

Airway management in the Emergency Department (ED) is challenging. Given the critically ill and physiologically unstable patients, complicated by c-spine collars, distorted anatomy, and airway contamination – the stakes are high. Recent evidence draws attention to an adverse event rate of approximately 8-12% in the ED.1–3 Even more daunting is that with successive attempts, the complication rate rises exponentially.1,4 Clearly, first pass success (FPS) is highly important. Large ED registry data and a meta-analysis suggests that we should be aiming for an FPS of 84%.1–3 But, what is the best tool to accomplish this task? Videolaryngoscopy (VL) or direct laryngoscopy (DL)? The battle rages on…

Photo taken from pixabay.com
Videolaryngoscopy = Direct Laryngoscopy
A recent Cochrane systematic review and meta-analysis was published by Lewis et al. with the conclusion that VL is better than DL, with an OR of failed intubation 0.35 (95% CI 0.19 – 0.65) and an OR of FPS 1.27 (0.77 – 2.09).5 However, this study was limited by a number of factors. There were 64 randomized control trials included with a wide variety of settings, patients, operators, and devices used, highlighting significant clinical and statistical (I2 = 79%) heterogeneity – suggesting that pooling the results across studies may have been inappropriate. In fact, the meta-analysis included only three studies concerning emergent intubation and there was only a single ED-based study by Yeatts and colleagues.6 This large, high-quality trauma study of 623 patients showed a FPS of 81% for DL and 80% for VL (p-value 0.002).
Owing to inconsistencies in the evidence,6–11 we must instead examine factors aside from the specific device in question.
For related reading, check out this recent VL vs. DL RCT by Lascarrou JB, et al. in 2017
Videolaryngoscopy may be superior for the inexperienced operator
There have been hints in the literature that VL may have improved success for novice intubators.7,12 Janz et al. conducted a study on ICU fellows performing emergent intubations, which compared the McGrath Mac VL to standard DL. Although obtaining an FPS of 69% for VL and 66% for DL (p-value 0.68), they carried out a subgroup analysis examining operator experience, either in fellowship or with each device. They found that less experience favoured VL, while more experienced operators had an odds ratio for FPS closer to 1, indicating no difference (see Figure 3).10
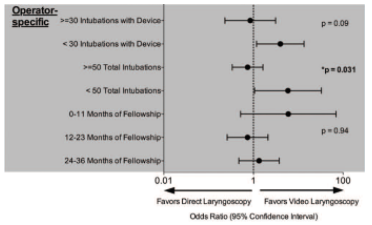
Figure 3 from Janz 2016 10
Videolaryngoscopy may be useful in the difficult airway
Similarly, other studies show that VL may be of benefit when specifically looking at the difficult airway.8,11,13 In 2015, Vassiliadis et al. conducted a large retrospective study examining ED intubations with either the CMAC VL or Macintosh DL.11 They found that if the operator encountered a Cormack-Lehane (CL) grade I-II, they had a FPS of 95% with VL and 96% with DL. But, when encountering a CL III-IV, operators obtained a FPS of 57% for VL and 30% for DL with an OR of 3.1 (1.5 – 6.7) favouring VL.
However, perhaps the debate can be shifted. Maybe we should refocus our energy on a device that can perform both VL and DL. Enter the Macintosh geometry VL…
Macintosh Videolaryngoscopy may be the optimal device for the ED environment
Mac VL device geometry allows for utility as both DL and VL if needed.
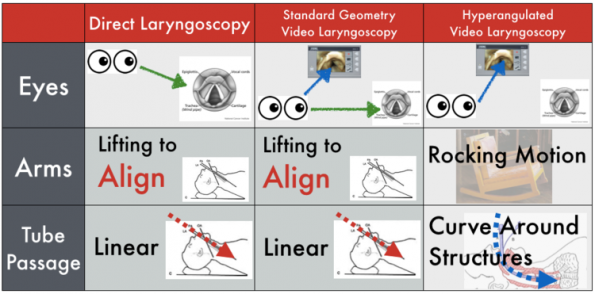
Image taken from Taming the SRU 2014
Mac geometry favours keeping the oral, pharyngeal, and laryngeal axes in line, facilitating smooth passage of the endotracheal tube. This technique avoids the adjustments frequently needed to troubleshoot the acute angle obtained with hyperangulated VL devices like the Glidescope.14 Learners can also train using DL with these devices, with the added safety benefit of a video screen for the supervising staff.
Evidence has shown that the CMAC (Mac geometry device) can be used as a DL and may have improved first and second pass success in ED intubations compared to standard DL.9,15 When comparing to other types of VL, the CMAC (and similar Mac VL) outperformed in the Cochrane review and in ED studies.3,5 In fact, the NEAR registry demonstrated a FPS for Mac VL of 91%, compared to 84% for DL and 80% for the Glidescope.
Bottom Line:
- Videolaryngoscopy = Direct Laryngoscopy for the majority of airways
- Videolaryngoscopy may be useful in difficult airways and with less experienced providers
- Mac Videolaryngoscopy may be the optimal choice for the ED environment
References
- Kerslake D, Oglesby AJ, Di Rollo N, James E, McKeown DW, Ray DC. Tracheal intubation in an urban emergency department in Scotland: A prospective, observational study of 3738 intubations. Resuscitation. 2015;89(C):20-24.
- Park L, Zeng I, Brainard A. Systematic review and meta-analysis of first-pass success rates in emergency department intubation: Creating a benchmark for emergency airway care. EMA – Emerg Med Australas. 2017;29(1):40-47.
- Brown CA, Bair AE, Pallin DJ, Walls RM. Techniques, success, and adverse events of emergency department adult intubations. Ann Emerg Med. 2015;65(4):363-370.e1.
- Mort TC. Emergency Tracheal Intubation: Complications Associated with Repeated Laryngoscopic Attempts. Anesth Analg. 2004:607-613.
- Lewis SR, Ar B, Parker J, Tm C, Af S. Videolaryngoscopy versus direct laryngoscopy for adult patients requiring tracheal intubation. Cochrane Library. 2016;(11)
- Yeatts DJ, Dutton RP, Hu PF, et al. Effect of video laryngoscopy on trauma patient survival. J Trauma Acute Care Surg. 2013;75(2):212-219.
- Silverberg MJ, Li N, Acquah SO, Kory PD. Comparison of Video Laryngoscopy Versus Direct Laryngoscopy During Urgent Endotracheal Intubation. Crit Care Med. 2015;43(3):636-641.
- Mosier JM, Stolz U, Chiu S, Sakles JC. Difficult airway management in the emergency department: GlideScope videolaryngoscopy compared to direct laryngoscopy. J Emerg Med. 2012;42(6):629-634.
- Sakles JC, Mosier JM, Patanwala AE, Arcaris B, Dicken JM. The Utility of the C-MAC as a Direct Laryngoscope for Intubation in the Emergency Department. J Emerg Med. 2016;51(4):349-357.
- Janz DR, Semler MW, Lentz RJ, et al. Randomized Trial of Video Laryngoscopy for Endotracheal Intubation of Critically Ill Adults*. Crit Care Med. 2016;44(11):1980-1987.
- Vassiliadis J, Tzannes A, Hitos K, Brimble J, Fogg T. Comparison of the C-MAC video laryngoscope with direct Macintosh laryngoscopy in the emergency department. EMA – Emerg Med Australas. 2015;27(2):119-125.
- Griesdale DEG, Liu D, McKinney J, Choi PT. Glidescope® video-laryngoscopy versus direct laryngoscopy for endotracheal intubation: a systematic review and meta-analysis. Can J Anesth Can d’anesthésie. 2012;59(1):41-52
- Ahmadi K, Ebrahimi M, Hashemian AM, Sarshar S, Rahimi-Movaghar V. Glidescope video laryngoscope for difficult intubation in emergency patients: A quasi-randomized controlled trial. Acta Med Iran. 2015;53(12):738-742.
- Bacon ER, Phelan MP, Doyle DJ. Tips and Troubleshooting for Use of the GlideScope Video Laryngoscope for Emergency Endotracheal Intubation. Am J Emerg Med. 2015;33(9):1273-1277
- Sakles JC, Mosier JM, Patanwala AE, Dicken JM, Kalin L, Javedani PP. The C-MAC?? video laryngoscope is superior to the direct laryngoscope for the rescue of failed first-attempt intubations in the emergency department. J Emerg Med. 2015;48(3):280-286.

