inside and outside the hospital. Circulation. 2013;128(4):417–35. doi:10.1161/cir.0b013e31829d8654
- Thompson LE, Chan PS, Tang F, Nallamothu BK, Girotra S, Perman SM, et al. Long-term survival trends of Medicare patients after in-hospital cardiac arrest: Insights from get with the guidelines-resuscitation ®. Resuscitation. 2018;123:58–64. doi:10.1016/j.resuscitation.2017.10.023
- Pound G, Jones D, Eastwood GM, Paul E, Hodgson CL. Survival and functional outcome at hospital discharge following in-hospital cardiac arrest (IHCA): A prospective multicentre observational study. Resuscitation. 2020;155:48–54. doi:10.1016/j.resuscitation.2020.07.007
- Wang DH. Beyond code status: Palliative care begins in the emergency department. Annals of Emergency Medicine. 2017;69(4):437–43. doi:10.1016/j.annemergmed.2016.10.027
- Zanders R, Druwé P, Van Den Noortgate N, Piers R. The outcome of in- and out-hospital cardiopulmonary arrest in the older population: A scoping review [Internet]. U.S. National Library of Medicine; 2021 [cited 2023 Oct 17]. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7938035/#:~:text=Results,following%20IHCA%20and%20OHCA%2C%20respectively.
- Cameron B, Laupacis A. Where do goals of care conversations belong? A case for the emergency department. CJEM. 2019;21(6):698–700. doi:10.1017/cem.2019.364
- Heyland D, Dodek P, Lamontagne F. Advance care planning evaluation in hospitalised elderly patients: A multicenter, prospective study (the accept study). BMJ Supportive & Palliative Care. 2012;2(2). doi:10.1136/bmjspcare-2012-000250.92
- Portanova J, Irvine K, Yi JY, Enguidanos S. It isn’t like this on TV: Revisiting CPR survival rates depicted on popular TV shows. Resuscitation. 2015;96:148–50. doi:10.1016/j.resuscitation.2015.08.002
- Hughes TM, Merath K, Chen Q, Sun S, Palmer E, Idrees JJ, et al. Association of Shared Decision-making on patient-reported health outcomes and healthcare utilization. The American Journal of Surgery. 2018;216(1):7–12. doi:10.1016/j.amjsurg.2018.01.011
- Levinson W, Lesser CS, Epstein RM. Developing physician communication skills for patient-centered care. Health Affairs. 2010;29(7):1310–8. doi:10.1377/hlthaff.2009.0450
- Mills LM, Rhoads C, Curtis JR. Medical student training on code status discussions: How far have we come? Journal of Palliative Medicine. 2016;19(3):323–5. doi:10.1089/jpm.2015.0125
- Schroder C, Heyland D, Jiang X, Rocker G, Dodek P. Educating medical residents in end-of-life care: Insights from a multicenter survey. Journal of Palliative Medicine. 2009;12(5):459–70. doi:10.1089/jpm.2008.0280
- Balaban RB. A physician’s guide to talking about end-of-life care [Internet]. U.S. National Library of Medicine; 2000 [cited 2023 Oct 17]. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1495357/
a really good article, public perception re CPR and intubation is a big issue, but as clinicians we need to take the lead on this and advocate for the patient (which can mean with-holding un-necessary painful interventions), remember, our duty of care, and to minimize harm, is towards the patient, not their family.