

Introduction
Frostbite is a frequent presenting complaint to emergency departments (EDs) in cold climates. It is more common among those without housing, those with mental health disorders as well as those who work or engage in outdoor activities.(1) These injuries can be debilitating requiring surgical intervention, debridement or amputation in the most severe cases. Complications can include local swelling, necrosis, gangrene, compartment syndrome, contracture and other physical deformities.(1) The high level of morbidity associated to frostbite injuries highlights the importance of initial management in the emergency department which we will review in this post.
Pathophysiology
Frostbite is a freezing cold thermal injury that occurs when tissues are exposed to temperatures below their freezing point (approximately -0.53C).(1,2) Cold exposure then causes peripheral vasoconstriction with intermittent cycles of vasodilation. Direct cellular injury occurs due to ice crystal formation, cell dehydration and shrinkage as well as electrolyte and pH imbalances.(1–3) Once rewarming occurs, reperfusion injury cascade triggers the production of free radicals and inflammatory mediators, which then contribute to progressive dermal ischemia.(1–3)
Initial Patient Evaluation
Early recognition is essential to improving prognosis where paresthesia is often the first symptom of frostbite injury.(1,2) It is important to also ensure to evaluate the patient for any concurrent pathologies such as hypothermia, trauma or underlying cause of frostbite. Generally, the patient may describe feeling numb, cold and clumsy.(1,2) Overall, the appearance of affected tissue can be variable including yellow, pale or even mottled blue. Following rewarming, the tissues may appear red, edematous as well as have blister formation.(1,2)
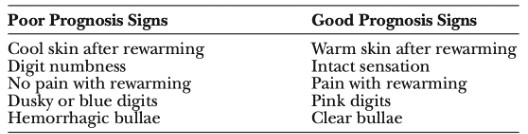
The purpose of this early assessment can help identify poor or good prognostic signs related to frostbite injury.
Table 1: Prognostic factors in frostbite injuries adapted from Gonzaga et al (4).
Classification
There have been several classification systems proposed for the grading of frostbite. Historically, frostbite was divided into “degrees” including frostnip and first-, second- and third-degree frostbite depending on the depth of the injury.(1,2) Frostnip is defined as the superficial non-freezing cold injury where there is no formation of ice crystals nor long-term tissue damage.(5)
However, the introduction of a newer classification by Cauchy and colleagues has been adopted by many centers as it gives an early prognostic factor of bone and tissue loss as well as a likely anatomic amputation level.(2,3,6) This classification further goes on to identify initial management (Table 2).
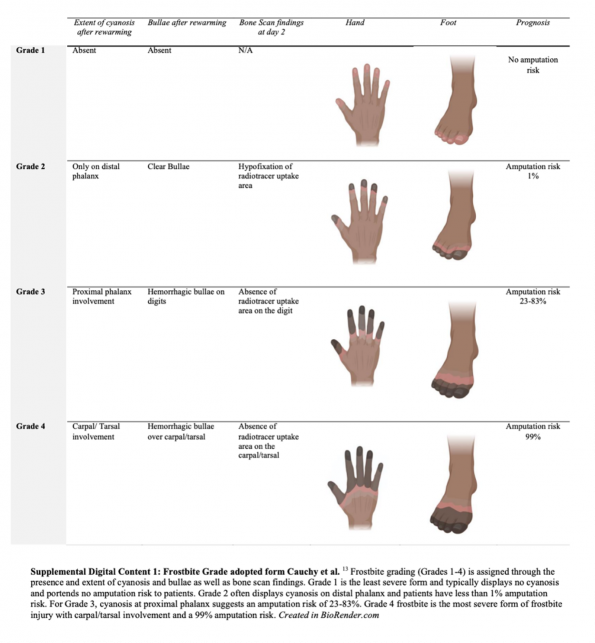
Figure 1: Supplemental image outlining the classification of frostbite adopted from Cauchy et al.
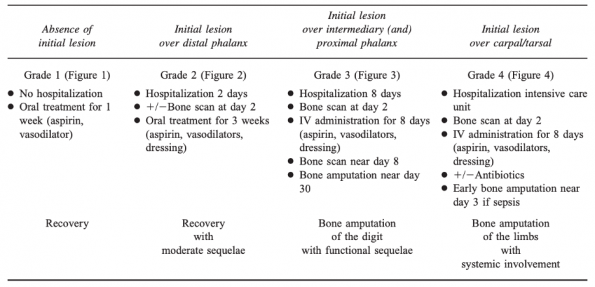
Table 2: Management of frostbite injuries at Day 0 per Cauchy and colleagues. Grading scheme following 1h rewarming in 38C bath, IV infusion of chlorohydrate buflomedil and 250mg aspirin (6).
Management in the Field
Initial assessment in the field should consist of traditional ABCDE (airway, breathing, circulation, disability, exposure) approach where primary first-aid and resuscitation takes precedence. Once this has been addressed and frostbite injury has been established, any wet and tight clothing should be removed.(1) Rubbing, massaging, applying dry heat as well as freeze-thaw-cycles must be avoided as this can cause further tissue damage.(1,2) As such, rewarming should be initiated in the field if it is likely that no further cold exposure will occur during transport. The affected area can also be wrapped in gauze and immobilized for comfort.(1,2) Once the patient has been stabilized, they should then be transported to the nearest medical facility for ongoing care.
Pre-Hospital Rewarming
If proper resources are available, and definitive care is more than 2 hours away, field rewarming should be done by warm water immersion.(2,5) This can be done by placing the affected extremity into warm water that is between 37-39°C. Ideally a thermometer should be used as the affected limb will have impaired temperature sensation. If this is not possible, then the unaffected limb or a caregiver’s / healthcare provider’s hand can be used to confirm that the water temperature is appropriate.(2,5) As an endpoint, rewarming is complete when the affected skin is red/purple and the tissues are pliable.(1,2) This same procedure can also be performed following arrival to an appropriate medical facility.
In the recently published 2023 American Burn association guidelines,(7) they pose the question regarding rewarming:
“Among adults with severe limb frostbite, does rapid rewarming in a 38°C to 42°C water bath compared to not using rapid rewarming in a 38°C to 42°C water bath result in a) fewer amputations and or b) more distal level of amputation.”
Interestingly, there is no compelling evidence of human studies; however, they do describe that in animal studies where extremities were exposed to extreme cold temperatures, rapid rewarming showed an advantage with less tissue loss when compared to spontaneous rewarming. Following these animal studies rapid rewarming was performed in humans and continues to be recommended based on expert consensus.
In-Hospital Management
Upon arrival to a medical facility, patients should be assessed in a systematic approach, with initial assessment of their ABCs. Given likely prolonged cold exposure in patients presenting with frostbite injuries, they should also be assessed for hypothermia. Recommendations from the Wilderness Medical Society (WMS) suggest that patients with mild hypothermia (35-32°C) should have concurrent treatment for hypothermia and frostbite.(5,8) Conversely, those with moderate (32-28°C) or severe (<28°C) hypothermia should be treated effectively for hypothermia prior to treatment of frostbite injury.(5,8) Warming of the affected extremity can be performed as described above in the pre-hospital warming section.
Management of frostbite injuries can be broken down as follows:
Analgesia
Unless there is a contraindication present, all patients should be started on a nonsteroidal anti-inflammatory drug such as ibuprofen. Its effect is thought to be two fold – analgesia as well as anti-inflammatory properties that reduce prostaglandins and thromboxanes.(1,2) There is no specific literature to confirm the exact benefits of this intervention, however, it continues to be recommended despite limited evidence.(1,2,5) The WMS recommends ibuprofen 12 mg/kg per day divided twice daily up to a maximum of 2400 mg/day.(5)
Tetanus
Routine standard tetanus toxoid guidelines should be followed as frostbite is not high risk for tetanus infection.(1–3)
Antibiotics
If there is evidence of infection, antibiotics should be provided and can be guided by skin swab results. There is limited evidence regarding prophylactic antibiotics for frostbite. In a retrospective study from 1993, Valnicek and colleagues report no difference in the incidence of wound infectious with the use or oral or intravenous antibiotics for prophylaxis.(9) Some practitioners recommend prophylactic antibiotics if there is edematous tissue, malnutrition, immunosuppression or a large surface of frostbite. There is no evidence to support this recommendation and it is highly practice specific.(2,5)
Debridement of blisters
WMS guidelines recommend drainage of clear blisters by aspiration with the rationale that these blisters contain prostaglandins and thromboxanes that can damage underlying tissue.(1,2,5) It is recommended that hemorrhagic blisters remain untouched. Overall, there is limited evidence to support this recommendation.
In discussion with Dr. Brent Trull, one of our local Ottawa plastic surgeons, he is in agreement with the WMS guidelines.
Aloe Vera
Aloe vera ointment has shown to improve outcomes through the reduction of prostaglandin and thromboxane production. WMS recommends application to thawed tissue before application of dressings.(5) WMS also recommends reapplication of aloe vera at each dressing change or every 6 hours. Interestingly, EM clinics of North America does not recommend application of aloe vera given that there is insufficient evidence.(2)
Imaging
Various imaging modalities have been recommended to assess the degree of vascular damage secondary to frostbite. As described by the WMS, patients can be considered for technetium pyrophosphate imaging (bone scan), magnetic resonance angiography (MRA), CT angiography, Doppler ultrasound as well as single photon emission computer tomography (SPECT).(5)
A retrospective observational cohort study from Finland in 2017, which followed the Helsinki frostbite management protocol, performed immediate angiography of the affected extremity in the setting of severe frostbite if there were no contraindications.(10) This was similar to a 2016 study by Gonzaga and colleagues where again angiography was used to determine extent of injury and guide subsequent treatment.(4) In their 2021 review, Gao and colleagues also describe that angiography can be helpful in patients who present less than 24 hours after frostbite injury without any contraindications to thrombolysis.(11) This test is readily available in the emergency department and should be considered in patients presenting with severe frostbite.
When patients present more than 24 hours following frostbite injury, bone scanning or MRA can be considered as these can offer prognostic information and guide management.(2,11) These tests are not readily available in the emergency department and would usually be ordered if patients are admitted.
Advanced In-Hospital Therapies
Thrombolytic Therapy
In treating frostbite injury, rapid rewarming addresses the ice crystal phase of cellular damage, but does not treat damage or thrombosis that may have already occurred in affected vessels.(12)
To investigate this, Twomey and colleagues performed an open label study in 2005 to investigate the safety and efficacy of tissue plasminogen activator (tPA) in the treatment of severe frostbite.(12) They administered tPA to all patients with severe frostbite that did not improve with rapid rewarming, had absent Doppler pulses in the distal limb or digits, without perfusion by technetium 99-m three-phase bone scan and no contraindication to tPA use. In this study, 19 patients with a total of 174 digits at risk of amputation were given intraarterial or intravenous tPA. Two patients had to have therapy stopped due to increased bleeding. In all, 16 of 19 patients responded to tPA treatment and this was one of the first studies demonstrating effective treatment with tPA and heparin for frostbite to prevent amputation.(12) They found this treatment was most effective in patients who had less than 24 hours of cold exposure, warm ischemia times less than 6 hours and no freeze-thaw cycles.(12)
Subsequently, in their retrospective review of clinical outcomes in 2007, Bruen and colleagues demonstrated that administration of tPA decreased the rate of digital amputation from 41% to 10% when administered within 24 hours of injury.(13) This was one of the first advances in the treatment of frostbite in over more than 25 years.
Click to read a more in-depth Expert Opinion on Thrombolytics…
In their retrospective review published in 2016, Gonzaga and colleagues looked at patients admitted to a regional burn center with frostbite from 1994 to 2007.(4) In this study, patients with severe frostbite without contraindications to fibrinolytics, underwent diagnostic angiography of the affected extremity. Patients found to have an abnormal angiogram with a perfusion defect were initiated with treatment with TNK, papaverine and IV unfractionated heparin. Repeat angiography was performed in 24 hours. If repeat angiography was normal, TNK was stopped while heparin was continued. If angiogram continued to be abnormal, the TNK infusion was continued. 114 patients were admitted for frostbite injuries, 69 patients underwent angiography and 66 patients received treatment with intra-arterial thrombolytic therapy. Complete vascular reperfusion after thrombolytics was demonstrated in about 2/3 of patients, which was associated with a 98% salvage rate. Overall 89% had at least a partial response with return of vascular flow beyond the next joint level for one or more digits.
In 2019, Drinane and colleagues performed a systematic review to determine if thrombolytic therapy is effective and to identify patients who may benefit from this treatment.(14) In total they found 42 studies that looked at 1842 limbs and digits in 325 patients. A total of 216 patients were treated with thrombolytics and 346 amputations were performed. TPA was most commonly administered intra-arterially. Limb salvage ranges from 0% to 100% with a weighted average of 78.7%. They conclude that thrombolytics are a safe and effective treatment of severe frostbite.
Lacey and colleagues assessed outcomes for patients admitted from 2014 to 2019 with frostbite following the institution of a protocol for the management of severe frostbite injury at their center.(15) They also performed a prospective observational study on a cohort of patients. Their management protocol included immediate rewarming, workup of patients with blood work, urine pregnancy test and a CT head. All patients without contraindication to thrombolytics and clinically diagnosed severe frostbite or positive technetium 99 bone scan are considered for intravenous thrombolytic therapy. After alteplase patients are started on therapeutic anticoagulation. Patients are also started on ibuprofen to help decrease inflammatory response. Gabapentin was started if neuropathic pain is present. ASA was also started to help minimize platelet aggregation on the healing endothelium. Salvage rate was 80.7% of at-risk tissue, however, this varied each year with a range from 57% to 92%. Since implementation of their protocol they also found a decrease in the ICU length of stay from 13 days in 2014 to 3.4 days in 2019 which was a statistically significant change.
An interesting study out of Colorado by Carmichael and colleagues, developed a protocol for the remote administration of tPA at referring hospitals prior to transfer to the tertiary referral center.(16) They subsequently did a retrospective review 5 years after implementation. Similar to previous studies, rewarming was performed, as well as full patient assessment including trauma workup if there was a suspicion of trauma or intoxication. The extremity is also assessed by Doppler when possible. TPA is administered in eligible patients (with third or fourth degree frostbite). Their study include 199 patients, of whom 40 received tPA therapy pretransfer, 32 received tPA on admission and 127 did not qualify for TPA. After controlling for confounders, they found that patients who received remote TPA had lower odds of any amputation compared to those receiving TPA at their center (OR 0.19 CI 0.05-0.65) and the group receiving no TPA (OR 0.14 0.05-0.4). Only one patient in the pre-transfer group (2.3%) has a significant bleeding event requiring transfusion. This study suggests that having a protocol in place with referral hospitals can decreased time to TPA and possibly decrease amputation.
Similar to when we think of stroke and myocardial infarction, Nygaard and colleagues studied if delay to thrombolytics had an impact on limb/digit salvage.(17) They included patients with perfusion defects shown on Tc-99m triple-phase bone scan in their retrospective review. 62% of patients in their study receive thrombolytic treatment. Compared to other studies they did not have a statistically significant difference in the TPA vs non TPA group for the percentage of patients requiring amputation or salvage rate. They did demonstrate in their analysis an additional 26.8% salvage loss with each hour of delayed treatment through regression analysis.
The American Burn Association just released Clinical Practice guidelines in April of this year and in their guidelines they have a conditional recommendation for thrombolytics.(7) From the studies they reviewed, there is a trend towards improved salvage with thrombolytic therapy both in terms of fewer amputations and a more distal level of amputations. In these guidelines they do not make a recommendation for intravenous vs intra-arterial TPA given insufficient evidence.
In discussion with one of local Ottawa plastic surgeons, Dr Brent Trull, he recommends having a low threshold to call plastic surgery to discuss possible thrombolysis for a patient who is presenting to the ED within 24 hours of rewarming.
Iloprost
Iloprost has been an emerging therapy for severe frostbite, first published in 1994.(18) Iloprost is a synthetic prostaglandin analogue that has been historically used for the treatment of pulmonary hypertension and acts by dilating systemic and pulmonary arteries and impairing platelet aggregation. It can also reduce capillary permeability, suppress platelet aggregation and activates fibrinolysis.(2)
These findings were subsequently followed by a randomized control trial performed by Cauchy and colleagues in 2011.(19) In this study, patients were randomized to one of three treatment regimens after receiving usual care of rewarming of affected part, 250mg Aspirin and 400mg intravenous buflomedil. One group received 250mg Aspirin and buflomedil (400mg for 1 hour per day), the second group received 250mg Aspirin plus prostacyclin (0.5-2 ng of iloprost per kg of body weight per minute for 6 hours per day) and the last group received 250mg of Aspirin, iloprost and fibrinolysis (100mg of recombinant tissue plasminogen activator for the first day only). Risk of amputation in the buflomedil group was 60% compared to 0% in the group receiving prostacyclin alone and 19% in the group receiving prostacyclin plus rt-TPA.(19) This is the only trial found in a 2020 systematic review investigating this question and it was deemed low quality evidence given small sample size, unclear risk of bias and use of buflomedil which has now been discontinued.(20) Buflomedil is an alpha-adrenolytic agent that was previously widely in Europe but is not currently approved in the United States or Canada.(5)
Poole and colleagues implemented the Yukon Frostbite Protocol in 2015 and subsequently reviewed charts of all patients who were treated as per the protocol between 2015 and 2020.(21) Using the grading system introduced by Cauchy and colleagues, grade 1-4 frostbite were managed with: daily hydrotherapy; debridement and aspiration of clear blisters; topical administration of aloe vera; regular ibuprofen; and pantoprazole. Patients with grade 2-4 frostbite received iloprost. Patients with grade 4 frostbite within 24 hours of rewarming also received alteplase. There were 22 patients enrolled in the study with 142 affected digits. All digits with grade 2 or 3 frostbite were salvaged, as were 50% of those with grade 4 frostbite. Four patients required amputation. All 29 digits amputated had grade 4 frostbite, the majority of digits (19) were from one patient. This study thus demonstrated a salvage rate of 100% for grade 2 or 3 frosbite and 50% for grade 4 frostbite. This is an improvement compared to other studies reporting the risk of amputation without iloprost or thrombolysis to be 31% for grade 2 frostbite, 67% for grade 3 frostbite and 98-100% for grade 4 frostbite.(6)
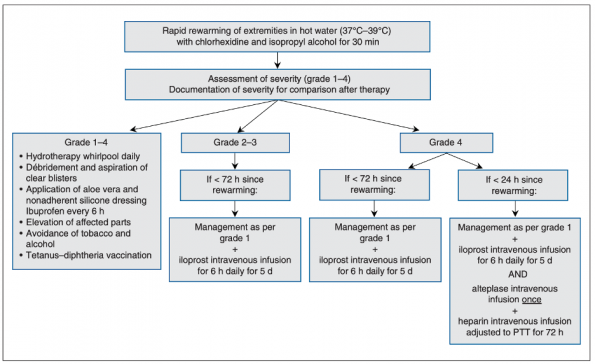
Figure 2: Management algorithm proposed with Iloprost based on degree of frostbite.
Interestingly, a recent 2022 study published by Crooks and colleagues from Calgary, assessed the effectiveness of a 5-day course of IV iloprost at reducing digital amputation for patients with severe frostbite injuries in an urban setting.(22) In this retrospective study, 90 patients were included where 26 were treated with iloprost and 64 patients received usual care. Frostbite grading was performed as per the classification system described by Cauchy and colleagues.(6) There were no digital amputations in patients with grade 2 frostbite. Lower digital amputation rates were observed for patients with more severe frostbite injuries treated with iloprost compared to usual care: Grade 3 (18% vs 44%, p < 0.001); grade 4 (46% vs 95%, p <0.001). This study did not show as significant benefit when compared to previous literature and perhaps this was related to the comorbidities of the patients included. Patients included in this study were from an urban cohort with significant medical and social comorbidities (52.4% unhoused in the standard care arm), while previous studies had looked at healthy mountaineers.(19,21)
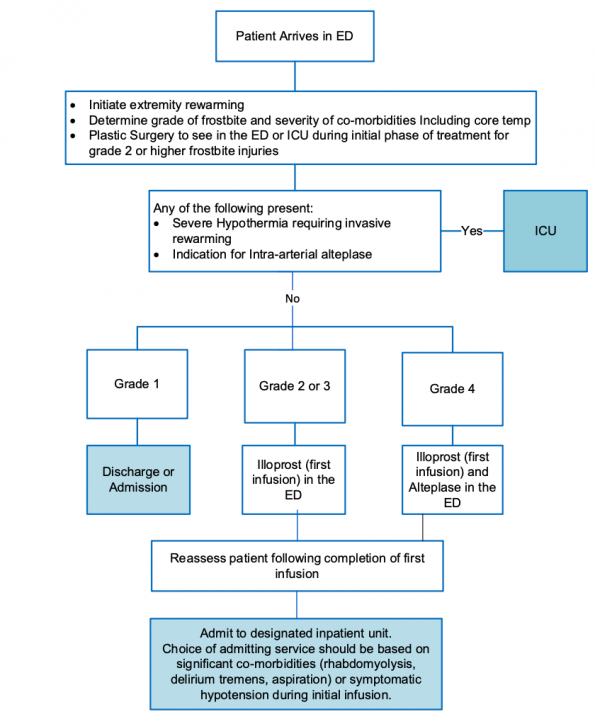
Figure 3: ED management of frostbite with Iloprost based on grade of injury curtesy of Dr. Crooks.
Hyperbaric Oxygen
Hyperbaric oxygen (HBO) has been used to aid in wound healing. It is thought that HBO may improve frostbite outcome by increasing the cellular oxygen availability to the damaged tissues. This can then help to mitigate the inflammatory cascade.(2,23)
From 2013 to 2019, Magnan and colleagues performed a multi-center prospective single-arm study where they compared patients in their prospective cohort who received early HBO in addition to standard care with iloprost.(23) They compared this to a historical cohort where patients received iloprost alone between 2000 and 2012. In this study they included patients with: grades 3 or 4 frostbite according to the Cauchy classification; initiation of medical care within 72 hours from frostbite injury; and, no contraindications to aspirin, iloprost or HBO. Standard treatment consisted of rewarming of frostbitten extremities for 60 min and 250mg ASA. Those with grade 3 or 4 frostbite then received the first iloprost infusion immediately and were hospitalized for 7 days. Those in the HBO group also received HBO daily in addition to the iloprost infusions. Technecium 99 bone scan was performed at day 3 and day 7. Patients were also follow up at 6 months and 1 year post treatment. The primary outcome of the study was the number of preserved segments at 12 months. Each phalanx and each metacarpal or metatarsal is defined as a segment. Their results demonstrated a higher number of preserved segments per patient in the prospective group with HBO treatment compared to the historical control (13 SD +/- 10 vs (6SD +/- 5). In the prospective cohort 57% of patients had three to four preserved segments compared to 13% in the control group (p<0.001).
Take Home Messages
- Assess extent of injury after 60 minutes of rewarming the extremity.
- For frostbite management:
- Follow routine tetanus guidelines;
- There is no evidence for prophylactic antibiotics;
- There is weak evidence for application of aloe vera;
- Consider debriding and / or aspirating clear blisters.
- In patients presenting up to 72 hours of injury with grade 2-4 frostbite consider calling your local plastic surgeon early. These patients may be eligible for limb salvage therapy with TPA / iloprost.
References
- Zaramo TZ, Green JK, Janis JE. Practical Review of the Current Management of Frostbite Injuries. Plastic and Reconstructive Surgery – Global Open. 2022 Oct 24;10(10):e4618.
- Handford C, Thomas O, Imray CHE. Frostbite. Emergency Medicine Clinics of North America. 2017 May;35(2):281–99.
- Sheridan RL, Goverman JM, Walker TG. Diagnosis and Treatment of Frostbite. Ingelfinger JR, editor. N Engl J Med. 2022 Jun 9;386(23):2213–20.
- Gonzaga T, Jenabzadeh K, Anderson CP, Mohr WJ, Endorf FW, Ahrenholz DH. Use of Intra-arterial Thrombolytic Therapy for Acute Treatment of Frostbite in 62 Patients with Review of Thrombolytic Therapy in Frostbite: Journal of Burn Care & Research. 2016;37(4):e323–34.
- McIntosh SE, Freer L, Grissom CK, Auerbach PS, Rodway GW, Cochran A, et al. Wilderness Medical Society Clinical Practice Guidelines for the Prevention and Treatment of Frostbite: 2019 Update. Wilderness & Environmental Medicine. 2019 Dec;30(4):S19–32.
- Cauchy E, Chetaille E, Marchand V, Marsigny B. Retrospective study of 70 cases of severe frostbite lesions: a proposed new classification scheme. Wilderness & Environmental Medicine. 2001 Dec;12(4):248–55.
- Wibbenmeyer L, Lacey AM, Endorf FW, Logsetty S, Wagner ALL, Gibson ALF, et al. American Burn Association Clinical Practice Guidelines on the Treatment of Severe Frostbite. Journal of Burn Care & Research. 2023 Apr 13;irad022.
- Dow J, Giesbrecht GG, Danzl DF, Brugger H, Sagalyn EB, Walpoth B, et al. Wilderness Medical Society Clinical Practice Guidelines for the Out-of-Hospital Evaluation and Treatment of Accidental Hypothermia: 2019 Update. Wilderness & Environmental Medicine. 2019 Dec;30(4):S47–69.
- Valnicek, Stan, Chasmar, Leslie, Calpson, J. Brian. Frostbite in the Prairies – A 12 Year Review. Plastic and Reconstructive Surgery – Global Open. 1993 Sep;92(4):633–41.
- Lindford A, Valtonen J, Hult M, Kavola H, Lappalainen K, Lassila R, et al. The evolution of the Helsinki frostbite management protocol. Burns. 2017 Nov;43(7):1455–63.
- Gao Y, Wang F, Zhou W, Pan S. Research progress in the pathogenic mechanisms and imaging of severe frostbite. European Journal of Radiology. 2021 Apr;137:109605.
- Twomey JA, Peltier GL, Zera RT. An Open-Label Study to Evaluate the Safety and Efficacy of Tissue Plasminogen Activator in Treatment of Severe Frostbite: The Journal of Trauma: Injury, Infection, and Critical Care. 2005 Dec;59(6):1350–5.
- Bruen KJ. Reduction of the Incidence of Amputation in Frostbite Injury With Thrombolytic Therapy. Arch Surg. 2007 Jun 1;142(6):546.
- Drinane J, Kotamarti VS, O’Connor C, Nair L, Divanyan A, Roth MZ, et al. Thrombolytic Salvage of Threatened Frostbitten Extremities and Digits: A Systematic Review. Journal of Burn Care & Research. 2019 Aug 14;40(5):541–9.
- Lacey AM, Rogers C, Endorf FW, Fey RM, Gayken JR, Schmitz KR, et al. An Institutional Protocol for the Treatment of Severe Frostbite Injury—A 6-Year Retrospective Analysis. Journal of Burn Care & Research. 2021 Aug 4;42(4):817–20.
- Carmichael H, Michel S, Smith TM, Duffy PS, Wiktor AJ, Lambert Wagner A. Remote Delivery of Thrombolytics Prior to Transfer to a Regional Burn Center for Tissue Salvage in Frostbite: A Single-center Experience of 199 Patients. Journal of Burn Care & Research. 2022 Jan 5;43(1):54–60.
- Nygaard RM, Lacey AM, Lemere A, Dole M, Gayken JR, Lambert Wagner AL, et al. Time Matters in Severe Frostbite: Assessment of Limb/Digit Salvage on the Individual Patient Level. Journal of Burn Care & Research. 2017;38(1):53–9.
- Groechenig, E. Treatment of Frostbite with Iloprost. October 1994. 344:1152–3.
- Cauchy E, Cheguillaume B, Chetaille E. A Controlled Trial of a Prostacyclin and rt-PA in the Treatment of Severe Frostbite. N Engl J Med. 2011 Jan 13;364(2):189–90.
- Lorentzen AK, Davis C, Penninga L. Interventions for frostbite injuries. Cochrane Injuries Group, editor. Cochrane Database of Systematic Reviews [Internet]. 2020 Dec 20 [cited 2023 Mar 26];2020(12). Available from: http://doi.wiley.com/10.1002/14651858.CD012980.pub2
- Poole A, Gauthier J, MacLennan M. Management of severe frostbite with iloprost, alteplase and heparin: a Yukon case series. cmajo. 2021 Apr;9(2):E585–91.
- Crooks S, Shaw BH, Andruchow JE, Lee CH, Walker I. Effectiveness of intravenous prostaglandin to reduce digital amputations from frostbite: an observational study. Can J Emerg Med. 2022 Sep;24(6):622–9.
- Magnan MA, Gayet-Ageron A, Louge P, Champly F, Joffre T, Lovis C, et al. Hyperbaric Oxygen Therapy with Iloprost Improves Digit Salvage in Severe Frostbite Compared to Iloprost Alone. Medicina. 2021 Nov 22;57(11):1284.

Management algorithms are very useful tools.