

Your patients need you to start rethinking what you know about pre-oxygenation. The peri-intubation period is a physiologically hazardous time; when we feel forced to act in critical situations, we often try to speed things up and cut corners. We hope to convince you, with an abundance of evidence, that taking the time to perfectly pre-oxygenate your patient is worthwhile and will dramatically improve patient outcomes, because mastering the basics of resuscitation is paramount to providing our critically ill patients with the best chance possible.
Objectives
- Review the physiology behind pre-oxygenation.
- Review the incidence of hypoxemia in RSI and complications.
- Discuss the literature and nuances of methods of pre-oxygenation in the emergency department.
- Provide an approach to pre-oxygenation in the critically ill patient.

Mosier, J. The Physiologically Difficult Airway and Management Considerations. Curr. Anesthesiol. Rep. (2024) doi:10.1007/s40140-024-00629-w
Why should you care about perfect pre-oxygenation
When we perform RSI, we place the patient in an involuntary state of apnea. During this time, the total oxygen present in the body is the oxygen available until ventilation resumes. This decreases at a fixed rate dependent on the metabolic consumption of O2 (VO2). Pre-oxygenation is a tool that can be used to increase the total body O2 available thereby increasing the time before critical desaturation.
Mortality and morbidity secondary to physiology
Major adverse events are reported to occur between 25-40% of endotracheal intubations in ED and critical care settings.2–4 Cardiac arrest in the context of endotracheal tube intubation occurs ~1-3%. The risk factors that have been identified include pre-intubation hemodynamic instability, hypoxia, and number of intubation attempts.5–8 Peri-intubation hypoxia has been reported to occur in up to 9-15% of all intubations outside of the operating theatres.2,3
When we break down the risk factors for peri-intubation hypoxia post-intubation we can see many that are prevalent in our patient population:9
- Hypoxic respiratory failure as an indication for intubation
- Lower O2 saturation at induction
- High body mass index
- Operator inexperience (<100 intubations).
- Lack of preparation for intubation before emergent intubation
Breaking it down further, hypoxemia has been demonstrated to be associated with peri-intubation cardiac arrest.7,10 A secondary analysis of the NEAR registry in 2021, by April et al, demonstrated that there is a 3-fold increase of cardiac arrest in those that have hypoxia pre-induction when removing confounders.10 Similarly, an immediate need to intubate without full preparation doubled the risk of peri-intubation cardiac arrest.
Similarly in a retrospective study of hypoxemia in critically ill ICU patients, there was increased inpatient mortality among those who had peri-intubation hypoxemia.11 In this same study, higher baseline oxygenation was protective against peri-intubation hypoxia.
Mortality and morbidity secondary to human factors
While the mortality and adverse effects are in part related to patient complexity and environmental factors, there is likely a component of human factors leading to patient harm.
1. The first pass is key
- The literature has suggested that first-pass success in the emergency department is associated with reduced adverse events. The likelihood of first-pass success without adverse events is decreased in both physiologically and anatomically difficult airways.12
2. Difficult intubations are common
- Difficult airways are encountered in 1-11% of all ED intubations with a failed tracheal intubation in 0-6% of cases. Comparatively, anesthesia reported difficult airways were encountered in 3-8% of cases, and rates of failed intubation 0.006-0.4%.4
3. Are you competent?
- It is not known what number is required to achieve competency, as previously mentioned, some studies have noted that intubators with <100 laryngoscopies are at higher risk of major adverse effects. In addition, it has been suggested that you may need to perform or directly observe 3-5 intubations a year to maintain competence.13
- This may have implications in the rural setting where the patient volumes are low but also in tertiary settings where the learners may do most of the procedures.
4. Situational awareness
- In an observational study looking at the perceived time taken to intubate and the number of desaturations. The physician reported times to intubation were approximately 50% of the actual time. In addition, the reported times that desaturation occurred were only recognized by the intubating physician in 50% of desaturation events. This is DESPITE the saturations being actively verbalized by an RN during the RSI!
5. Preparation is poor
- An observational study in Australia has suggested that as little as ¼ of patients undergoing RSI reach maximal FeO2 before induction.1
Pre-oxygenation Physiology – Keys to Improving Safe Apnea Time
In fundamental terms – When performing RSI, we place the patient in an involuntary state of apnea. During this time, the total oxygen present in the body at the time of induction is the oxygen available until ventilation resumes. This decreases at a rate dependent on the metabolic consumption of O2 (VO2).
Given this, pre-oxygenation has been used as a tool to increase the total body O2 available thereby maximizing the time before critical desaturation.
Your safe apnea time is therefore comprised of 4 factors:
- Your functional residual capacity (FRC) – ie: How large your tank of oxygen is.
- The percentage of O2 contained in the tank. Ie the quality of the fuel in your tank.
- The availability of the reserve to be provided to the body (V/Q and shunt physiology).
- The rate of consumption of O2 (VO2). ie how quickly your fuel will be used.
Safe Apnea Time = (FRC x %O2 x Shunt %)/VO2
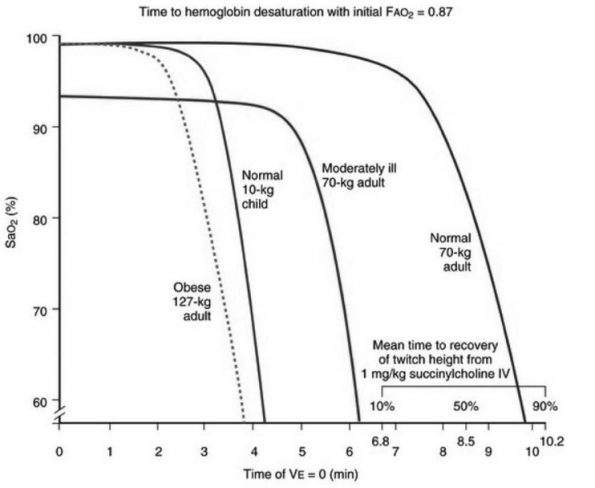
When we look at different populations you can see that the rate and time to desaturation varies depending on the previously mentioned physiological factors. 14
So how does pre-oxygenation maximize these factors:
Functional residual capacity
Conceptually can be thought of as “how large your tank is”. Factors such as age, position, obesity and pregnancy all impact on the FRC. As such recruitment of alveolar segments may further increase your FRC increasing your O2 capacity
Positioning is a key component of how we can optimize this variable.
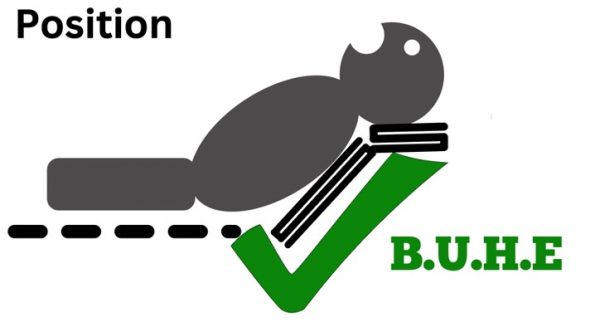
It has been demonstrated in many studies that the ”Back Up Head Extended” position improves safe apnea time and paO2. This is achieved by flexion at the hips by elevating the head of the bed from 20-45% or more whilst extending the neck and aligning the tragus with the sternum. A troop pillow or blankets can be adjuncts to optimize this position.
The primary way this helps with pre-oxygenation is by increasing your FRC volume by offloading compression of the chest/abdominal impedance of the diaphragm, as well as improving V/Q mismatch as such is a critical component in the pre-oxygenation of patients who are pregnant and the morbidly obese. A systematic review and meta-analysis of head-up position in 2022 evaluated 6 RCTs in the OR and one in the ICU that compared head-up oxygenation vs supine position. They found that there was a significant improvement in safe apnoeic time by a mean of 61.99 sec. Similar advantages though have been seen in the non-obese patient population.15
Percent O2/Denitrogenation
At room air, oxygen accounts for only 21% of the gases we inhale. Therefore our lungs are primarily occupied by gases other than oxygen, nitrogen being the majority component. By providing 100% FiO2 we can increase oxygen volume from 450ml to ~3L. In healthy individuals with an FiO2 near 100%, maximal FeO2 occurs within 3 to 5 minutes with tidal volume breathing. This can be expedited through improved alveolar ventilation by hyperventilating or taking maximal breaths. When we do not optimize FeO2 the time to critical desaturation (60%) decreases from 9.9 mins to 2.8 mins in healthy individuals.
V/Q mismatch.
The capacity is only as good as the availability to deliver the O2 to the blood. As such improving the V/Q mismatch in cases of shunting through PEEP may improve the V/Q mismatch. Also as mentioned above the B.U.H.E. position will improve shunt physiology.
Decrease O2 consumption
This is often a fixed variable but influences the rate at which deoxygenation occurs and as such we need to be aware of this. Optimization is through reduction of metabolic demand by appropriately resuscitating the patient and improving fever, pain, work of breathing, and HR. Unfortunately, this is a large topic that is pathophysiology specific so it will not be covered in this post but please refer to the many other posts within the EMOttawa Blog such as Dr. Drew’s review of the surviving sepsis guideline. or Dr. Lacroix’s post on the physiologically difficult intubation.
Practical Application of Pre-Oxygenation – The Players And The Strategy
Monitors
It goes without saying that the most readily available means of assessment of oxygenation is an oxygen saturation probe. However, it should be remembered that this is a surrogate marker for PaO2 and not reflective of denitrogenation. If you consider a healthy person without hypoxemia, a pulse oximeter would demonstrate saturation of 100%, yet the person is not denitrogenated and would have relatively short safe apnea times.
Ideally, we would monitor FeO2 which would give us a better understanding when the patient is maximally denitrogenated. In a study by Oliver et al, FeO2 monitoring improved the number of patients reaching target FeO2 by 44%.18 Unfortunately, FeO2 monitoring is not readily accessible in all EDs and as such we rely upon being diligent and systematic in our approach to pre-oxygenation.
Lastly, we should discuss the role of etCO2 in monitoring our patients for preoxygenation. Whilst not reflective of oxygenation, it allows us to accurately determine when apnea has occurred on induction which is important to prevent loss of denitrogenation.
Non-Rebreather Mask vs Bag-Mask Ventilation
A normal NRB mask with a reservoir is said to have delivered an FIO2 close to 90% at 15L/min. This is true in the normal healthy patient with a minute ventilation of 5-7L/min. Whilst most O2 delivery systems will read up to a maximum flow rate of 15L, the rates that can be delivered are a lot higher. As demonstrated by the evidence below, continue to open the O2 to flush rates to improve O2 delivery.
- In an observational study by Caputo et al 2019, a flush-rate non-rebreather mask is better at achieving higher FeO2 than a non-rebreather at 15 L/min.1
- Driver Et al 2017 compared FeO2 after 3 mins pre-oxygenation with NRB at flush rate vs NRB 15L vs BVM at 15L, and face mask at flush in a small crossover study with healthy volunteers. They demonstrated that NRB was non-inferior to BVM 15L in healthy patients and superior to other modalities.20
- In a follow-up study by Driver Et al in 2018, they compared NRB flush rate to BVM/flush rate and BVM flush with simulated leak. This study demonstrated non-inferiority of NRB at flush rate vs BVM at flush rate in healthy individuals and superior FeO2 (83% vs 30%) when compared to BVM with a simulated leak.21
There are some cons related to the use of NRB likely making it inappropriate in certain patient populations and clinical scenarios and inferior to BVM.
Poor Mask Seal: NRBs lack a cushioned rim and design that would provide a perfect seal around the patient’s face. Therefore with improper positioning/seal, there is going to be entrainment of room. Also consider that if a patient is breathing at a rate of 40 breaths per minute there is so much facial movement that the mask will have inadequate seal.
High-Minute Ventilation: As mentioned above, NRBs are limited by the flow rate of oxygen that can be delivered. If your patient’s minute ventilation exceeds the flow provided then you will run into reductions in FiO2 delivered due to air mixing, or even worse a patient breathing from a depleted reservoir bag. To contextualize this follow this scenario;
- The typical Tidal Volume (TV) for a 70kg patient is ~7ml/kg.
- A patient with a respiratory rate of 40, may have a minute ventilation of 70x7x40 = ~ 20L/min. Factor in increases in TV seen in these patients which may drive minute ventilation upwards of 40L /min.
- As you can see, those that have such high minute ventilation would not be receiving sufficient O2 to achieve 100% FiO2 and would rebreathe exhaled CO2.
Studies have demonstrated this concept. In patients with higher minute ventilation or poor seal entrainment of room air can lead to FiO2 in the range of ~60% maximally, thereby preventing complete denitrogenation and therefore reducing safe apnea time.19,20
Therefore, In the ED, a tight seal NRB mask at flush rate can be considered in those with a very low risk of desaturation and low minute ventilation. In every other scenario, however, you will get more effective pre-oxygenation using a BVM with a PEEP valve.
Apneic Oxygenation
Apneic oxygenation is as the name suggests, continuous oxygenation during the period of apnea, before ventilation commencement. It is usually administered through a nasal cannula (NC) or high-flow nasal cannula (HFNC). The theory is that as the patient utilizes the alveolar O2 which diffuses across the alveolar wall, it is replenished by a fresh reservoir drawn in by the pressure gradient generated.22 As the replaced O2 is provided intra-nasally, airway patency is paramount to this being an effective method of oxygenation. HFNC has an added advantage of providing a small amount of PEEP which assists with recruitment as well as higher flow rates. Prolonged safe apnea times have been observed in both NC and HFNC.23
In Healthy Populations
Within the operating room, there have been clear indications that it prolongs safe apneic time in healthy individuals.24–26 A systematic review and meta-analysis by Carvalho in April 2024, looked at the effectiveness of different pre-oxygenation strategies. It assessed 52 studies of almost 4000 patients.26 They found the following:
- Apneic HFNC in the head-up position prolonged safe apnea times by more than 4 mins compared to NRB facemask.
- Rates of arterial desaturation were decreased by 66% when compared to NRB without apneic oxygenation.
- HFNC as a pre-oxygenation modality in the head-up position improved safe apnea time in those with impaired FRC but not having refractory shunt.
In Critically Ill Populations
In the setting of the critically ill patient, the evidence for preventing hypoxemia is controversial in recent literature.27–29.
- A systematic review and meta-analysis conducted by E Silva Et Al in 2017 included more than 1800 patients. Apneic oxygenation was associated with decreased hypoxemia and increased first-pass success but not associated with prevention of severe hypoxemia (Sats <85%).
- The ENDAO trial conducted by Caputo et al in 2019, an open-label RCT of 206 patients, did not demonstrate any significant difference in mean O2 sats or critical desaturation when at least 3 minutes of pre-oxygenation was provided (average 13mins). It should be noted however that the majority did not experience prolonged apnea.
- Similarly, a Cochrane review in 2023 on apneic oxygenation did not find that it likely caused a clinically significant improvement in oxygenation during intubation.30
The use of apneic oxygenation has not been shown to decrease the rate of desaturation in critical care patients. There have been some interesting associations that are worth commenting on.
- A meta-analysis by Jhou et al 2020 compared HFNC to NRB in ICU patients. They found HFNC to be non-inferior to NRB in terms of rates of desaturation. There was a benefit seen in subgroup analysis in patients with a PaO2/FiO2 ratio >200 in preventing severe hypoxemia.
- In the Pre-AERATE trial 2022, the lowest SpO2 after the first attempt at intubation was compared between apneic oxygen via HFNC vs conventional oxygen therapy. No significant difference was found. However, there was an association between improved safe apnea time and lower rates of desaturations on repeat intubation attempts.
- In the PROTRACH study, a multi-centre ICU study in 2019, Guitton et al compared HFNC with apneic O2 to BVM at 15L in mild hypoxemia PaO2/FIO2 ratio >200. There was no difference in lowest SpO2, but significantly fewer major adverse events despite a higher patient population with difficult airways and longer intubation time.
The Low Down on Apneic Oxygenation
Therefore, to summarize, there may be some benefit to prolongation of apnea time when apneic oxygenation is used which may be useful in the difficult airway scenario. Given that HFNC may not frequently be available in the ED, a nasal cannula at 15L for apneic oxygenation is likely to be a useful adjunct given the frequency of difficult airways being encountered in the ED. It is important to note though that lower flow rates may impair your pre-oxygenation particularly if using BVM to pre-oxygenate.31g
Non Invasive Positive Pressure Ventilation (NIPPV)
In the critically ill patient population, particularly in the cases of severe hypoxic respiratory failure, NIPPV has been demonstrated to be superior to BVM, HFNO, NRB:
- The FLORALI-2 study, a Multicentre open-label RCT of 322 ICU patients, compared NIV vs HFNC with apneic oxygenation in acute hypoxic respiratory failure. There was no difference in all comers however, in the PaO2/FiO2 group < 200 there was significantly reduced severe hypoxemia with an aOR 0.55.
- In a comparative study done by Bailly et al 2019, post-hoc analysis of the MACman study showed that compared to forms of pre-oxygenation, both BVM and NIV have been demonstrated to be more effective at preventing desaturation in severe hypoxia than NRB mask. The study indicated that NIV was favourably compared to BVM with an aOR of 0.1.
The Evidence-Based Strategy – BVM and NIV
Bead Up Head Elevated Always! There is no way to say how important this is in improving your respiratory physiology.
The BVM and NIV should be the workhorse of pre-oxygenation. As summarized above, given good technique and adequate mask seal, this strategy will optimize your denitrogenation, recruit alveolar segments with PEEP (increasing FRC and optimizing V/Q mismatch) and provide apneic oxygenation. In the meta-analysis by Carvalho 2024, pressure support in the upright position significantly reduced the odds of arterial desaturation when compared to face mask pre-oxygenation.26 When using BVM, try employing a two-handed seal whenever possible. Driver et al in 2019 demonstrated that loss of seal resulted in a decrease by a mean of 51% FeO2. This also highlights the importance of etCO2 in monitoring for apnea onset.
In the case of your severely ill respiratory failure patient consider NIPPV as your pre-oxygenation strategy before intubation.
The Final Word of Caution – To RSI or not to RSI
There are circumstances where apnea will not be tolerated such as significant hypoxia despite optimization of pre-oxygenation or the patient has significant physiological derangement such as hypotension or acidosis. In these situations, we need to consider whether intubation is absolutely indicated and whether RSI is the right procedure.
A retrospective observational ICU study from Germany in 2023 demonstrated a 2.2% adverse event rate in the awake intubation group compared to 27% in the RSI group. There were some limitations with this study that limited applicability in the ED. All awake intubations were done with HFNC oxygenation (which isn’t always readily available) compared to none in the RSI group, as well as all awake intubations were performed by residents with an anesthetic consultant of > 5 years of experience to guide the awake intubation process.
Despite these limitations, this should encourage us as emergency physicians to develop the necessary skills in awake intubation as there is a subset of patients who will benefit from this technique.
References
- Caputo, N. D., Oliver, M., West, J. R., Hackett, R. & Sakles, J. C. Use of End Tidal Oxygen Monitoring to Assess Preoxygenation During Rapid Sequence Intubation in the Emergency Department. Ann. Emerg. Med. 74, 410–415 (2019).
- Downing, J. et al. Prevalence of peri-intubation major adverse events among critically ill patients: A systematic review and meta-analysis. Am. J. Emerg. Med. 71, 200–216 (2023).
- Russotto, V. et al. Intubation Practices and Adverse Peri-intubation Events in Critically Ill Patients From 29 Countries. JAMA 325, 1164–1172 (2021).
- Law, J. A. et al. Canadian Airway Focus Group updated consensus-based recommendations for the management of the difficult airway: part 1. Difficult airway management encountered in an unconscious patient. Can. J. Anaesth. J. Can. Anesth. 68, 1373–1404 (2021).
- Marin, J., Davison, D. & Pourmand, A. Emergent endotracheal intubation associated cardiac arrest, risks, and emergency implications. J. Anesth. 33, 454–462 (2019).
- Park, C. Risk factors associated with inpatient cardiac arrest during emergency endotracheal intubation at general wards. Acute Crit. Care 34, 212–218 (2019).
- Yang, T.-H., Chen, K.-F., Gao, S.-Y. & Lin, C.-C. Risk factors associated with peri-intubation cardiac arrest in the emergency department. Am. J. Emerg. Med. 58, 229–234 (2022).
- De Jong, A. et al. Cardiac Arrest and Mortality Related to Intubation Procedure in Critically Ill Adult Patients: A Multicenter Cohort Study. Crit. Care Med. 46, 532–539 (2018).
- McKown, A. C. et al. Risk Factors for and Prediction of Hypoxemia during Tracheal Intubation of Critically Ill Adults. Ann. Am. Thorac. Soc. 15, 1320–1327 (2018).
- April, M. D. et al. Peri-intubation cardiac arrest in the Emergency Department: A National Emergency Airway Registry (NEAR) study. Resuscitation 162, 403–411 (2021).
- Smischney, N. J. et al. Risk Factors for and Outcomes Associated With Peri-Intubation Hypoxemia: A Multicenter Prospective Cohort Study. J. Intensive Care Med. 36, 1466–1474 (2021).
- Pacheco, G. S. et al. First Pass Success Without Adverse Events Is Reduced Equally with Anatomically Difficult Airways and Physiologically Difficult Airways. West. J. Emerg. Med. 22, 360–368 (2021).
- Gillett, B., Saloum, D., Aghera, A. & Marshall, J. P. Skill Proficiency is Predicted by Intubation Frequency of Emergency Medicine Attending Physicians. West. J. Emerg. Med. 20, 601–609 (2019).
- Benumof, J. L., Dagg, R. & Benumof, R. Critical hemoglobin desaturation will occur before return to an unparalyzed state following 1 mg/kg intravenous succinylcholine. Anesthesiology 87, 979–982 (1997).
- Hung Tsan, S., Viknaswaran, N., Lau, J., Cheong, C. & Wang, C. Effectiveness of preoxygenation during endotracheal intubation in a head-elevated position: a systematic review and meta-analysis of randomized controlled trials. Anaesthesiol. Intensive Ther. 54, 413–424 (2022).
- Tsan, S. E. H., Lim, S. M., Abidin, M. F. Z., Ganesh, S. & Wang, C. Y. Comparison of Macintosh Laryngoscopy in Bed-up-Head-Elevated Position With GlideScope Laryngoscopy: A Randomized, Controlled, Noninferiority Trial. Anesth. Analg. 131, 210–219 (2020).
- Couture, E. J. et al. Effect of reverse Trendelenburg position and positive pressure ventilation on safe non-hypoxic apnea period in obese, a randomized-control trial. BMC Anesthesiol. 23, 198 (2023).
- Oliver, M., Caputo, N., West, J. R., Hackett, R. & Sakles, J. C. 44 Impact of End-Tidal Oxygen Monitoring on the Efficacy of Preoxygenation During Rapid Sequence Intubation in the Emergency Department. Ann. Emerg. Med. 74, S18 (2019).
- Weingart, S. D. & Levitan, R. M. Preoxygenation and Prevention of Desaturation During Emergency Airway Management. Ann. Emerg. Med. 59, 165-175.e1 (2012).
- Driver, B. E., Prekker, M. E., Kornas, R. L., Cales, E. K. & Reardon, R. F. Flush Rate Oxygen for Emergency Airway Preoxygenation. Ann. Emerg. Med. 69, 1–6 (2017).
- Driver, B. E. et al. Preoxygenation With Flush Rate Oxygen: Comparing the Nonrebreather Mask With the Bag-Valve Mask. Ann. Emerg. Med. 71, 381–386 (2018).
- Fayed, M., Maroun, W., Patel, N. & Galusca, D. Apneic Oxygenation: A Summarized Review and Stepwise Approach. Cureus 15, e50916 (2023).
- Mosier, J. et al. Time to Loss of Preoxygenation in Emergency Department Patients. J. Emerg. Med. 59, 637–642 (2020).
- Vourc’h, M. et al. High-flow Nasal Cannulae Versus Non-invasive Ventilation for Preoxygenation of Obese Patients: The PREOPTIPOP Randomized Trial. EClinicalMedicine 13, 112–119 (2019).
- Jaber, S. et al. Preoxygenation with standard facemask combining apnoeic oxygenation using high flow nasal cannula versus standard facemask alone in patients with and without obesity: the OPTIMASK international study. Ann. Intensive Care 13, 26 (2023).
- Crístian de Carvalho, C. et al. Effectiveness of preoxygenation strategies: a systematic review and network meta-analysis. Br. J. Anaesth. S0007-0912(24)00130–2 (2024) doi:10.1016/j.bja.2024.02.028.
- Miguel-Montanes, R. et al. Use of high-flow nasal cannula oxygen therapy to prevent desaturation during tracheal intubation of intensive care patients with mild-to-moderate hypoxemia. Crit. Care Med. 43, 574–583 (2015).
- Caputo, N. et al. Emergency Department Use of Apneic Oxygenation Versus Usual Care During Rapid Sequence Intubation: A Randomized Controlled Trial (The ENDAO Trial). Acad. Emerg. Med. Off. J. Soc. Acad. Emerg. Med. 24, 1387–1394 (2017).
- Crewdson, K., Heywoth, A., Rehn, M., Sadek, S. & Lockey, D. Apnoeic oxygenation for emergency anesthesia of pre-hospital trauma patients. Scand. J. Trauma Resusc. Emerg. Med. 29, 10 (2021).
- White, L. D., Vlok, R. A., Thang, C. Y., Tian, D. H. & Melhuish, T. M. Oxygenation during the apnoeic phase preceding intubation in adults in prehospital, emergency department, intensive care and operating theatre environments. Cochrane Database Syst. Rev. (2023) doi:10.1002/14651858.CD013558.pub2.
- McQuade, D., Miller, M. R. & Hayes-Bradley, C. Addition of Nasal Cannula Can Either Impair or Enhance Preoxygenation With a Bag Valve Mask: A Randomized Crossover Design Study Comparing Oxygen Flow Rates. Anesth. Analg. 126, 1214–1218 (2018).
- Mosier, J. The Physiologically Difficult Airway and Management Considerations. Curr. Anesthesiol. Rep. (2024) doi:10.1007/s40140-024-00629-w.
