

Traumatic injuries are amongst the most common presentations for all emergency departments (ED). In 2010, there were over 1 million patients in Canada who visited the ED for trauma, result in an cost of almost 9 billion dollars.1 Yet, in spite of their frequency, there remains a great deal of practice variation and uncertainty about the optimal imaging approach in these patients. In this post, we will explore the existing and emerging evidence of imaging in selected traumatic presentations.
First, we will discuss the nuances of cervical spine (C-spine) imaging, focusing on:
- Using X-ray vs. computed tomography (CT) for clearing the C-spine
- The role of flexion-extension radiography after a normal C-spine CT
- Indications and evidence supporting or refuting the use of magnetic resonance imaging (MRI) after a normal C-spine CT
In the second part, we will focus on the use of immediate whole-body CT (WBCT) in the high-energy blunt trauma patient, covering:
- A brief historical overview
- Limitations of the earlier literature on WBCT
- Latest evidence on the role of WBCT for severely injured patients
Part 1 – Imaging the C-spine
What is the imaging of choice in the young adult whose C-spine cannot be cleared clinically?
In 2009, the Eastern Association for the Surgery of Trauma (EAST) updated their guidelines to recommend CT unconditionally (if available).2 Most of the studies that influenced their recommendations are summarized in a meta-analysis by Holmes published in 2005:
- This meta-analysis found a pooled sensitivity for X-ray identifying C-spine injuries of 52%.3
- Unfortunately, of the seven studies included, four of them were in populations not representative of the majority of the ED patients evaluated for C-spine injuries
- One was in ICU patients, a second only in patients with GCS scores less than 9, and two of them in patients with altered mental status
- Consequently, the C-spine injury rates in these studies ranged from 5% to 76% representing much more injured population than the average ED patient
- The impressively high C-spine injury rate makes the conclusions of these studies difficult to apply in a Canadian C-spine Rule population with a C-spine injury rate of 1.2-2.4%. 4
The gains in performance from CT must be weighed against the possible downsides of completely replacing X-ray with CT: what will be the effect of patients waiting for imaging? Increased radiation doses for younger patients? Expected increases in volume from community centres transferring patients to have their C-spines cleared with CT?
While the evidence certainly suggests that X-ray is insufficiently sensitive to clear the C-spine in the severely injured patient or those at high risk of C-spine injury, the evidence dissuading the use of X-ray in the young cooperative and neurologically intact patient is lacking. Our local Spine Surgery experts agree that the EAST guidelines are neither practical nor realistic. However, they also highlight the importance of being weary on relying solely on X-ray when clearing the C-spine.
Bottom Line: C-Spine X-ray vs. CT
The EAST guidelines’ unconditional recommendation of using CT as the primary imaging modality in clearing the C-spine is based on evidence in severely injured patient populations with high risk of C-spine injury. While in these patient groups X-ray is insufficiently sensitive, evidence questioning its use in the young cooperative patient at low-risk of C-spine injury is lacking.
What is the role of flexion-extension radiographs after a normal CT of the C-spine?

The purpose of flexion-extension C-spine radiographs (FECSR) is to assess for instability after major hyperextension and hyperflexion forces, and they were most commonly performed in the pre-CT era. An adequate FECSR involves complete visualization of the C-spine to T1, at least 30° of flexion, and at least 30° of extension. A systematic review from a group in the Netherlands published in 2013 aimed to assess the test performance of FECSR in identifying C-spine injuries5:
- This review included six high quality studies totaling 1,324 patients
- Overall, they found that the rate of obtaining adequate FECSR varied dramatically between studies and were unacceptably low
- Five of the six studies obtained adequate FECSR less than 70% of the time
- Both the sensitivity and specificity of FECSR in detecting ligamentous injuries in this systematic review anged from 0 to 100 %
- From all the studies, zero clinically significant injuries were identified by FECSR after a negative CT
- Although limited by the high clinical heterogeneity and low ligamentous injury rate (1.1 %), this systematic review seriously questions whether there is a role for FECSR after a normal C-spine CT
Corroborating the conclusions from this systematic review, a large retrospective study over a seven year period published in 2016 reported similar test performance characteristics.6 The authors included 2,404 patients who had a normal C-spine CT and investigated the diagnostic value of adding FECSR when compared to the reference gold standard of MRI or surgical intervention for unstable injuries. Overall, 176 FECSR were performed and 4 abnormalities were identified. MRI demonstrated that the 4 patients with abnormal FECSR were false-positives, and an additional 4 patients had MRI abnormalities that were not clinically-significant injuries. The sensitivity for FECSR in this large retrospective study for identifying unstable C-spine injuries after a normal C-spine CT was 0%.
Bottom Line: Flexion-Extension Radiographs
There is no role for flexion-extension radiographs in the ED after a normal 64-slice C-spine CT.
What is the role of MRI in the patient who has persistent C-spine tenderness or isolated paresthesias?
Three of the traditional reasons to think about MRI in the patient with suspected C-spine injury include:
- Persistent neck tenderness
- Neurological findings, and
- The obtunded and unexaminable patient
There is a wealth of literature for clearing the C-spine in the obtunded patient that will not be covered here, as this scenario pertains more to our trauma and critical care colleagues. With the evolution of a new generation of CT scanners, the question remains as to the yield of adding MRI to these patient groups after a normal C-spine CT.
Although there is abundant literature on the obtunded patient, far fewer studies focus on awake and alert patients. In 2017 Maholtra et al. published a meta-analysis of 23 studies that included patients that received MRI after a normal C-spine CT.7
- Out of the 5,286 patients in their study, MRI showed an abnormality in 15% and a clinically significant injury in 0.3 %
- In the subgroup of 1,387 awake and alert patients (which includes patients with persistent tenderness and neurological deficits):
- MRI identified an abnormality in 7% and a clinically significant injury in 0.7%
- This large meta-analysis showed that although MRI detects a significant number of injuries after a negative CT, a small minority of these are unstable
- The strength of this meta-analysis’ conclusions are tempered by the:
- High clinical heterogeneity of the studies included
- High number of retrospective studies
- Use of the 3-column model of instability as the definition of clinical significant injury
One of the most useful studies included in the meta-analysis by Maholtra was a prospective study by a group in California published in 2014.8
- They analyzed the clinically significant injury rate (defined by surgical intervention, use of halo, or mandatory rigid collar) of 830 consecutively enrolled patients who were alert and had either persistent neck tenderness or a neurological deficit
- Overall, 2.8% of patients had clinically important injuries
- Of the 100 MRIs that were performed after a negative CT, 15% of them identified an abnormality but no clinically important injuries were diagnosed
- The sensitivity for a modern 64-slice C-spine CT in detecting clinically important injuries in this study was 100 %, and MRI did not add any useful information in patients with persistent tenderness
- A major limitation to consider in interpreting their results is that only 100 MRIs were performed, and the majority of them were due to equivocal findings on CT
Building on these findings, the authors conducted a multi-centre trial involving 18 North American trauma centres including one Canadian site.9
- They studied over 10,000 patients suspected for C-spine injury, and over 5,000 of these patients were alert and complained of persistent midline tenderness
- The authors found that out of the 9,178 negative CTs, three clinically significant injuries were missed
- All three of these patients had motor deficits consistent with central cord syndrome that warranted an MRI regardless
- Although the sensitivity for CT in detecting clinically significant C-spine injuries was 98.5%, none were missed when CT was combined with a motor exam
- The large sample size of patients with persistent midline tenderness makes the conclusions of this study generalizable to this patient population
- However, although these results certainly suggest a limited role for MRI in patients with a normal CT and sensory deficits, only 576 patients had neurological deficits and fewer than 200 had sensory phenomena.
Bottom Line: MRI in Persistent Neck Tenderness and Isolated Paresthesias
MRI adds no clinically useful information in the patient with persistent neck tenderness after a normal 64-slice C-spine CT. There is emerging evidence suggesting that the role of MRI is questionable for patients with isolated paresthesias. MRI is warranted for all patients with an abnormal motor exam.
Summary: Approach to Imaging the C-spine
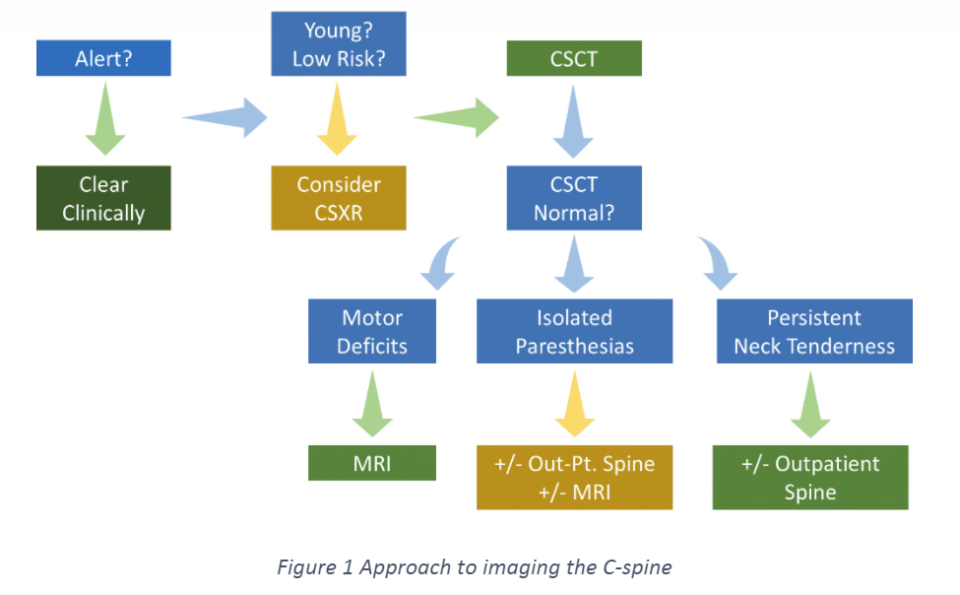
- If the patient is alert, the priority should be to clear clinically using the Canadian C-spine Rule
- If unable to clear clinically, then consider whether they are young and low risk for C-spine injury (there is no externally validated tool in risk stratifying these patients).
- C-spine X-rays can be considered, but if relying on them to clear the C-spine then it is imperative that patients understand they need re-assessment if their symptoms are progressing or if they have persistent neck tenderness
- CT clearly outperforms X-ray
- Otherwise, C-spine CT is the imaging modality of choice. If the CT is completely normal, then consider whether the patient has motor deficits, isolated paresthesias, or persistent neck tenderness
- Patients with motor deficits require an MRI
- There is emerging evidence that the value of MRI for patients with isolated paresthesias and a normal C-spine CT is low. MRI can still be considered, however an alternative is outpatient spine follow-up for reassessment.
- The best evidence suggests there is no additional value of MRI in patients with persistent neck tenderness after a normal C-spine CT.
Part 2 – Immediate WBCT or Selective Imaging in the High-Energy Blunt Trauma Patient
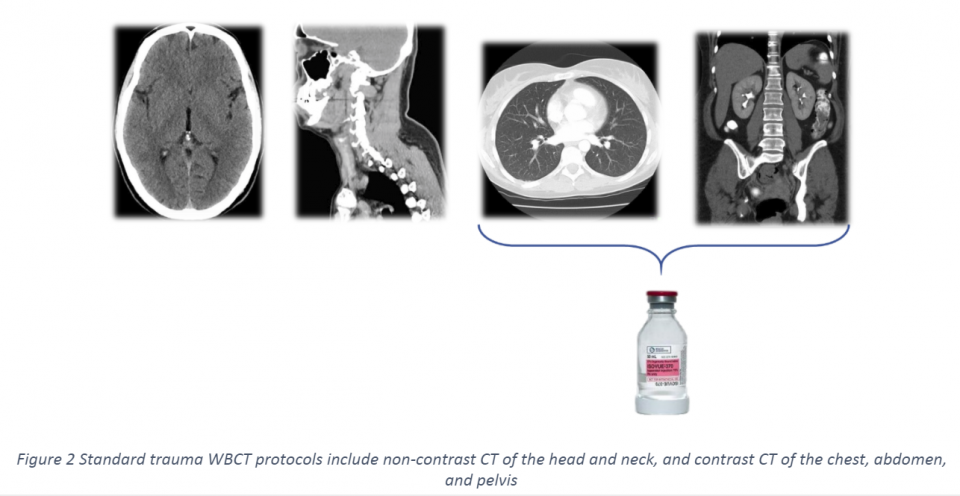
Advancements in CT technology have transformed how we manage severely injured patients. With the introduction of multi-detector scanners, we are obtaining thinner-slices resulting in higher resolution and shorter acquisition times. These two key innovations were instrumental in the development of rapid WBCT techniques. A standard trauma WBCT consists of:
- Non-contrast CT of the head and neck
- Contrast CT of the chest, abdomen, and pelvis (ideally with spine reformatting)
The adoption of immediate WBCT in trauma was paved by early studies that showed decreased time in the ED of up to 30 minutes, and impressive mortality decreases of up to 36 %.10 However, opponents of its widespread use warned of increased costs, radiation, and uncertainty in the management of incidental findings. By some estimates, as few as 300 WBCTs in trauma can contribute to one additional cancer-related death.11 The debate on the use of a widespread immediate WBCT strategy vs. a selective-imaging approach has been fierce.
For information regarding decision rules for selective use of CT Chest in blunt trauma see this journal club article and a previous Grand Rounds Summary by Dr. Francis Bakewell
Limitations of the Early Immediate WBCT Literature
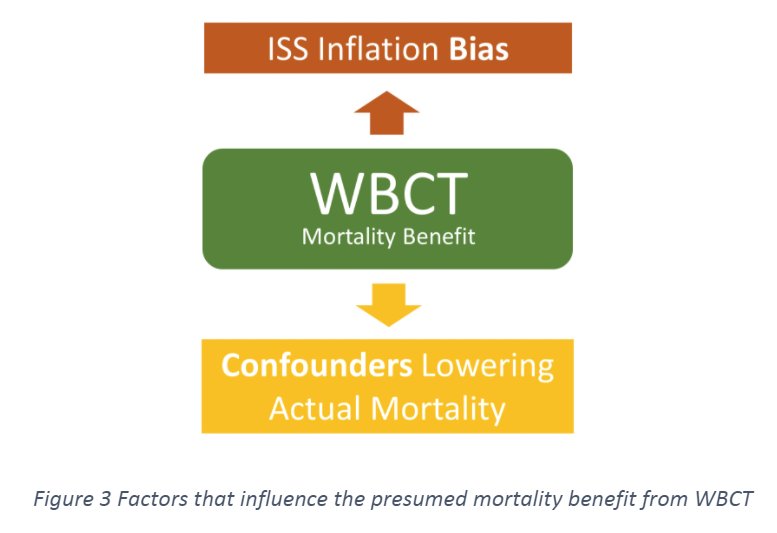
There are two main forces that limit our ability to draw conclusions from much of the earlier trauma WBCT literature. The first includes confounders that affect the actual mortality of patients studied, and the second is the concept of injury severity score (ISS) inflation.12
Confounders Lowering Actual Mortality
Since a large portion of the trauma WBCT literature relies on retrospective and registry data, pooled results are affected by a high degree of clinical heterogeneity. Ultimately, researchers’ goal is to determine whether immediate WBCT confers a mortality benefit compared to selective imaging. However, many trauma centres that adopted rapid WBCT protocols also saw other advancements that improved trauma care, including:
- Earlier balanced transfusions
- More aggressive access to interventions
- More rapid definitive surgical therapies
- Or even just the expertise of personnel that handle routine traumas
All of these factors are major confounders that will lower mortality and were seen alongside adoption of immediate WBCT.
To use sepsis as an analogy: what we need to determine is whether immediate WBCT is more akin to administering early antibiotics or measuring the central venous pressure. The take home point is that from retrospective and registry data it is difficult to unbundle immediate WBCT from the rest of trauma management.
ISS Inflation
The second limitation of the earlier WBCT literature is the phenomenon of ISS inflation. Since performing a WBCT will identify more occult injuries, the reported injury severity of these patients is higher than patients undergoing selective imaging. The ISS is an anatomic score of injury severity that – along with other severity indexes – is used to predict mortality. Studies that retrospectively compare patients who received immediate WBCT against selective imaging, have a tendency to attribute a higher ISS to the immediate WBCT group due to the uncovering of otherwise unidentified injuries. While these findings might not alter the management or actual prognosis of patients, they elevate their ISS. Consequently, retrospective studies have the risk of falsely attributing that the gap observed from actual mortality and predicted mortality is due to immediate WBCT improving survival rather than on it artificially increasing their predicted mortality.
Recent Evidence Comparing Immediate WBCT and Selective Imaging
There are multiple systematic reviews and meta-analyses comparing immediate WBCT with selective imaging – each with slightly different inclusion criteria, results, and conclusions. The latest meta-analysis was published in 2017 in Injury.13
- The authors included 11 trials: one randomised controlled trial (RCT), five prospective cohort studies, and five retrospective studies
- They found a pooled mortality benefit in favour of an immediate WBCT strategy with an odds-ratio (OR) of 0.74 (95% confidence interval 0.61-0.91)
- From the three studies that reported time spent in the ED, they found a decrease of 14 minutes in the ED length of stay
- One of the main limitations of this meta-analysis was the degree that their results were driven by retrospective studies
- The RCT included in their analysis was REACT-2 published in The Lancet in 201614 and currently represents the highest quality of evidence in this topic
- They prospectively included trauma patients with either significant vital sign abnormalities, major traumatic diagnoses, or high energy mechanisms and randomised 1,403 patients to either an immediate WBCT or a selective imaging strategy
- The study was conducted in five trauma centres – four in the Netherlands and one in Switzerland
- Overall, they found that the in-hospital and 30-day mortality was identical in both groups (16%)
- In sub-group analysis, there was also no difference in mortality between the imaging arms in polytrauma patients and those with traumatic brain injury
- They report that there was a significantly lower median radiation dose in the selective imaging group (20.6 mSv, range 9.9-22.1) compared to the immediate WBCT group (20.9 mSv, range 20.6-20.9), as 45 % of patients in the selective imaging arm received radiation doses lower than 20 mSv
- This is the first RCT to evaluate whether immediate WBCT confers a mortality benefit compared to selective imaging, however it carries with it some significant limitations
- While they found no mortality benefit, the results are limited by the high rate of patients in the selective imaging group receiving a WBCT (46 %)
- Although this does not represent true crossover, it highlights the reliance on WBCT in severely injured patients
- The lower radiation dose seen in the selective imaging group is also driven by a lower range, rather than a clinically important decrease in the median radiation dose
- The study also used broad inclusion criteria resulting in over a third of patients having an ISS less than 16, however this also represents the reality of trauma assessment in that severely injured patients will actually have a wide range in ISS depending on their injury distribution
- Lastly, our local trauma experts are weary of the limitations of generalizing European studies to North America when other aspects of trauma management affect outcomes and prognosis
See this link for a journal club review of a 2012 study published in CMAJ on WBCT
Bottom Line: Recent Evidence Immediate WBCT vs. Selective Imaging
The evidence is conflicting on whether immediate WBCT is superior to selective imaging. The best quality evidence suggests no mortality benefit, however significant limitations hinder its generalizability.
Summary: Immediate WBCT in Blunt Trauma
- Conclusions from retrospective and registry data comparing immediate WBCT with selective imaging are limited by confounders and ISS inflation.
- Some evidence suggests that an immediate WBCT strategy could decrease time in the ED.
- The best available evidence, in the form of an RCT, does not support a mortality benefit from immediate WBCT, however its generalizability and validity have major limitations to be considered.
- Selective imaging can have the potential to significantly decrease radiation dose – the extent of this benefit is uncertain.
- Selective imaging does not equate to not performing an immediate WBCT, but rather using clinical factors in deciding the optimal imaging required for patients.
References
- Parachute. The Cost of Injury in Canada. Parachute. Public Health Agency of Canada. Toronto.
- Como J, Diaz J, Dunham, et al. Practice Management Guidelines for Identification of Cervical Spine Injuries Following Trauma. The Journal of Trauma. 2009; 67.
- Holmes J, and Akkinepalli R. Computed Tomography Versus Plain Radiography to Screen for Cervical Spine Injury: A Meta Analysis. The Journal of Trauma. 2005.
- Stiell I, Clement C, O’Connor A, et al. Multicentre prospective validation of use of the Canadian C-Spine Rule by triage nurses in the emergency department. CMAJ. 2010; 182.
- Sierink J, van Lieshout W, Beenen L, et al. Systematic review of flexion/extension radiography of the cervical spine in trauma patients. European Journal of Radiology. 2013; 82.
- Oh J, Asha S, and Curtis K. Diagnostic accuracy of flexion-extension radiography for the detection of ligamentous cervical spine injury following a normal cervical spine computed tomography. Emergency Medicine Australasia. 2016; 28.
- Malholtra A, Wu X, Kalra V, et al. Utility of MRI for cervical spine clearance after blunt traumatic injury: a meta analysis. Emergency Radiology. 2017; 27.
- Resnick S, Inaba K, Karamanos E, et al. Clinical relevance of magnetic resonance imaging in cervical spine clearance. JAMA Surgery. 2014; 149.
- Inaba K, Byerly S, Bush L, et al. Cervical spinal clearance: a prospective Western Trauma Association Multi-Institutional Trial. The Journal of Trauma and Acute Care Surgery. 2016; 81.
- Huber-Wagner S, Kanz K, Hanschen M, et al. Whole-body computed tomography in severely injured patients. Current Opinion in Critical Care. 2018; 24.
- Beatty L, Furey E, Daniels C, et al. Radiation exposure from CT scanning in the resuscitative phase of trauma care. CJEM. 2015; 17.
- Long B, April M, Summers S, and Koyfman A. Whole body CT versus selective radiological imaging strategy in trauma: an evidence-based clinical review. AJEM. 2017; 35.
- Chidambaram S, Goh E, and Khan M. A meta-analysis of the efficacy of whole-body computed tomography imaging in the management of trauma and injury. Injury. 2017; 48.
- Sierink J, Treskes K, Edwards M, et al. Immediate total-body CT scanning versus conventional imaging and selective CT scanning in patients with severe trauma (REACT-2): a randomised controlled trial. The Lancet. 2016; 388.

