

According to the AHA guidelines, in 2016 the annual incidence of out-of-hospital cardiac arrest (OHCA) in the US was roughly 360,000 and was 209,000 for in-hospital cardiac arrest. In Canada, we see 40,000 OHCA per year (Mozaffarian 2016).
- Data from the ROC Epistry confirms survival to hospital discharge in 2014 after non-traumatic EMS-treated cardiac arrest with any first recorded rhythm was 12% for patients of any age.
- This number may not seem great, but survival was 10.4% in 2010 and 8.2% in 2006.
- Survival increases to 38.6% in bystander-witnessed ventricular fibrillation (VF) arrest.
We are obviously doing something right, with extensive cardiac arrest research and refinements to the guidelines playing a major role.
Despite these encouraging numbers, many emergency providers are still faced with a significant sense of futility when it comes to the management of cardiac arrest. At times, we find ourselves simply going through the motions when managing these patients, when we should be leaders in the field of resuscitation medicine.
My objectives for this post are to provide evidence for controversial and cutting-edge topics, and ways in which we can improve the care of cardiac arrest patients in the ED, beyond what is outlined in the guidelines.
Minimizing interruptions in chest compressions

The best evidence we have for interventions that improve outcomes in cardiac arrest surround high-quality CPR:
- Chest compressions at a rate of 100-120/min with a depth of 5-6 cm and maximum chest recoil (Link 2015)
- The updated guidelines emphasize maximizing compression time, with improved rates of ROSC and survival to hospital discharge with chest compression fractions of at least 60% (Vaillancourt 2011).
In order to minimize interruptions in chest compressions:
- Use quantitative end-tidal capnography:
- ETCO2 correlates with measured cardiac output during resuscitation, and can be used both to judge the effectiveness of resuscitative attempts and as a marker of ROSC.
- A rapid rise in ETCO2 may be a better marker for ROSC than the pulse check, and does not require interruption in compressions.
- Anticipatory charging of the defibrillator:
- To maximize efficiency, ask the record-keeper to announce when there are 30 seconds to the next rhythm check.
- The defibrillator can be charged to 200J and ready to deliver a shock as soon as VF/VT is identified.
- If the rhythm is not shockable, the charge can be dumped.
- Patients with shorter pre- and peri-shock pauses have higher odds of survival (Cheskes 2014).
- An alternative to this is the use of “see-through CPR” machines, able to filter out compression artefact.
- Careful use of the advanced airway:
- There is some emerging evidence that airway management in the first 15 minutes of cardiac arrest may be associated with a decrease in rates of survival to discharge (Andersen 2017).
- This signal was amplified in patients who had an initial shockable rhythm, leading to the hypothesis that it is due to a delay in defibrillation.
- In primary cardiac arrest, consider avoiding early intubation if a patient can be ventilated adequately with a bag-valve mask.
Check out these links for more information on chest compressions during cardiac arrest:
- Mechanical vs manual chest compressions for OHCA
- What is optimal chest compression depth during OHCA resuscitation of adult patients
- Mechanical chest compressions and simultaneous defibrillation vs conventional CPR in OHCA
- Trial of continuous vs. interrupted compressions during CPR
Effective use of PoCUS in cardiac arrest
In the updated guidelines, the use of point-of-care ultrasound has been recommended as a highly sensitive and specific tool for real-time confirmation of endotracheal tube placement. PoCUS is also being used to guide chest compressions real-time, and in lieu of pulse checks in some centres, given the reportedly dismal accuracy of 78% (Tibballs 2009). However, transthoracic ultrasound can be challenging in cardiac arrest given subcutaneous air from chest compression trauma and the patient’s body habitus – image acquisition may not always fall within the guideline-recommended 10 second maximum for interruption of compressions.
A recent study examines the potential harms of PoCUS in cardiac arrest (Huis in’t Veld 2017):
- The authors found that the use of ultrasound nearly doubled the duration of pulse checks in cardiac arrest, with a mean time of 21 seconds.
- This study reinforces that PoCUS is not a harmless tool; in order to use it efficiently, there should be a focused clinical question and deliberate practice.
- Ultrasound in cardiac arrest should be used to identify reversible etiologies and considered in prognostication.
Prognostication
The absence of spontaneous cardiac activity on ultrasound is strongly associated with poor outcomes, with a negative likelihood ratio of 0.06 for survival (Tsou 2017). This information can then be integrated with other variables in the clinical picture for decision-making surrounding termination of resuscitation.
See also this 2012 paper by Blyth et al.
Reversible causes
PoCUS should be used methodically in cardiac arrest, seeking to identify classic “ultrasound signatures” of potentially reversible etiologies, such as cardiac tamponade, pneumothorax, pulmonary embolism, and hypovolemia (Tsou 2017). In the REASON trial (Gaspari 2016), patients found to have pericardial effusion or signs of pulmonary embolism on PoCUS had significantly higher rates of survival to hospital discharge.
Several ultrasound algorithms have been described (ie RUSH, EGLS); none have been shown to outrank the others, but all underscore the importance of a structured approach for efficient use of resuscitative ultrasound in cardiac arrest to answer a focused question. Simulation can be useful to practice fitting image generation into the resuscitation (Olszynski 2016). The sonographer should be set up in the subcostal position prior to pause for rhythm analysis, loop record videos, and analyze while someone else resumes compressions. Another alternative that doesn’t require holding compressions is the use of transesophageal echocardiography, a tool gaining traction in the ED.
High quality chest compressions with minimal interruptions is the first priority in cardiac arrest management. Resuscitative ultrasound has the potential for harm when used incorrectly, but is a useful tool when applied effectively, with the purpose of answering a focused clinical question.
See this post by Dr. Rajiv Thavanathan for further information on PoCUS (specifically ECHO) in cardiac arrest.
A novel approach to PEA management
- Traditionally, the management of pulseless electrical activity arrest revolves around high-quality CPR and identification of reversible causes.
- The “H’s & T’s” are still taught and memorized by ACLS providers, but can be difficult to remember in the heat of the moment.
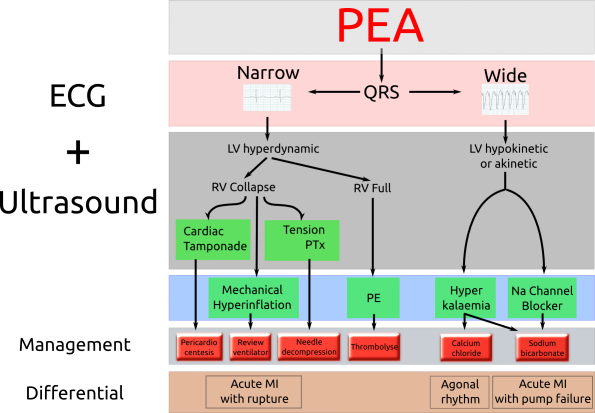
http://adelaideemergencyphysicians.com/2014/08/a-new-pea-diagnostic-algorithm-ecg-and-ultrasound/
- A simplified approach published in 2014 (Littman) helps to refine the DDx based on width of the QRS.
- A narrow QRS is more likely to be due to a mechanical problem
- Most commonly: hypovolemia, cardiac tamponade, tension pneumothorax, and pulmonary embolism
- These etiologies can be identified by PoCUS
- A wide QRS is more likely to be due to a metabolic cause
- Focus on: hyperkalemia and sodium-channel blocker toxicity
- Management is medical, with calcium and bicarbonate
- A narrow QRS is more likely to be due to a mechanical problem
New data is emerging that supports separating out a different set of patients from PEA arrest, those with “pseudo-PEA” vs. true electromechanical dissociation.
- “Pseudo-PEA”
- Occurs in a severe shock state, with such profound hypotension that peripheral pulses may not be palpable
- But, the basic physiology of the cardiac contraction remains intact
- Gaspari 2017
- Secondary analysis of the REASON data
- Found that patients in PEA arrest with cardiac activity on PoCUS who received vasopressors were 8 times more likely to have ROSC
- These patients were also much more likely to survive to hospital discharge (Flato 2015)
We should therefore use the tools at our disposal (PoCUS, invasive blood pressure monitoring with arterial lines) to identify this subset of patients and treat them accordingly with a norepinephrine infusion while identifying reversible etiologies.
Refractory VF/VT

Cardiac arrest survival in individuals with a shockable rhythm is approximately 30%, compared with 2-10% for asystole and PEA. This number can increase to 60% with high quality CPR in the setting of a strong coordinated system of care. Refractory VF, or VF storm, is defined as VF resistant to at least 3 defibrillation attempts, 3 mg of epinephrine, and 300 mg of amiodarone. Electrical storm can be frustrating for emergency providers to treat, given what we know about the potential for good outcomes. Evidence for the management of this condition is evolving, with some innovative options presented here:
- Dual-sequential defibrillation (DSD):
- The addition of a second set of pads and defibrillator ensures a second vector through the heart.
- Evidence for DSD is sparse and mostly retrospective (Cortez 2016), but shows survival to hospital discharge with good neurologic outcomes.
- Beta-blockers:
- Refractory VF is exacerbated by high levels of catecholamines, both endogenous and exogenous.
- Epinephrine administered during cardiac arrest management may be harmful through activation of beta-1 myocardial receptors, which increase oxygen demand and lower the VF threshold.
- The administration of selective beta-blockers, such as esmolol, has been shown to increase survival to hospital discharge with good neurologic outcomes (Driver 2014, Lee 2016).
- Esmolol is ideal given its beta-1 selectivity, rapidity of onset, and short duration of action.
- ECMO:
- Evidence for survival benefit with good neurologic outcomes comes out of Melbourne and Minnesota (Stub 2015, Yannopoulos 2016), with a protocol for ECMO that involved pre-hospital services and ED cannulation.
- These protocols require buy-in from the hospital’s intensivists, cardiac surgeons, and pre-hospital systems with careful selection of appropriate patients.
Conclusions
Cardiac arrest care is protocolized in ACLS for universal access, simplified for those who rarely run codes. As consultants specializing in Emergency Medicine, we should be on the forefront of resuscitation management, using cutting edge technologies and research to advance the field and save lives. That includes minimizing interruptions in chest compressions, using point-of-care ultrasound wisely and effectively; integrating interpretation of the QRS and ultrasound into the management of pulseless electrical activity; and the consideration of dual-sequential defibrillation, selective beta-blockers, and ECMO for the treatment of refractory ventricular fibrillation.
References
- Andersen LW et al. Association between tracheal intubation during adult in-hospital cardiac arrest and survival. JAMA. 2017. 317(5):494-506.
- Cheskes S et al. The impact of peri-shock pause on survival from out-of-hospital shockable cardiac arrest during the Resuscitation Outcomes Consortium PRIMED trial. Resuscitation. 2014. 85:336-342.
- Cheskes S et al. Chest compression fraction: a time dependent variable of survival in shockable out-of-hospital cardiac arrest. Resuscitation. 2015. 97:129-135.
- Cortez E et al. Use of double sequential external defibrillation for refractory ventricular fibrillation during out-of-hospital cardiac arrest. 2016. 108:82-6.
- Cunningham LM et al. Cardiopulmonary resuscitation for cardiac arrest: the importance of uninterrupted chest compressions in cardiac arrest resuscitation. Am J Emerg Med. 2012. 30:1630-8
- Driver BE et al. Use of esmolol after failure of standard cardiopulmonary resuscitation to treat patients with refractory ventricular fibrillation. Resuscitation. 2014. 85:1337-1341.
- Flato UAP et al. Echocardiography for prognostication during the resuscitation of intensive care unit patients with non-shockable rhythm cardiac arrest. Resuscitation. 2015. 92:1-6.
- Gaspari R et al. Emergency department point-of-care ultrasound in out-of-hospital and in-ED cardiac arrest. Resuscitation. 2016. 109:33-9.
- Gaspari R et al. A retrospective study of pulseless electrical activity, bedside ultrasound identifies interventions during resuscitation associated with improved survival to hospital admission. Resuscitation. 2017 (in press).
- Huis in’t Veld MA et al. Ultrasound use during cardiopulmonary resuscitation is associated with delays in chest compressions. Resuscitation. 2017. 119:95-8
- Lanctot JF, Valois M & Beaulieu Y. EGLS: echo-guided life support. Crit Ultrasound J. 2011. 3:123-9
- Lee YH et al. Refractory ventricular fibrillation treated with esmolol. Resuscitation. 2016. 107:150-5.
- Link MS et al. Part 7: adult advanced cardiovascular life support: 2015 American Heart Association guidelines update for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2015; 132(18 Suppl 2):S444-64
- Littman L, Bustin DJ & Haley MW. A simplified and structured teaching tool for the evaluation and management of pulseless electrical activity. Medical Principles and Practice. 2014. 23:1-6.
- Mozaffarian D et al. Heart Disease and Stroke Statistics – 2016 Update. Circulation. 2016.133:e38-e360
- Olszynski PA et al. Ultrasound during critical care simulation: a randomized crossover study. CJEM. 2016. 18(3):183-190.
- Rea T et al. The relationship between chest compression fraction and outcome from ventricular fibrillation arrests in prolonged resuscitations. Resuscitation. 2014. 85:879-884.
- Stub D et al. Refractory cardiac arrest treated with mechanical CPR, hypothermia, ECMO and early reperfusion (the CHEER trial). Resuscitation. 2015. 86:88-94.
- Tibballs J & Russell P. Reliability of pulse palpation by healthcare personnel to diagnose pediatric cardiac arrest. Resuscitation. 2009. 80(1): 61-4.
- Tsou P-Y et al. Accuracy of point-of-care focused echocardiography in predicting outcome of resuscitation in cardiac arrest patients: A systematic review and meta-analysis. Resuscitation. 2017. 114:92-99.
- Vaillancourt C et al. The impact of increased chest compression fraction on return of spontaneous circulation for out-of-hospital cardiac arrest patients not in ventricular fibrillation. Resuscitation. 2011. 82:1501-7.
- Yannopoulos D et al. Minnesota Resuscitation Consortium’s advanced perfusion and reperfusion cardiac life support strategy for out-of-hospital refractory ventricular fibrillation. J Am H Assoc. 2016. 5(6).

