

Point of Care Ultrasound (PoCUS) for the evaluation and diagnosis of gallbladder related disease is becoming commonplace in the Emergency Department. Here, we present a quiz to test your knowledge, some answers, and helpful tips and tricks to enhance your gallbladder PoCUS game!
Gallbladder Ultrasound Quiz
Click on the case to take the quiz before reading more about Gallbladder Sonography below !
Case 1
Case 2
Case 3
Case 4
Case 5
Case 6
Case 7
Case 8
——————————————————————————————–
Acute Cholecystitis is one of the most common complications of gallstone disease, and a frequent cause of right upper quadrant pain in patients presenting to the emergency department.
No single clinical or laboratory test carries a sufficiently high positive or negative likelihood ratio to rule out the diagnosis of acute cholecystitis (1,2). The evaluation of patients with suspected acute cholecystitis is supported by the appropriate imaging studies (2).
Ultrasound is the investigation of choice in the initial evaluation of acute biliary disease (3). ED PoCUS has been shown to be similarly accurate to radiology performed ultrasound when the following sonographic features are present (4, 5).
- Presence of gallstones plus one or more secondary finding
- Sonographic Murphy’s sign
- Gallbladder wall thickening
- Pericholecystic fluid
Clinical Algorithm
Point-of-care biliary ultrasound performed by emergency physicians provides timely access to diagnostic information and is associated with shorter ER visits (6). Multiple algorithms have been proposed in the literature for PoCUS assessment for possible acute cholecystitis (6,7). A suggested clinical algorithm incorporating emergency department (ED) PoCUS is shown in figure 1.
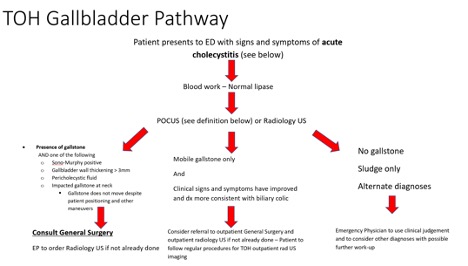
Figure 1: Recommended approach to investigating gallstone complications in the ED
Approach to scanning
The goal of the PoCUS exam is to visualize the entire gallbladder in both its longitudinal (long axis) and transverse (short axis) in order to avoid false negatives for gallstones. Several approaches may be used to optimize visualization.
General steps for performing PoCUS of gallbladder
- Select the curvilinear transducer (2.5-3.5MHz)
- The patient should be supine
- Place the transducer adjacent to the xiphoid process, and ensure it is in true transverse orientation (straight up and down)
- Heel the probe cephalad to identify the caudal tip of the liver
- From the epigastrium, keeping the liver in view, slide the probe along the costal margin to the right
- The gallbladder is usually situated close to the right anterior axillary line, look for the portal vein which forms the “exclamation sign” with the gallbladder
- Use color doppler function to distinguish gallbladder from other fluid filled structure such as the IVC
If in doing so, you do not see the gallbladder well or at all, apply the following troubleshooting tips to optimize your image
- Ask the patient to do an inspiratory hold or push the abdomen out. This will cause the liver to shift caudally and push the gallbladder out from the thoracic cage
- Place the patient in lateral decubitus position – this helps to bring the gallbladder out from under the ribs and help to displace bowel gas
- Lateral approach – start with the RUQ view of FAST scan, locate the hepatorenal interface. Then slowly sweep the bean anteriorly until the gallbladder appears in view
- Intercostal approach –consider using a probe with a smaller footprint such as the phase array. Start right midclavicular line, and sweep the probe caudad then cephalad, as well as sliding medial and lateral at each intercostal space.
Once you have identified the gallbladder, sweep slowly in its long and short axis in order to identify for the presence of gallstones, anterior wall thickening, and presence of pericholecystic fluid.
Interpretation of Gallbladder Ultrasound
References
- Trowbridge, R. L., Rutkowski, N. K., & Shojania, K. G. (2003). Does this patient have acute cholecystitis?. Jama, 289(1), 80-86.
- Jain A, Mehta N, Secko M, Schechter J, Papanagnou D, Pandya S, et al. History, Physical Examination, Laboratory Testing, and Emergency Department Ultrasonography for the Diagnosis of Acute Cholecystitis. Acad Emerg Med. 2017;24(3):281–97.
- O’Connor, O. J., & Maher, M. M. (2011). Imaging of cholecystitis. American Journal of Roentgenology, 196(4), W367-W374.
- Ross M, Brown M, McLaughlin K, Atkinson P, Thompson J, Powelson S, et al. Emergency physician-performed ultrasound to diagnose cholelithiasis: A systematic review. Acad Emerg Med. 2011;18(3):227–35.
- Summers, Shane M., William Scruggs, Michael D. Menchine, Shadi Lahham, Craig Anderson, Omar Amr, Shahram Lotfipour, Seric S. Cusick, and J. Christian Fox. “A prospective evaluation of emergency department bedside ultrasonography for the detection of acute cholecystitis.” Annals of emergency medicine 56, no. 2 (2010): 114-122.
- Hilsden, R., Leeper, R., Koichopolos, J., Vandelinde, J. D., Parry, N., Thompson, D., & Myslik, F. (2018). Point-of-care biliary ultrasound in the emergency department (BUSED): implications for surgical referral and emergency department wait times. Trauma surgery & acute care open, 3(1), e000164.
- Villar, J., Summers, S. M., Menchine, M. D., Fox, J. C., & Wang, R. (2015). The absence of gallstones on point-of-care ultrasound rules out acute cholecystitis. The Journal of emergency medicine, 49(4), 475-480.


this was really nice. thank you for taking the time to post this.