
A healthy patient presents to the Emergency Department (ED) where you are working one night. He complains of a four-day history of progressively worsening fatigue, constant and diffuse headache, neck stiffness, fever, chills and night sweats. There was no associated photophobia or phonophobia. He denies any infective symptoms, sick contacts or recent travel. He denies any past medical or surgical history and is up to date on all his vaccinations.
On initial examination, his vitals are as follows: BP 108/53, HR 73, RR 14, SpO2 99% and temperature 36.6 C. He appears lethargic and confused. His neck is supple with no signs of meningismus. His skin is well perfused with no signs of mottling. The rest of his neurological, cardiac, respiratory, and abdominal examinations are normal.
Bloodwork and a lumbar puncture are performed and the patient is given a litre of normal saline. The patient’s care was handed over to the next emergency physician on shift with a presumed diagnosis of meningitis vs an influenza-like illness. The plan at this stage was to discharge the patient home if his lumbar puncture was negative.
His bloodwork returned showing:
- WBC = 17.7
- Neutrophils: 15
- Lactate 2
- Normal urinalysis and normal chest x-ray.
- His lumbar puncture showed no red blood cells and only 1 white blood cell with a normal protein and glucose count.
On re-assessment, the patient appeared obviously diaphoretic with rigors. He remained alert but not oriented to person, place or time with a GCS of 11. His repeat vitals are as follows: BP 94/50, HR 150, RR 13, SpO2 99% and temperature of 38.4 C.
What is your differential diagnosis?
-
Distributive shock
- Sepsis: Most likely cause in our patient, the etiology needs to be elicited further
- Neurogenic shock: Consider CNS or Spine trauma
- Anaphylaxis
- Endocrinologic: Thyroid storm, adrenal crisis
- Toxicologic: Sympathomimetic, serotonin syndrome, etc.
-
Hypovolemic shock
- Consider hemorrhage or fluid loss
-
Left ventricular failure/Cardiogenic shock
- Left ventricular systolic dysfunction, such as acute ACS
- Acute mitral or aortic regurgitation
- Left ventricular outflow tract obstruction
-
Right ventricular failure
- Pulmonary embolism
- Right ventricular myocardial infarction
-
Obstructive shock
- Pericardial tamponade
- Tension pneumothorax
- High airway pressures
The most likely diagnosis in our patient is a distributive shock from sepsis, for a deeper dive on appropriate and nuanced management of sepsis, see previous posts here and here.
Case Progression
An ED PoCUS was performed which showed a hyperdynamic heart contracting at a rate of approximately 150 beats per minute with a large mitral valve vegetation. He had no stigmata of infective endocarditis. At this stage, a third blood culture was sent, broad-spectrum antibiotics were initiated and a cardiology comprehensive echo and CT head were requested.


Revisiting the RUSH exam
The Rapid Ultrasound for Shock and Hypotension (RUSH) exam was originally described by Weingart et al. 2006 with the goal of creating a rapid method of using ultrasound to evaluate medically shocked patients.
The components of the exam can be recalled with the mnemonic: HI-MAP:
- Heart
- IVC
- Morison’s pouch
- Aorta
- Pulmonary
In our case, cardiology performed a transthoracic echo (TTE) demonstrating a moderate-sized vegetation on the posterior mitral valve associated with a valve perforation and mild to moderate mitral valve regurgitation. He was subsequently admitted to Cardiology following a comprehensive TTE.
A transesophageal echo (TEE) showed a large vegetation on the posterior leaflet, and a smaller vegetation on the anterior leaflet of his mitral valve with moderate to severe mitral regurgitation. A brain MRI showed multiple areas of restricted diffusion in both hemispheres and cerebellar hemispheres consistent with acute ischemia of embolic origin. Additionally, he also suffered emboli to both his kidneys and legs.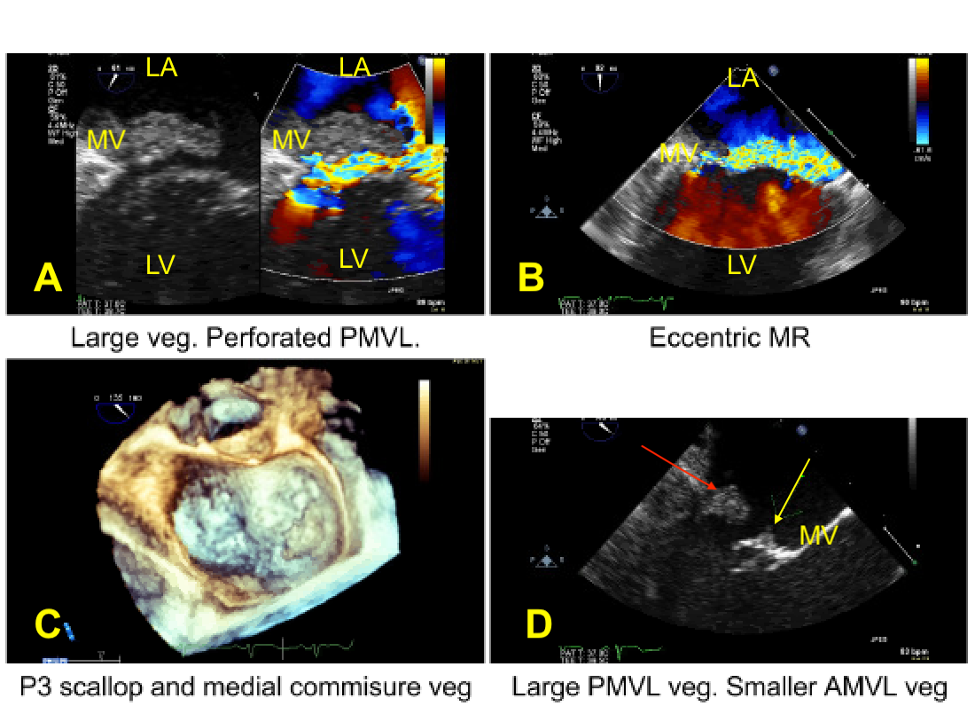
The above images represent the comprehensive TEE. Panel A shows a vegetation on the mitral valve with regurgitation along the posterior leaflet. Panel B shows flow in both directions, however, there is significant regurgitation, as the jet almost takes up 50% of the area, classifying this as moderate-severe regurgitation. Panel C shows the vegetation on the medial commissure. Panel D shows two vegetations, a large posterior MV vegetation (red arrow) and smaller anterior MV vegetation (yellow arrow).
Infective Endocarditis
Early diagnosis and treatment of infective endocarditis (IE) plays a significant role in clinical outcomes. In-hospital mortality rates for IE are as high as 40%. Most patients with endocarditis have risk factors such as; a predisposing valvular abnormality including rheumatic heart disease, mitral valve prolapse, calcific or degenerative aortic and mitral valves, IV drug use, or the presence of endovascular hardware such as prosthetic valves or pacemakers. IE can involve either the left or right side of the heart. Both present with fever, non-specific influenza-like-illness and shock. Left-sided endocarditis can present with acute heart failure, and septic emboli to the brain and body. Right-sided IE can present with septic pulmonary emboli.
There are three echocardiographic findings that are considered to be Duke major criteria for Endocarditis:
- Presence of vegetations; defined as mobile echo dense masses implanted in a valve or mural endocardium in the trajectory of a regurgitating jet or implanted prosthetic material
- Presence of abscess
- Presence of a new dehiscence of a valvular prosthesis
Additionally, on point of care ultrasound, the valve may appear thickened and regurgitation may be appreciated on colour Doppler.
Suggested PoCUS Approach to Assess Valve Abnormalities
- Assessment of valve form
- What does the valve look like?
- Are there areas of calcification?
- Are there areas of thickening?
- Assess the annulus to the leaflet tip?
- Is there a mass?
- What does the valve look like?
- Assessment of valve function
- How does the valve move?
- Is there normal excursion?
- Is there appropriate valve coaptation?
- Is there severe regurgitation?
- Add color Doppler to the valve of interest and to the area where you expect to see regurgitation.
- If the regurgitant jet fills more than 50% of the area (i.e., LA for MR or Aortic Outflow Tract for AV) then consider the possibility of severe regurgitation.
- How does the valve move?
It is important to note that PoCUS is not a replacement for a comprehensive echocardiogram and clinical judgment
Discussion
This case highlights the utility of PoCUS in the medically undifferentiated shock patient. There is rapidly expanding evidence that shows that PoCUS aids in the diagnosis and management of this patient population. As shown in our case, the use of ED PoCUS changed the management of our patient. It allowed us to rapidly diagnose IE in a patient with no risk factors and initiate treatment early on in a disease with large morbidity and mortality, which may have otherwise had a poor clinical outcome. PoCUS is a high impact diagnostic ED tool that should be routinely used in the undifferentiated febrile patient.
Note that all patient information has been changed to protect patient confidentiality, and the following post has been vetted by the Ottawa Hospital Privacy Officer.
References
Oxborough, D. (2008). A practical approach to transthoracic echocardiography. British Journal or Cardiac Nursing. 3. 163. 10.12968/bjca.2008.3.4.28922.
Weingart, S. https://emcrit.org/rush-exam/


