
Clinical case:
You are working an urgent care shift and your next patient to see is Jessica, a 35 yo female with an upper extremity injury. The one-liner on the EMR reads: ‘Jesse’. When you go to speak with them, you see a young masculine-presenting patient who appears pale and diaphoretic. You introduce yourself and your personal pronouns, and learn that your patient goes by Jesse and uses the pronouns he/him.
Jesse tells you that he has been having severe shoulder pain that radiates to the back and jaw for about one hour. The pain came on as he was playing golf with a friend, and it has persisted since. He did not injure himself nor do any heavy lifting, and the pain is not worse with movement. The pain did not go away when he sat down, nor when he took Tylenol. He also feels sweaty and anxious, with no nausea, shortness of breath, or presyncope. He has never had pain like this before. He is otherwise healthy, though his family doctor has recently told him that he has high cholesterol. He has no family history of heart disease. He smokes 1 pack of cigarettes daily, drinks alcohol socially, and uses cannabis occasionally.
Jesse’s only medications are buproprion XR 300mg daily and testosterone undecanoate IM 1000mg every month. His testosterone is prescribed by an endocrinologist who is following him throughout his transition. Jesse tells you that he was assigned-female-at-birth (AFAB), and identifies as a transgender (trans) man. As such, he has been getting monthly testosterone injections for the past 11 months.
His vitals are as follows: BP 110/60, HR 66, RR 20, T 36.6, O2 sat 94%. Cardiac and respiratory exams are unremarkable. Jesse asks you if he could be having a heart attack. You think that his story sounds highly suspicious, and you are not sure of the effects that testosterone has on cardiac risk. You order a stat troponin and ECG.
Question:
Are transgender and gender-diverse (TGD) persons on testosterone at a higher risk for acute coronary syndrome (ACS)?
Evidence:
There is very little literature on the topic of TGD persons who take testosterone with regards to cardiovascular risk. We know that the FDA has previously issued a warning for testosterone taken for hypogonadism in cisgender (cis) men as it may increase the risk of myocardial infarction.1,2 This warning has been controversial as some subsequent studies have been discordant.3 However, patients who take testosterone as gender-affirming hormone therapy (GAHT) generally take at minimum two-fold higher doses in the first year of treatment, and may be subject to even higher risks.4
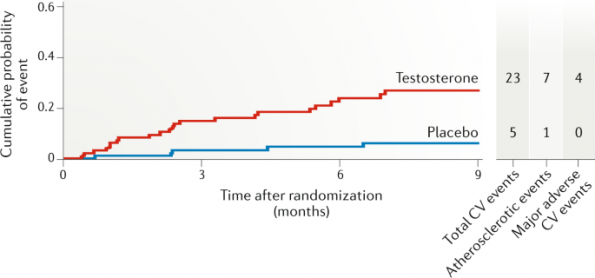
Figure 1 | Gagliano-Jucá, T., Basaria, S. Testosterone replacement therapy and cardiovascular risk. Nat Rev Cardiol 16, 555–574 (2019). https://doi.org/10.1038/s41569-019-0211-4.
One study published in 2019 found that trans men are at a four-fold higher risk of MI than cis women, and a two-fold higher risk of MI than cis men.5 Possible mechanisms of increased cardiovascular risk for trans men taking GAHT include increases in blood pressure, insulin resistance, changes in lipid profiles (most notably decreases in HDL, increases in triglycerides and LDL), and increased BMI.6,7 We do know that TGD persons are at higher risk for venous thromboembolism.
Some other considerations:
- Ethinyl estradiol, an oral estrogen formulation which has largely fallen out of use, is associated with an increased risk of cardiovascular events in trans women. The same has not been shown to be true for other formulations.8
- Trans people experience significantly greater rates of depression, anxiety, and other mental health conditions.9 Poor mental health is known to be correlated with increased cardiovascular risk, further impacting the cardiac health of transgender people.10
- TGD people are burdened with significantly higher psychosocial stress related to increased violence, stigma, and interpersonal and institutional discrimination.11 Chronic stress is associated with a higher risk of cardiovascular disease.12
- Trans people have higher rates of substance use, including smoking.11,13 Smoking is a well-established cardiovascular risk factor.
- Although understudied, some studies show that trans youth are less likely to participate in physical education class and regular physical activity. This can be in part attributed to feeling misunderstood uncomfortable in environments where students are segregated by gender.14 Studies also show lower rates of physical activity in trans adults compared to cis adults.15
- There is currently no guidance on whether clinicians should use sex recorded at birth or affirmed gender when risk stratifying and using risk calculators.16 Notably, it seems unlikely that any TGD participants were included in the derivation and validating of scores like HEART, TIMI, etc.
- Inquiries in multiple settings have identified that trans persons avoid emergency departments out of fear for discrimination, being misgendered or dead-named, medical violence, or dismissal.
Case continued:
Jesse’s ECG shows new diffuse T wave inversions and his troponin comes back elevated. You subsequently diagnose him with NSTEACS, transfer him to an area of your ED with cardiac monitoring. You begin treatment with nitro spray, ASA, clopidogrel, and unfractionated heparin, and you urgently consult cardiology to come see Jesse.
References:
- Research C for DE and. FDA Drug Safety Communication: FDA cautions about using testosterone products for low testosterone due to aging; requires labeling change to inform of possible increased risk of heart attack and stroke with use. FDA. Published online September 2, 2019. Accessed November 30, 2021. https://www.fda.gov/drugs/drug-safety-and-availability/fda-drug-safety-communication-fda-cautions-about-using-testosterone-products-low-testosterone-due
- Finkle WD, Greenland S, Ridgeway GK, et al. Increased Risk of Non-Fatal Myocardial Infarction Following Testosterone Therapy Prescription in Men. PLOS ONE. 2014;9(1):e85805. doi:10.1371/journal.pone.0085805
- Haddad RM, Kennedy CC, Caples SM, et al. Testosterone and cardiovascular risk in men: a systematic review and meta-analysis of randomized placebo-controlled trials. Mayo Clin Proc. 2007;82(1):29-39. doi:10.4065/82.1.29
- Petering RC, Brooks NA. Testosterone Therapy: Review of Clinical Applications. AFP. 2017;96(7):441-449.
- Alzahrani T, Nguyen T, Ryan A, et al. Cardiovascular Disease Risk Factors and Myocardial Infarction in the Transgender Population. Circulation: Cardiovascular Quality and Outcomes. 2019;12(4):e005597. doi:10.1161/CIRCOUTCOMES.119.005597
- Streed CG, Harfouch O, Marvel F, Blumenthal RS, Martin SS, Mukherjee M. Cardiovascular disease among transgender adults receiving hormone therapy: A narrative review. Annals of Internal Medicine. 2017;167(4):256-267. doi:10.7326/M17-0577
- Streed CGJ, Beach LB, Caceres BA, et al. Assessing and Addressing Cardiovascular Health in People Who Are Transgender and Gender Diverse: A Scientific Statement From the American Heart Association. Circulation. 2021;(daw, 0147763):CIR0000000000001003. doi:10.1161/CIR.0000000000001003
- Gooren LJ, Wierckx K, Giltay EJ. Cardiovascular disease in transsexual persons treated with cross-sex hormones: reversal of the traditional sex difference in cardiovascular disease pattern. Eur J Endocrinol. 2014;170(6):809-819. doi:10.1530/EJE-14-0011
- Reisner SL, Poteat T, Keatley J, et al. Global health burden and needs of transgender populations: a review. The Lancet. 2016;388(10042):412-436. doi:10.1016/S0140-6736(16)00684-X
- Khawaja IS, Westermeyer JJ, Gajwani P, Feinstein RE. Depression and Coronary Artery Disease. Psychiatry (Edgmont). 2009;6(1):38-51.
- Parent MC, Arriaga AS, Gobble T, Wille L. Stress and substance use among sexual and gender minority individuals across the lifespan. Neurobiology of Stress. 2019;10:100146. doi:10.1016/j.ynstr.2018.100146
- Lagraauw HM, Kuiper J, Bot I. Acute and chronic psychological stress as risk factors for cardiovascular disease: Insights gained from epidemiological, clinical and experimental studies. Brain Behav Immun. 2015;50:18-30. doi:10.1016/j.bbi.2015.08.007
- Kcomt L, Evans-Polce RJ, Veliz PT, Boyd CJ, McCabe SE. Use of Cigarettes and E-Cigarettes/Vaping Among Transgender People: Results From the 2015 U.S. Transgender Survey. Am J Prev Med. 2020;59(4):538-547. doi:10.1016/j.amepre.2020.03.027
- Bishop A, Overcash F, McGuire J, Reicks M. Diet and Physical Activity Behaviors Among Adolescent Transgender Students: School Survey Results. J Adolesc Health. 2020;66(4):484-490. doi:10.1016/j.jadohealth.2019.10.026
- Downing JM, Przedworski JM. Health of Transgender Adults in the U.S., 2014-2016. Am J Prev Med. 2018;55(3):336-344. doi:10.1016/j.amepre.2018.04.045
- Denby KJ, Cho L, Toljan K, Patil M, Ferrando CA. Assessment of Cardiovascular Risk in Transgender Patients Presenting for Gender-Affirming Care. The American Journal of Medicine. 2021;134(8):1002-1008. doi:10.1016/j.amjmed.2021.02.031

