
In this post, we will discuss updates and controversies surrounding rate control in Afib, specifically we will:
- Review the new 2017 CAEP Afib best practices guidelines
- Review Tachycardia Induced Cardiomyopathy
- Review Afib and Type 2 ACS
- Discuss the identification and management of secondary Afib
2017 CAEP AAF Best Practices Guideline Update:
Risk Stratification:
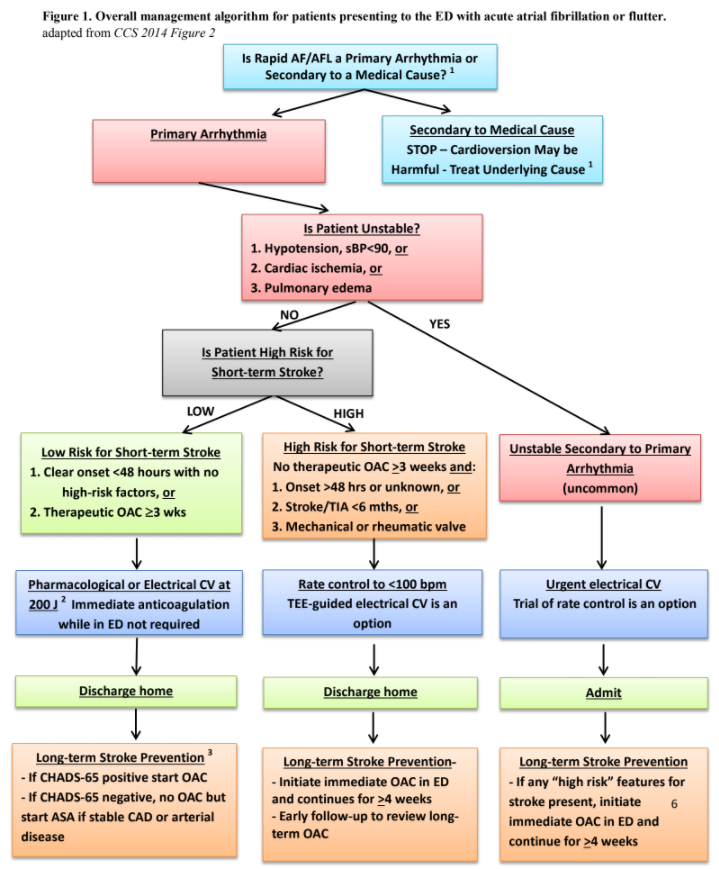
- Unstable AAF (Acute Afib) is very rare:
- This entity should only be considered if there is new significant hypotension sBP <90 and signs of hypoperfusion, severe ongoing cardiac chest pain, or significant pulmonary edema (crackles, hypoxia, dyspnea)
- Do not treat AAF if it is secondary to a medical cause
- Investigate underlying disease processes aggressively and treat as indicated
- Cardioversion can be harmful
- Avoid rate control
- Secondary Afib is a compensatory state and will resolve once the underlying disease processes has been treated. It should not be the primary focus of treatment and the patient is not likely to be harmed by a transient rapid HR.
- Consider patients with Onset of RAFF (recent-onset atrial fibrillation and flutter) >48 hours, Stroke/TIA within 6 months, and mechanical valve (INR <2.5) to be high risk for a short-term stroke and opt for rate control
- 48-hour window for AAF onset is expert opinion and has never been validated as a safe time-frame for cardioversion of AAF
- Consider patients with onset of AAF >24hours and ≥2 CHADS risk factors to be high risk for a short term stroke
- As per 2014 study published by Nuotio et al. in JAMA [3]
- Risk in this group of a thromboembolic complication is 1.1% at 30 days as compared to 0.3% if presentation <24 hours.
- Extrapolating this data over a year, the risk of embolism is larger with cardioversion than if you left the patient in AAF without anticoagulation
Rhythm Control Strategy:
- Either electrical or pharmacological cardioversion is acceptable and remains at the discretion of the treating physician and patient preference
- Drug of choice is Procainamide 15mg/kg IV in 500cc NS over 30-60min
- Avoid if hypotension or QTc >500
- Amiodarone is not recommended for pharmacological cardioversion
- Drug of choice is Procainamide 15mg/kg IV in 500cc NS over 30-60min
- Electrical cardioversion is suggested to start at 200J
Rate control strategy:
- First line therapy with either CCB IV (Diltiazem) or BBer IV (Metoprolol) is acceptable
- No current convincing evidence of superiority for either class over the other
- If patient is chronically managed on one class then opt to begin therapy with the same medication. Do not cross classes if possible and consider cardiology referral/admission if required
- Begin PO dosing in the ED within 30 min of adequate rate control
- Diltiazem 30-60mg po
- Metoprolol 25-50mg po
- Target HR 100 at rest and HR 110 with exertion
- Second line therapy is Digoxin IV
- Consider first line if patients present with hypotension or acute heart failure (HF)
Controversial topics!
Calcium Channel Blockers (CCB) vs Beta Blockers (BB) in RAFF and HF:
The vast majority of the evidence on this topic is based off of old Cardiology literature. Currently there have not been adequate trials conducted in the ED assessing the safety and efficacy of these classes of drugs when given in the ED for rate control to patients with known or new onset HF.
-
- Evidence to avoid CCB in heart failure patients is extrapolated from the MDPIT trial [4]
- CCB increased mortality in patients on long-term CCB therapy for HF
- Vast majority of these patients were in sinus rhythm
- CCB increased mortality in patients on long-term CCB therapy for HF
- Evidence of BBs safety in HF is extrapolated from CIBIS [5], COPERNICUS [6], and MERIT-HF [7]
- Trials showed improved mortality in patients with HF on long term BB therapy
- Once again, the vast majority of patients were in sinus rhythm
- Trials showed improved mortality in patients with HF on long term BB therapy
- No study has been performed on whether IV BBs are safer to give to patients with HF for rate control in RAAF than CCB.
- Expert opinion in Ottawa from Cardiology is that in IV doses, both medications will cause substantial myocardial suppression and should be avoided if signs or symptoms of HF
- Expect no difference in myocardial suppression when given as a push dose vs. in a minibag except for delay in onset of action
- Evidence to avoid CCB in heart failure patients is extrapolated from the MDPIT trial [4]
How to assess AAF patients for occult HF:
- History
- Not sudden onset, no palpitations, sub-acute course, permanent Afib, new SOBOE, Orthopnea, PND
- Physical
- Low Grade shock, narrow pulse pressure, confused, delirious, decreased urine production
- Labs
- Low threshold to investigate
- Add LFTs, VBG, and Lactate to assess for signs of hypoperfusion
- Low threshold to investigate
- PoCUS
- BEST MODALITY!!
- Assess Cardiac function in real time, but you must know your skill level
If any of these investigations shows signs of HF then IV BB and IV CCBs should be avoided as first-line agents in rate control for RAFF
Recommended Management of AAF and HF
- Assess patient for signs of HF (History, Physical, Labs, PoCUS)
- First line is IV Digoxin loading dose unless significant renal failure
- If there are signs of HF a Cardiology referral is indicated and admission should be considered
- Controlling the HR in these patients should be done slowly and in a closely monitored setting
Does Digoxin Increase Rates of Conversion to Sinus Rhthym?
A frequent question surrounding Digoxin is whether its use results in higher rates of cardioversion to sinus rhythm thus, endangering patients who are high risk for a short-term stroke and are ideally managed by rate control?
- No solid evidence that Digoxin increases cardioversion rates to sinus rhythym over placebo in the Canadian ED population. Previous studies have looked at US or international populations and we cannot extrapolate these results to the Canadian RAAF population as we opt for a rhythm control strategy more frequently.
- Expert opinion in Ottawa is that you probably get more conversion to sinus rhythm but it may not be significant
- Increased benefit for avoiding hypotension associated with CCB/BB accounts for the slight increased stroke risk of converting to sinus rhythm
Tachycardia Induced Cardiomyopathy (TIC):
What is TIC?
-
- Reversible systolic or diastolic ventricular dysfunction seen in patients with prolonged rapid heart rate that reverses upon controlling the tachydysrhythmia
- Onset usually takes weeks of rapid HR and recovery is over the course of months
- Classically, TIC develops with slower tachyarrhythmias (HR <140) as they are less symptomatic and thus are more likely to present after being in a rapid HR for a longer period.
- Overall incidence of TIC in Aflutter patients managed with a rate control strategy at time of ablation was approximately 14% in Ottawa [8]
- The only independent predictor for developing TIC in this population was ventricular rate
Why does TIC Matter?
- These are high risk patients
- They have occult/new onset HF
- Aggressive treatment with BB/CCB is potentially life threatening → results in cardiogenic shock
- This is a patient population that if not recognized could have a significant adverse outcome as a result of usual care
When to suspect TIC:
- Requires a high index of suspicion
- Signs and symptoms of new HF
- Prolonged course of symptoms increases likelihood
- Patient unable to feel palpitations
- Patients with permanent Afib/Flutter and poor rate control medication compliance
What to do if you suspect TIC:
- Refer, Admit to Cardiology
- Consider Digoxin as a rate control agent if appropriate (eg. No severe renal failure)
- Treatment is to slow down the HR, but recovery of LVEF is over the course of months and there is no rush to control HR rapidly
- Typically, these patients will have a TTE and cardioversion as an inpatient followed by intensive follow-up and treatment to ensure recovery of LV function
RAFF and ACS:
What do you do if you have a person in RAFF and they have a troponin elevation >95%tile
- If you think that this is a Type 1 ACS treat as such and ignore the Afib as this is secondary
- If the patient is unstable secondary to AAF:you need to consider cardioversion
- If it’s Type 2 ACS (supply-demand ischemia) ignore the initial trop and treat Afib as per our guidelines
- After treatment obtain a 0-3-6 hour TNI to look for a plateau
- If the troponin plateaus: discharge home and refer to Cardio as an outpatient for stress test/risk stratification
- If the troponin continues to elevate: refer to Cardio as these patients are higher risk and may require more urgent invasive testing
- After treatment obtain a 0-3-6 hour TNI to look for a plateau
For further information on Afib:
- See our review of the 2014 Canadian management guidelines : Part 1, Part 2, Part 3
- Dr. Matthew Lipinski’s review of Select Cardiac Arrhythmias in the ED
- Journal Club:
References:
- Stiell I, et al. “CAEP Acute Atrial Fibrillation/Flutter Best Practices Checklist” Publication pending 2018.
- Nuotio I, Hartikainen JE, Gronberg T, Biancari F, Airaksinen KE. Time to cardioversion for acute atrial fibrillation and thromboembolic complications. JAMA 2014; 312(6):647-649.
- Goldstein N, Boccuzzi S, Cruess D, Nattel S. Diltiazem increases late-onset congestive heart failure in postinfarction patients with early reduction in ejection fraction. The Adverse Experience Committee; and the Multicenter Diltiazem Postinfarction Research Group. Circulation. 1991;83:52-60, originally published January 1, 1991
- CIBIS-II Writers. “The Cardiac Insufficiency Bisoprolol Study II (CIBIS-II): a randomised trial”. The Lancet. 1999. 353(9146):9-13.
- Packer M, et al. “Effect of Carvedilol on the Morbidity of Patients With Severe Chronic Heart Failure”. Circulation. 2002. 106(17):2194-9.
- Fagerberg B, et al. “Effect of metoprolol CR/XL in chronic heart failure: Metoprolol CR/XL Randomised Intervention Trial in Congestive Heart Failure”. The Lancet. 1999. 353(9169):2001-7.
- Pizzale S, et al. “Frequency and predictors of tachycardia-induced cardiomyopathy in patients with persistent atrial flutter”. Can J Cardiol. 2009 Aug; 25(8): 469–472.

