

Drowning accounts for over 360,000 worldwide deaths annually, including the deaths of hundreds of Canadians.[1],[2] Despite this, accurate drowning statistics remain obscured by significant under-reporting.[1]
As an emergency physician you will see drowning patients in your ED. Surveying our local Ottawa group, 48% of resident and staff respondents said they’ve seen a drowning patient in the ED. Notably, even more respondents identified seeing a drowning when the definition was clarified.
In this high-yield post, I’ll untangle confusing terms you may have seen surrounding drowning and provide you local data. In part 1, we will review drowning pathophysiology as it relates to historical and current management as a physician first-responder on the pre-hospital setting. Part 2 of this series will focus on management as a resuscitation team lead, urgent care clinician management of the secondary drowning and a broad review of wilderness medicine survival strategies specific to high-risk drowning scenarios that could one day save your life.
Content breakdown:
_________
Definitions
The following drowning definitions are outdated:[3]
-
- Near-drowning
- Secondary drowning
- Dry drowning
- Wet drowning
- Freshwater drowning
- Saltwater drowning
Why? These terms were confusing and lacked a physiologic basis. For example, research shows no pathophysiologic or mortality difference between fresh and salt-water drowning.[4],[5]
The World Health Organization (WHO) operationalized drowning as “the process of experiencing respiratory impairment from submersion or immersion in liquid”.[3] This definition isn’t new – it was published almost twenty years ago in 2004.
Drowning can be further split into fatal or non-fatal drowning. If there wasn’t a fatal outcome, that’s a non-fatal drowning. The 30-minute drowning resuscitation with ROSC is a non-fatal drowning. The twelve-year old who choked on hot-tub water is a non-fatal drowning.
Appropriately diagnosing drowning is critical to improve patient care. For example, if the twelve-year-old above is discharged as “choking” or “aspiration”, this patient becomes missed in drowning statistics. Ultimately, what isn’t identified as a drowning case can’t be researched further to optimize care. In Canada, the Drowning Prevention Research Centre leads research on epidemiology and prevention, and diagnostic misclassification creates a barrier to accurate data collection.[1]
Canadian Data
Approximately 460 Canadians die of drowning each year, and more suffer non-fatal drowning incidents resulting in long-term consequences. Locally in Ontario, we average over 150 deaths annually.[1]
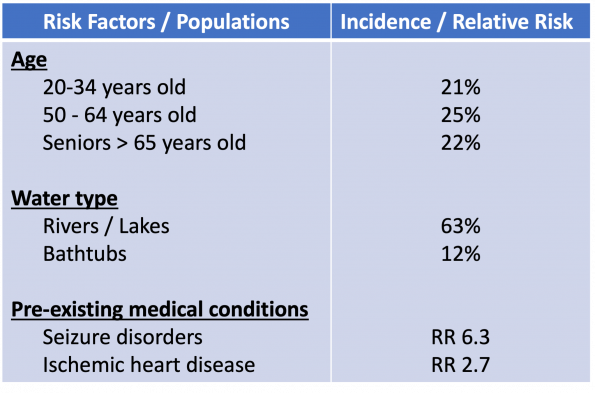 Of fatal drownings, the highest rates are among men 50 to 64 years-old (25%), seniors 65 years and older (22%), and young adults 20 to 34 years of age (21%).[1] Deaths are most likely to occur between May to September, on weekends, and in natural bodies of waters such as rivers or lakes (63%). Furthermore, drownings in bathtubs are also common at around 12% of cases.
Of fatal drownings, the highest rates are among men 50 to 64 years-old (25%), seniors 65 years and older (22%), and young adults 20 to 34 years of age (21%).[1] Deaths are most likely to occur between May to September, on weekends, and in natural bodies of waters such as rivers or lakes (63%). Furthermore, drownings in bathtubs are also common at around 12% of cases.
A recent publication on fatal Canadian drownings found over one-third had a pre-existing medical condition, including seizure disorders (RR=6.3) and ischemic heart disease (RR=2.7).[6]
Now how many drowning patients present to an emergency room? A lot more.
A myth is that drowning is often fatal, and a minority present to care.
The truth is that on average, for every 1 child that dies of drowning, another 8 will receive care in an ED (USA).[7] In Ontario, we average 543 ED visits annually for drowning and 95 hospitalizations, although the true incidence is likely higher given non-fatal drowning diagnostic misclassification.[1]
Drowning Pathophysiology

To best appreciate the physiology of drowning, try the following exercise. Take a deep breath in and hold it while reading through the following two paragraphs, picturing yourself in open water. On average, this will take between 30-45-seconds: enough to safely feel air hunger.
Drowning starts with a period of panic as you’re unable to breath in, and your body surges with catecholamines.[2] Perhaps you’re struggling to stay above the water, or you’re completely submerged. Your arterial CO2 levels are slowly rising telling your brain to breathe in, but this initial urge can be overridden. Research studies found the average breath-hold breaking point in healthy subjects to be 49 seconds.[8] Kate Winslet in Avatar 2 reportedly held her breath for seven minutes and 15 seconds, but let’s not try to beat this extreme.
Eventually, you have an involuntary gasp and inspiratory effort. This leads to water aspiration which triggers an involuntary coughing reflex upon tracheal impact. Within the lungs, you begin to wash out pulmonary surfactant. This rapidly causes profound changes in your gas exchange and lung compliance, leading to atelectasis, inflammation, and non-cardiogenic pulmonary edema. Simultaneously you attempt to clear your airway by swallowing water, but this leads only to gastric distension and emesis. Eventually, hypoxia occurs leading to a loss of consciousness, but this can take minutes. A cardiac arrest from hypoxia subsequently occurs, noting this is preceded by bradycardia and pulseless electrical activity (PEA) rather than a ventricular dysrhythmia.[9],[10]
Now breathe in.
Historical Drowning Treatments
With your refreshed knowledge on drowning physiology, let’s dive into debunked historical drowning treatments.
In 1839, one of the first published articles on drowning treatment was published in the Lancet by Dr. Hancock. He describes the concept of exsugation, defined by sucking strongly on the nostrils of a drowning patient to revive them. Thankfully this never caught on.[11]
Fast-forward to the 1980s, the Heimlich maneuver entered into practice for choking victims. Soon after, Henry Heimlich and Edward Patrick touted the maneuver as effective in drowning victims.[12],[13] However, this was largely speculative and lacked clinical evidence. In fact, it contributed to delays in oxygenation with increased rates of emesis and airway contamination.[14],[15] It was ultimately denounced by the American Heart Association and Institute of Medicine as an ineffective drowning treatment.
Pre-Hospital Drowning Care
We spend more time by water each year than consciously appreciated. Excluding home bathtubs, your local leisure center, and even your tropical beach vacation, reflect briefly on how many times each year you encounter water outdoors by a pond, river, lake? Perhaps an outdoor skating rink, or a backyard canal? Multiply that by a lifetime, and it’s easy to see your chance of encountering first-response drowning care to a drowning victim is quite high.
I’m not advocating that you perform in-water rescues outside of your scope of training – that’s dangerous. However, just you can be called upon as doctor on board of a plane for a medical emergency, you may just encounter a drowning victim. Below, there are three important steps you can take as a physician first-responder for a drowning victim.
1. Ventilation First Resuscitation
For the arrested drowning patient, begin with rescue breaths first, not chest compressions.
This is nuanced, and if you’d like a deeper dive into my rationale, click the drop-down link below.
Ventilation First Rationale
On first-glance, consensus-based expert guidelines appear to offer conflicting evidence.
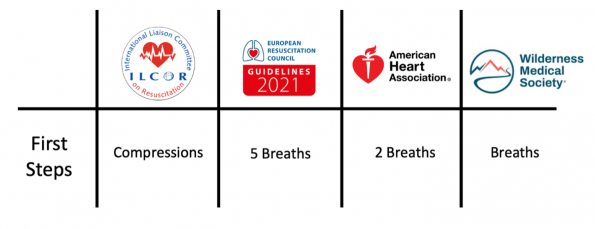
- The most recent International Liasson committee on Resuscitation (ILCOR) 2021 guidelines suggests “commencing CPR with compressions rather than ventilations.[16]
- The European Resuscitation Council (ERC) 2021 guidelines advise beginning with “5 rescue breaths using 100% inspired oxygen if available”.[17]
- The American Heart Association (AHA) guidelines state “deliver 2 rescue breaths first”.[18]
- The Wilderness Medicine Society highlights that “initial resuscitation should focus on establishing and maintaining a patent airway and providing oxygen.”[5]
Examining ILCOR’s compression recommendation, we can appreciate nuances within these guidelines. ILCOR published a recent systematic review on this topic involving five databases and 730 references. Briefly, 0 of the 730 studies met full-text PICO inclusion criteria comparing breath-first to compression-first ventilation in drowning victims.
In fact, an RCT comparing the two strategies will likely never be performed however, that being said, a decision needs to be made on what the best available evidence suggests. This indirect evidence comes from two sources: bystander-CPR and In-Water Resuscitation (IWR) studies.
In a 2021 Resuscitation review, three drowning studies were identified that compared conventional breath and compression CPR to compression-only CPR by bystanders.[19] All studies trended towards increased survival if breaths were provided, including one study finding a highly positive association between bystander ventilations and survival (OR = 6.7).[20] That review identified five studies examining IWR on patient outcomes.[19] IWR is defined as providing an unconscious drowning patient with rescue breaths while in the water prior to extrication. IWR does not involve in-water chest compressions which are conceivably impossible without a backboard.
Of the five studies, four were feasibility studies involving manikins limiting their real-world application. A single retrospective study in Brazil examined IWR in 86 unconscious, apneic patients.[21] The results of this study were impressive but marred by methodological flaws and selection biases.
The indirect studies outlined above all suggest a trend towards increased survival with early ventilations. Combined with our understanding of drowning pathophysiology contributing to a hypoxic arrest, I agree with the AHA, ERC, and Wilderness Medicine Society that a breath-first ventilation strategy is best.
On further clarifying ILCOR’s guidelines, they do state that “health care providers (HCP) and those with a duty to responding to drowning [lifeguards] consider providing rescue breaths first … if trained to do so.”[16] Speaking with Dr. Christian Vaillancourt of ILCOR, he highlighted that a common barrier to bystander CPR initiation is hesitancy to provide rescue breaths, and they want to maximize public engagement in resuscitations. For the non-healthcare trained bystander, initiating compressions first maintains simplicity as retains the same CPR sequence as that of non-drowning arrests. For you reading this, however, starting with breaths is highly recommended.
2. Call for an AED early, but don’t delay CPR
Shockable rhythms in drowning are uncommon. In a systematic review involving 12 studies and 14920 patients, a shockable rhythm in OHCA due to drowning was uncommon, reported range of VF/VT between 2-14%.[19]
This is where the story and witnesses become invaluable. Does this occur suddenly in an otherwise healthy 60-year-old ex-Olympian swimmer? Perhaps in that circumstance, there was an underlying primary cardiac event, so have a higher index of suspicion for shockable rhythm. However, typical drowning pathophysiology involves bradycardia into a PEA arrest.
You may be asking, can cold-water itself trigger a cardiac dysrhythmia and arrest? For example, over 70% of deaths during US triathlons occur during the swim phase of the race.[22] Rosen’s Emergency Medicine also describes immersion syndrome, which is “syncope from cardiac dysrhythmias on sudden contact with water that is at least five degrees lower than core temperature”.[23] The answer is: likely not.
It’s why we didn’t see thousands of deaths from the ALS Ice Bucket Challenge in 2014. Small case series have demonstrated cardiac arrythmias following cold-water immersion, but these are seldom dangerous ventricular arrythmias. Instead, they’re sinus tachycardias, bradycardias or PVCs.[24] For triathletes, there’s numerous proposed mechanisms behind deaths clustering in the swim-phase, the most intriguing being swimming induced pulmonary edema (SIPE).[22]
3. Consider PEEP and Recruitment Maneuvers
In our earlier review of drowning pathophysiology, we discussed pulmonary surfactant washout causing profound changes in gas exchange and lung compliance. Indeed, one article directly measured this directly in a sheep model.[25] Using anesthetized sheep, the researchers instilled either 1-3 ml/kg of fresh or salt-water intratracheally then measured lung compliance which ultimately decreased by 66% within 5-minutes of administration. Furthermore, work of breathing increased 5-9x and airway resistance increased 2-8x.
Now think about little-Bo-PEEP.
We can extrapolate our treatment for ARDS and similar disease states with high airway resistances to drowning.[26] Difficult BVM ventilation in drowning patients should be countered in the same way. If your pre-hospital BVM has a PEEP valve, use it if you’re encountering resistance to bagging. Further consider other pre-hospital recruitment maneuvers like head-up positioning and an assisted two-hand BVM technique.
Summary
Briefly, the take-home points for Part 1 are as follows:
- Drowning as defined by the WHO in 2004 is the process of experiencing respiratory impairment from submersion or immersion in liquid.
- Avoid outdated and irrelevant drowning terms such as secondary, near, dry, wet, freshwater and saltwater drowning.
- The pathophysiology involves washout of pulmonary surfactant, alveolitis, non-cardiogenic pulmonary edema, and hypoxia contributing to bradycardia into PEA arrest.
- In the pre-hospital setting:
- Ventilate (2-5 breaths) before compressions
- Call for an AED early but know that shockable rhythms are uncommon (2-14%)
- Consider PEEP and recruitment maneuvers for difficulty oxygenating
Now that we have covered the pathophysiology and pre-hospital management of these patients, in Part 2, we will dive into a review of in-hospital resuscitation in addition to prognostication and monitoring of non-fatal drownings in the ED.
References
[1] Drowning Prevention Research Centre, “Canada Drowning Prevention Plan (9th Edition),” 2022, doi: https://www.drowningresearch.ca/media/576/cdndrowningpreventionplan-en-9thedition-20220520.pdf.
[2] F. Salomez and J.-L. Vincent, “Drowning: a review of epidemiology, pathophysiology, treatment and prevention,” Resuscitation, vol. 63, no. 3, pp. 261–268, Dec. 2004, doi: 10.1016/j.resuscitation.2004.06.007.
[3] E. F. van Beeck, C. M. Branche, D. Szpilman, and J. H. Modell, “A new definition of drowning: towards documentation and prevention of a global public health problem,” Bull. World Health Organ., 2005.
[4] Conn, Alan W. MD FRCPCMiyasaka, Katsuyuki MDKatayama, Masao MDFujita, Michio PhDOrima, Hiromitsu PhDBarker, Geoffrey MB FFARACSBohn, Desmond MB FRCPC, “A canine study of cold water drowning in fresh versus salt water,” vol. 23, no. 12, pp. 2029–2037, 1995.
[5] A. C. Schmidt, J. R. Sempsrott, S. C. Hawkins, A. S. Arastu, T. A. Cushing, and P. S. Auerbach, “Wilderness Medical Society Clinical Practice Guidelines for the Treatment and Prevention of Drowning: 2019 Update,” Wilderness Environ. Med., vol. 30, no. 4, pp. S70–S86, Dec. 2019, doi: 10.1016/j.wem.2019.06.007.
[6] C. L. Dunne, J. Sweet, and T. Clemens, “The link between medical conditions and fatal drownings in Canada: a 10-year cross-sectional analysis,” Can. Med. Assoc. J., vol. 194, no. 18, pp. E637–E644, May 2022, doi: 10.1503/cmaj.211739.
[7] “Centers for Disease Control and Prevention: Water-related injuries facts.” [Online]. Available: www.cdc.gov/HomeandRecreationalSafety/Water-Safety/waterinjuries-factsheet.html
[8] N. Trembach and I. Zabolotskikh, “The Influence of Age on Interaction between Breath-Holding Test and Single-Breath Carbon Dioxide Test,” BioMed Res. Int., vol. 2017, pp. 1–5, 2017, doi: 10.1155/2017/1010289.
[9] B. Albert and Jr. Craig, “Causes of loss of consciousness during underwater swimming,” J. Appl. Physiol., vol. 16, no. 4, pp. 583–586, Jul. 1961, doi: 10.1152/jappl.1961.16.4.583.
[10] M. H. Wyckoff et al., “2021 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations: Summary From the Basic Life Support; Advanced Life Support; Neonatal Life Support; Education, Implementation, and Teams; First Aid Task Forces; and the COVID-19 Working Group,” Circulation, vol. 145, no. 9, Mar. 2022, doi: 10.1161/CIR.0000000000001017.
[11] Hancock, John, “Resuscitation from Drowning & From Asphyxiation by Gases,” Lancet, 1839.
[12] H. J. Heimlich, “Subdiaphragmatic pressure to expel water from the lungs of drowning persons,” Ann. Emerg. Med., vol. 10, no. 9, pp. 476–480, Sep. 1981, doi: 10.1016/S0196-0644(81)80281-8.
[13] H. J. Heimlich and E. A. Patrick, “Using the Heimlich maneuver to save near-drowning victims,” Postgrad. Med., vol. 84, no. 2, pp. 62–73, Aug. 1988, doi: 10.1080/00325481.1988.11700363.
[14] P. Rosen, M. Stoto, and J. Harley, “The use of the Heimlich maneuver in near drowning: Institute of medicine report,” J. Emerg. Med., vol. 13, no. 3, pp. 397–405, May 1995, doi: 10.1016/0736-4679(95)00022-3.
[15] D. Szpilman and P. J. Morgan, “Management for the Drowning Patient,” Chest, vol. 159, no. 4, pp. 1473–1483, Apr. 2021, doi: 10.1016/j.chest.2020.10.007.
[16] ILCOR Staff, “CAB or ABC in drowning: Basic Life Support Systematic Review,” 2022, [Online]. Available: https://costr.ilcor.org/document/cab-or-abc-in-drowning-bls-856-tf-systematic-review
[17] C. Lott et al., “European Resuscitation Council Guidelines 2021: Cardiac arrest in special circumstances,” Resuscitation, vol. 161, pp. 152–219, Apr. 2021, doi: 10.1016/j.resuscitation.2021.02.011.
[18] “Part 10.3: Drowning,” Circulation, vol. 112, no. 24_supplement, Dec. 2005, doi: 10.1161/CIRCULATIONAHA.105.166565.
[19] J. Bierens et al., “Resuscitation and emergency care in drowning: A scoping review,” Resuscitation, vol. 162, pp. 205–217, May 2021, doi: 10.1016/j.resuscitation.2021.01.033.
[20] H. Hubert et al., “Can we identify termination of resuscitation criteria in cardiac arrest due to drowning: results from the French national out-of-hospital cardiac arrest registry: Termination of resuscitation criteria in CAD,” J. Eval. Clin. Pract., vol. 22, no. 6, pp. 928–935, Dec. 2016, doi: 10.1111/jep.12562.
[21] D. Szpilman and M. Soares, “In-water resuscitation—is it worthwhile?,” Resuscitation, vol. 63, no. 1, pp. 25–31, Oct. 2004, doi: 10.1016/j.resuscitation.2004.03.017.
[22] R. E. Moon, S. D. Martina, D. F. Peacher, and W. E. Kraus, “Deaths in triathletes: immersion pulmonary oedema as a possible cause,” BMJ Open Sport Exerc. Med., vol. 2, no. 1, p. e000146, Aug. 2016, doi: 10.1136/bmjsem-2016-000146.
[23] R. M. Walls, Rosen’s Emergency Medicine Concepts and Clinical Practice (10th Edition). 2023.
[24] M. Tipton, P. Kelleher, and F. Golden, “Supraventricular arrhythmias following breath-hold submersions in cold water,” Undersea Amp Hyperb. Med. J. Undersea Hyperb. Med. Soc. Inc, vol. 21, no. 3, p. 305—313, Sep. 1994.
[25] H. J. H. Colebatch and D. F. J. Halmagyi, “Lung mechanics and resuscitation after fluid aspiration,” J. Appl. Physiol., vol. 16, no. 4, pp. 684–696, Jul. 1961, doi: 10.1152/jappl.1961.16.4.684.
[26] O. Thom, K. Roberts, S. Devine, P. A. Leggat, and R. C. Franklin, “Treatment of the lung injury of drowning: a systematic review,” Crit. Care, vol. 25, no. 1, p. 253, Dec. 2021, doi: 10.1186/s13054-021-03687-2.


Trackbacks/Pingbacks