

Anti-racism is not easy topic to think about. In fact, it’s pretty uncomfortable. As you read this, it’s important to lean into that discomfort and reflect on why you’re feeling that way. Sometimes thinking about equity can leave us feeling unsure of how it applies to our work context and what actions we can take. This post will relate anti-racism to the Emergency Department (ED) context and have example actionable items. Anti-racism in the ED involves looking at Bias and Systemic Racism.
Disclaimer: The goal of this post is to help us grow as emergency healthcare providers and try to improve our patient care. This post will focus on bias and systemic racism, with examples focusing on OHCA, analgesia and COVID-19. It is absolutely not all inclusive. There are many aspects of anti-racism that this post does not touch upon, this does not mean they’re not important, just that the information can be found through other sources.
Bias in the ED
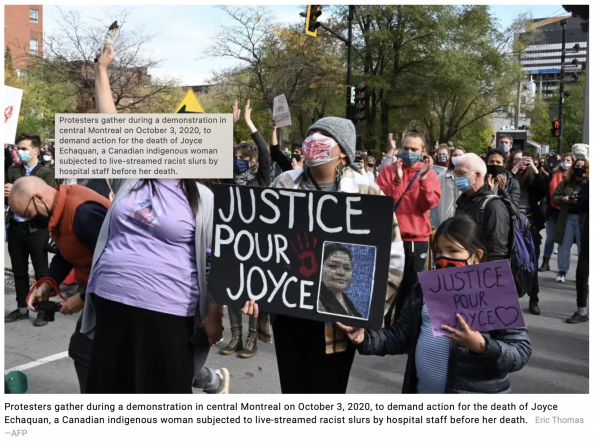
The horrific story of Joyce Echaquan in August of 2020 shocked all of us. She was an indigenous woman that was a 37year old mother of seven children. She was admitted to a Canadian hospital for “stomach pains”. During her stay, she felt consistently neglected and filmed and exposed the healthcare workers saying derogatory and racist comments about her. She died that night, and the cause of her death is still unclear.
This is Explicit Bias in action. Bias is how you think about, conceptualize and categorize a group of people in your mind. Explicit bias is when individuals are aware of their prejudice towards a group. So overt racism and clearly racist comments are examples of explicit bias. As emergency providers, we can’t tolerate this if we see it. We have an obligation to our patients and to each other to call this out if we see it. Explicit Bias is still a problem in Canada.
In contrast, Implicit Bias involves all of the subconscious feelings, perceptions, attitudes, and stereotypes that have developed as a result of prior life experiences and social influences. It is this automatic positive or negative preference for a group, based on our subconscious thoughts. With implicit bias, we may be unaware that its biases and not facts, are driving our decision-making.
The clearest example of implicit bias in the Emergency Department is the story of Brian Sinclair.1 His case shows us just how dangerous implicit biases in the ED can be. The healthcare providers ignored and tried to explain away a disabled, seemingly impoverished person of colour, without inquiring into the actual circumstances of his care. The fact that someone like that blends into our landscape to the point where they could literally die in the waiting room, just screams implicit bias. Ask yourself if this could have happened in your ED?

Implicit biases are much more pronounced in situations where people are stressed, fatigued, have competing demands, and have insufficient time or limited information…you have likely experienced many or all of these things during your last emerg shift.2 Our place of work is a perfect storm for implicit biases. In emergency medicine, we need to be fast, and efficient and the only way we can actually achieve that is by making quick associations based on our patient’s characteristics. The problem with implicit bias is that we come to rely on it so much in our work, and while it allows us to be fast, it often has a negative effect on the marginalized patients like Brian Sinclair, and on other people of colour. It is a double-edged sword.
So what’s the answer in acute care? Well, it’s not so easy as just ignoring all of our biases. We can’t just stop our biases from influencing us by sheer force of will. The nature of implicit biases is that they occur unconsciously and so they occur without us knowing. We need to reframe our expectations to acknowledge that we all have biases that we bring in to work.3
It’s not about preventing us from having biases, but about recognizing the bias and preventing it from leading to discrimination and having a negative effect on our marginalized patients. If we don’t start thinking about our implicit biases because of someone’s skin colour, then we’re saying that it’s ok that our biases are hurting our patients. When we prescribe a medication and it leads to iatrogenic injury – we reflect on that and try to avoid it happening again. Well, you can think of it the same way with implicit biases – our implicit biases are hurting our patients and lead to iatrogenic injury, and so we need to reflect on our biases to mitigate the damage.
So how do we recognize when we are being biased by someone’s skin colour, and how do we stop it from influencing patient care negatively? The evidence points to perspective taking as one of the options that can help mitigate implicit bias. A proposed framework to use this is in the PAUSE framework.4 The pause framework, is a proposed tool that you can use on your next shift.
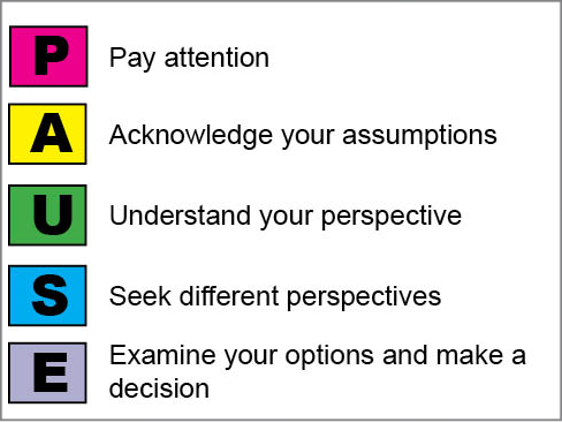
- Use the PAUSE framework by first paying attention to key moments that may show bias – a key moment to use this is when you leave a patient’s room and are feeling some kind of strong emotion, for example being upset or frustrated. Think about moments when you are feeling a lot of countertransference – this likely signifies that you’re relying on implicit biases. Another time to use this is before you see a patient, and in your mind you say the word “probably”… “they’re probably drunk, they’re probably drug-seeking”…the word probably is my personal cue to use this.
- The next step is to acknowledge the assumption you’re making. Then you need understand your own perspective and what prompted you to make that assumption. Force yourself to then seek a different perspective – this is where you consider a different way of thinking and viewing that person. A key part of this is empathizing with the patient and trying to share their perspective and see their point of view. The last step is to examine your options and make a decision. This PAUSE framework is like any other cognitive forcing strategy. Everyone has to find what works for them, but this is one possible option.
Actionable Item: Start reflecting on your implicit biases and how it might be negatively influencing your racialized patients. Use the PAUSE framework on your next emerg shift to reflect on and mitigate your implicit bias.
Systemic Racism in the ED
Systemic racism captures the idea that institutions like medicine are set up in a way so as to disadvantage a group of people. We often focus on this concept of systemic racism by looking at those who are disadvantaged, but it is critical to recognize that while the system disadvantages one group, it provides unearned advantages to another group. A good way to understand this is to look at the coin metaphor.5
The coin itself is a metaphor for a system of inequality – racism in this case. Those at the bottom of the coin are those we are oppressing by imposing a series of disadvantages that are unearned and undeserved. The flip side, and the top of the coin is privilege – this is the group of people that have a set of unearned advantages. In North American society, the coin is set up so that our white patients see the privilege, while those patients who are not white are oppressed. We can’t dismantle systemic racism by only focusing on those who are oppressed, it is equally important to recognize that while we are oppressing one group, we are giving privilege to another group…they’re two sides of the same coin
As you look at each of these coins as inequalities, there will be some in which you are oppressed in – where you will be very aware of the unearned oppression you experience. Then there will be inequalities that you have privilege in that you may be blind to. Each of these systems of inequalities can be considered their own coin, but importantly, they all intersect in profound ways. Multiple marginalized identifiers may have a determinantal effect that is larger than the sum of any of these composite parts – Brian Sinclair was a disabled, person of colour who was impoverished, and each of these systems of inequalities intersect with one another to provide a far greater stigma than any one alone. The intersectional nature of these inequalities should remain in the back of our minds because racism is just one piece of the puzzle.
Although we often think of medicine as “pure”, it has been a vehicle for systemic racism. In the 1920’s the Tuskegee Syphilis experiments involved doctors blatantly lying to black Americans and withholding treatment for Syphilis just to see what happened. In Canada, there is a history of doctors forcing sterilization on indigenous women as part of eugenics program to purge the indigenous population. Medicine is not innocent. The brutalization and dominance of these people has reverberated through time and still affects their descendants today – from food insecurity, to poverty, to education to housing. Moreover, it has led to many visible minority groups being suspicious and fearful of our medical system due to our history of abuse of mistreatment.
Examples in the ED
The amount of health disparities due to racism is staggering.6 We’re going to focus on two as examples in the ED: OHCA and analgesia.
Out of Hospital Cardiac Arrests (OHCA)
One of the clearest studies we have is the Shah 2014 paper from the USA.7 It was a systematic review and meta-analysis of 15 studies, most of these were cohort studies. The bottom line was that patients of colour were less likely to obtain ROSC in comparison to white patients. The odds ratio was a staggering 0.59 for ROSC in black patients compared to white patients. It gets worse, Black patients less likely to receive bystander CPR (OR 0.66), witnessed arrest (OR 0.77), inital VF/VT rhythm (OR 0.66) This isn’t limited to black patients, Hispanic and Asian patients were also less likely to obtain ROSC compared to white patients
Why is there such a discrepancy in bystander CPR and other OHCA metrics? Well part of it may be implicit bias – people may have a bias against non-white people, and thus be less inclined to perform CPR. A larger factor though is likely systemic: the neighbourhoods people live in, the education they have access to, the resources allocated to their neighbourhoods. It’s multifactorial. The brunt of a history of racism may have led to minorities either having less easy access to CPR training, or live in areas that don’t have AED’s, or having poorer health because racism has led to negative SDOH.
But clearly this is a symptom of a problem that is so large and wide scoping, all the rationale listed such as poverty, food insecurity, housing are not things that we can change easily as emerg docs. We can advocate of course, but we rely on politicians and policy makers to influence things like poverty and housing.
So, how can we as emergency physicians make any systems level change regarding racism? We have to remember that we can still affect the system at our emergency department level. Many of you sit on committees which can drastically influence our patient care.
Actionable item: It is important to leverage your position on committees to consider race inequalities and how improvements can be made, you can then liase with your local EDI committee about this and build partnerships with affected community members.
Analgesia
There is a discrepancy in analgesia prescriptions between white and non-white patients in the ED. A recent paper demonstrating this Goyal et al.8 This was a cross sectional retrospective study of pediatric patients with long bone fractures that presented to seven ED. They looked at 21069 visits of ED’s that were part of the PECARN network. Minority children were less likely to receive opiods (OR 0.86) or achieve optimal pain reduction (OR 0.80) compared to white patients. These discrepancies are starting out the moment patients even enter the healthcare system.
In the ED, a group of patients that is often racialized and needs analgesia is in our sickle population. Sickle cell societies have long recognized the role of implicit bias and structural racism that impacts our willingness to prescribe aggressive analgesia to this patient population.9 Their recommendation is to adopt SCD specific pain protocols because that standardizes care and reduces the impact of your bias.
Actionable Item: One small way to reduce your racial bias is to use the sickle cell protocol on your next shift. This concept can be translated to other painful conditions like renal colic. This is just one small step – it doesn’t solve the problem. However, thinking about racism can sometimes leave us feeling overwhelmed by the scope of the problem. If you’re feeling that way, this is one step you can take as an individual provider on your next emerg shift.
Anti-Racism in the ED
The crux of anti-racism involves understanding that both our implicit bias and systemic racism work and compound on each other to create health disparities. It is a dangerous cycle where systemic inequalities produce inequitable outcomes that then reinforce our harmful stereotypes about people of colour which is then use to justify inequitable systemic practices.
Change in our ED’s starts by recognizing how we all have implicit biases and how they negatively influence marginalized people in our busy ED environment. It then involves recognizing systemic racism as a 2 sided coin where one group has privilege and another group is oppressed. If there is one thing to take away, it is that we all need incorporate reflection as part of our daily practice in order to reflect on our biases and inequitable practices.
At the end of the articles we’re including a couple reflections from our own staff on what Black History Month has meant to them with the hopes of normalizing a diversity of experiences while encouraging you to reflect honestly and non-judgmentally on your own memories knowing every year is another opportunity to learn and grow a little more.
During BHM, I think about the jokes or critiques about BHM I’ve heard since early adulthood. Valid critiques about how it’s the shortest month of the year, but also not valid “critiques” like “how come there’s no white history month?” when… every month is white history month. I think the celebration of black people / history makes white people uncomfortable because it makes us acknowledge the systemic racism that is STILL prevalent today, and the privileges and disadvantages we all have simply based on our skin colour. – Rachel
With regards to BHM – I didn’t even know it existed until my teen years, and even then, it was only from watching television. Can something fall short if it never fell at all? I echo Barb’s sentiments – trying to listen, learn, and do better. – Jenn
Yes, as a kid at home we read about and talked about Malcolm X, Martin Luther King Jr, we sang the works of Fanny Crosby. We read about Mandela and Desmond Tutu. All that despite the factthere were no Black people where I grew up and BHM in Canada started in the late 70’s. The realities of race up close were French/English/Italian and Garden River vs Batchewana Indian bands. And no matter what one identified as, I don’t think I knew anyone not related though extended family to all of those categoriesWait… the McAuley family Who owned the only hotel were descendants of people who came on the Underground Railroad but they had intermarried with everyone else as well, by the 1950’sSo…to be honest the very first time I ever saw Black People around Haviland Bay was not until they were actually my own family. And in truth to this day, I think the only Black people around Haviland Bay are my own family.As for BHM now… it’s great… but living breathing family itself has been a bigger teacher of Black experience globally and in Canada – Christine
References:
- Allan B, Smylie J. First Peoples, Second Class Treatment | Wellesley Institute. Wellesley Inst. Published online 2015:1-71. http://www.wellesleyinstitute.com/?s=Allen+B.+SMylie+J%0Ahttp://www.wellesleyinstitute.com/publications/first-peoples-second-class-treatment/
- Ryn M van. Protecting Yourself and Your Patients from Implicit Biases. Published online 2012:117-122. doi:10.1016/b978-0-240-82155-9.00020-5
- Sukhera. Bias in the Mirror.; 2018. doi:10.26481/dis.20181129js
- Ross HJ. Everyday Bias. Rowman & Littlefield Publisher; 2014 .
- Nixon SA. The coin model of privilege and critical allyship: Implications for health. BMC Public Health. 2019;19(1):1-13. doi:10.1186/s12889-019-7884-9
- Owens A, Holroyd BR, Mclane P. Patient race, ethnicity, and care in the emergency department: A scoping review. Can J Emerg Med. 2020;22(2):245-253. doi:10.1017/cem.2019.458
- Shah KS, Shah AS, Bhopal R. Systematic review and meta-analysis of out-of-hospital cardiac arrest and race or ethnicity: Black US populations fare worse. Eur J Prev Cardiol. 2014;21(5):619-638. doi:10.1177/2047487312451815
- Goyal MK, Johnson TJ, Chamberlain JM, et al. Racial and ethnic differences in emergency department pain management of children with fractures. Pediatrics. 2020;145(5). doi:10.1542/PEDS.2019-3370
- Power-Hays A, McGann PT. When Actions Speak Louder Than Words — Racism and Sickle Cell Disease. N Engl J Med. 2020;383(20):1902-1903. doi:10.1056/nejmp2022125
