
Hey everyone! Buckle up. This is a long one. To provide context, I recently presented a 2-part blog post regarding thrombolytics in acute ischemic stroke. In these posts I explored the foundational literature for this tPA, as well as some of the common controversies I had seen online. Part I can be found here, and you’ll find part 2 here.
A reply to this post was made by Dr. Justin Morgenstern on the First10EM blog, with some critiques of my post, found here.
To keep stirring the pot on this classic debate, I detail some responses to Dr. Morgenstern’s arguments.
I want to start off with one point of clarification:
My articles are not a reply to the recent NNT article he and Dr. Ken Milne authored, and so I can’t agree with the start of his article, or any of the points suggesting my arguments are strawmen, as they are simply independent arguments. Based on a discussion over twitter, I think both Justin & I are on the same page on this one now.
Moving on.
Argument 1
The first point discusses that I refer to ATLANTIS B as the first negative tPA trial, and that this insinuates some bias within my article. I think this is a matter of language, and perhaps I should have been more clear: ATLANTIS-B showed clear harm. In my mind I differentiate harm from equipoise.
ECASS-1 was negative for its primary outcome. However, the modified intention to treat, which was in my opinion very reasonably justified due to a high proportion of protocol violations (17.5%) found an OR of 1.29 (95% CI 1.09-1.54) P = 0.035 for an outcome of functional independence. With respect to mortality, there was no difference. Omitting this in countering my argument in my opinion constitutes a strawman argument itself, but I will leave that digression aside.
This is powerful data, this highlights that at the time we couldn’t select the right patients, but that if we did, there could be benefit.
To dismiss this as a negative trial seems remiss, and so I didn’t take that stance. I considered it neutral, as it added to the body of evidence for tPA, but did not in isolation inform us on which patients would benefit. ECASS-1 hinted to us that this was an agent with potential. This is akin to many of the original endovascular studies in stroke, which struggled to identify which patients may benefit originally.
Simplifying this rich data to a p-value of 0.38 without looking deeper is the first point where I disagree with Dr. Morgenstern.
Similarly, with respect to ECASS-II, this study again adds to the pool of data we have. Their primary outcome looked at excellent neurological outcomes (mRS 0 or 1) for tPA vs placebo and found a 3.7% benefit, favouring tPA, that was not statistically significant (P = 0.277). Dr. Morgenstern argues that this is clearly a negative trial.
When we look at the less optimistic outcome of good neurological outcomes (mRS 0-2) for tPA vs placebo, we see a 8.3% absolute benefit that is statistically significant (P = 0.024). This was not a pre-specified outcome, and it was not a primary outcome, and that deserves scrutiny. But to not consider this rich data, once again, is in my opinion problematic.
I again, consider ECASS 2 to be a neutral trial. It hinted at benefit and a demand for highly nuanced care, and so was hypothesis generating for further, more refined trials. I think this is a fairly unbiased interpretation of the devil in the details of the tPA literature, but I’ll let you, the reader, decide that one.
Argument 2
Dr. Morgenstern next highlights that in my articles, the discussion is biased because only a subset of trials are discussed.
I think Dr. Morgenstern and I may differ fundamentally here, and this may be a difference of opinions that we can’t rectify. His view is that as a general rule in medicine, we assess drugs as a class and that it is a rare exception when one member of a class turns out to be superior to another.
As was already brought up on twitter previously, I think it is easy to find examples where this is not the case: amoxicillin vs piperacillin-tazobactam for sepsis, clopidogrel vs ticagrelor for ACS…the list goes on.
When this was raised on twitter, the reply was that this is generally taught as part of evidence based medicine. To me that sounds like justifying dogma.
As it applies to the tPA debate, Dr. Morgenstern’s view is that tPA = all other thrombolytics.
My view is that tPA has its own pharmacologic properties, some agents may be quite similar, others different, and each have their own safety & benefit profiles. As tPA is the drug that we use clinically, and is the drug we have the most evidence for, it was the one I focused my article on. This is not ignoring negative trial results.
Dr. Morgenstern goes on to cite the Wardlaw 2014 Cochrane review and the 2016 donaldson et al. systematic review and meta-analysis as an argument that all thrombolytic agents should be considered equal. This is not the conclusion I derived from these papers.
From the Wardlaw paper:
“Quality of the evidence: The overall quality of evidence, particularly for the drug with the majority of data, rt-PA, is good. The concerns about quality in earlier trials are largely overcome. The recent trials had good allocation concealment, central telephone randomization, central blinded follow-up, and very few losses to follow-up.”
“Thrombolytic therapy given up to six hours after stroke reduces the proportion of dead or dependent people. Those treated within the first three hours derive substantially more benefit than with later treatment. This overall benefit was apparent despite an increase in symptomatic intracranial haemorrhage, deaths at seven to 10 days, and deaths at final follow-up (except for trials testing rt-PA, which had no effect on death at final follow-up)”
From the Donaldson meta-analysis:
Impact of tPA on functional independence: OR 1.2 (95% CI 1.08 – 1.33) P = 0.001
Impact of tPA on mortality: OR 1.04 (95% CI 0.92 – 1.18) P = 0.49
Impact of all thrombolytics on functional independence: OR 1.14 (95% CI 1.04 – 1.25) P = 0.004
Impact of all thrombolytics on mortality: OR 1.17 (95% CI 1.06 -1.30, P = 0.003)
tPA is equal to all thrombolytics with respect to its impact on improving functional independence. But it has a better safety profile. I think these two papers quite clearly show that. And this makes sense, it’s consistent with the pharmacologic properties of tPA as a specific fibrinolytic agent, as compared with a less specific agent like streptokinase. It provides the modest benefit of earlier generation thrombolytic agents but with a better safety profile (complete sidebar – this is why the stroke world is really excited about TNK right now – but that’s another topic entirely).
I am advocating that the existing data shows benefit for tPA with acceptable safety. I would not advocate for the use of an agent such as streptokinase, as the formative trials on that thrombolytic agent (MAST-I, MAST-EU, ASK) had discouraging results regarding the potential for harm.
Argument 3
“The second part of this article is broken down into 4 arguments that are supposedly made against thrombolytics, and provides rebuttals to those arguments. In my mind, this is where the strawman seems to arise, as these are not arguments I have ever made, nor are they made in the NNT article that provoked this discussion.”
Again – the article provides 4 arguments I have frequently come across, but they are independent arguments and weren’t inspired by the NNT article, so to call them a strawman strikes me as unfair.
Argument 4
“No one thinks the Hoffman re-analysis invalidates the findings of NINDS” – I’d disagree with this. There’s definitely those that have this impression, and it’s why I wrote this argument in my article. Regarding the methodology of NINDS, I 100% agree that we can’t take this is a stand alone trial and not look further. The study was positive, but it was from 1995, and it had its limitations. Totally agree.
It’s this trial, in conjunction with all of the other trials that I highlight in part 1 that convince me of the benefit for tPA within 4.5 hours. It is not any trial on its own.
Argument 5
This argument by Dr. Morgenstern centers around the time is brain paradigm only being a hypothesis.
I agree that it is not an absolute and shouldn’t be considered as such. With that said, I never suggested that it was an absolute, but rather that it is a very biologically plausible hypothesis, which has data supporting it. For the entire picture of an individual patient’s stroke timeline we now look to perfusion imaging, rather than painting every person with the same brush and using crude time cut offs as we once did.
To be a purist however, there is much more evidence than just the Lees 2010 paper to support that earlier therapy provides better outcomes, and later therapy caries more risk:
- Emberson et al individual patient data meta-analysis:
- Excellent neuro outcomes in pts receiving tPA <3h. Absolute improvement of 9.8% compared to placebo, OR 1.75 (95% CI 1.35 – 2.27) p < 0.0001
- Excellent neuro outcomes in pts receiving tPA 3-4.5h. Absolute improvement of 5.2% compared to placebo. OR 1.26 (95% CI 1.05 – 1.51) p = 0.0132
- Mortality in pts receiving tPA <3h. Difference of 0.3%, HR 1.00 (0.81 – 1.24)
- Mortality in pts receiving tPA 3 – 4.5h. Difference of 1.0%, HR 1.14 (0.95 – 1.36) ptrend = 0.22
Figure 1 in particular from the Emberson paper is quite compelling.
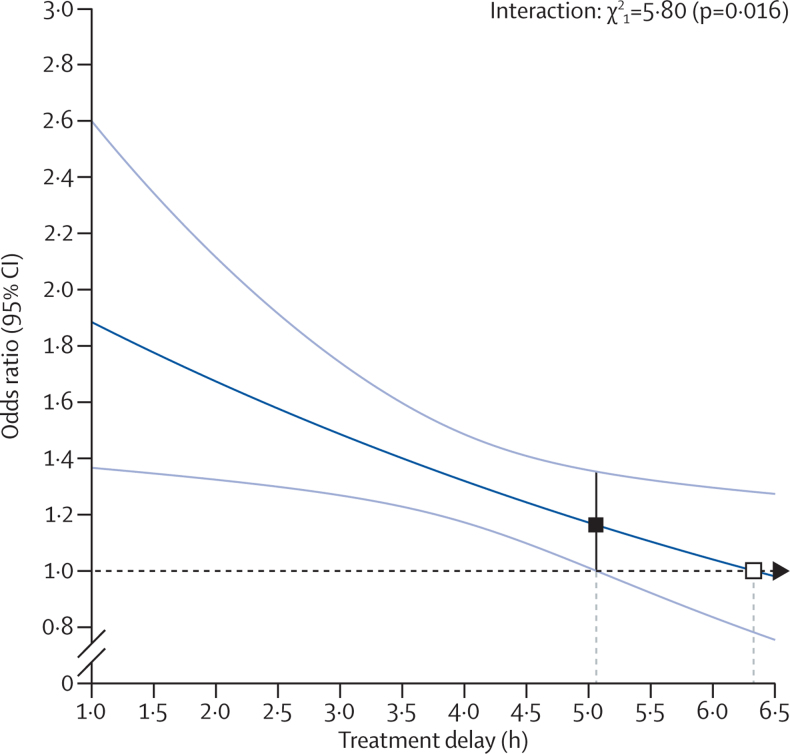
Effect of timing of alteplase treatment on good stroke outcome (mRS 0–1). Figure 1, Emberson et al.
Additionally, I’m not sure I follow Dr. Morgenstern’s argument that the 2014 Wardlaw paper argues against the time is brain hypothesis, when they corroborate the findings of the Emberson paper:
“Treatment within three hours of stroke was more effective in reducing death or dependency (OR 0.66, 95% CI 0.56 to 0.79) without any increase in death (OR 0.99, 95% CI 0.82 to 1.21; 11 trials, 2187 participants).”
And
“ Trials testing rt‐PA showed a significant reduction in death or dependency with treatment up to six hours (OR 0.84, 95% CI 0.77 to 0.93, P = 0.0006; 8 trials, 6729 participants) with significant heterogeneity; treatment within three hours was more beneficial (OR 0.65, 95% CI 0.54 to 0.80, P < 0.0001; 6 trials, 1779 participants) without heterogeneity.”
Argument 6
Regarding my point around a common argument “The harms are too high, and outweigh any benefit”, Dr. Morgenstern agrees that this is an argument he has heard made before.
He however shifts to point out that it should rather be an argument of certainty, and that we have fairly high certainty around the potential for harms (at least around symptomatic intracranial hemorrhage), and less certainty due to trial limitations, bias etc for the positive effects of tPA.
I think this is a very reasonable point. Additionally, I really appreciate the following point which Dr. Morgenstern makes:
“I will correct one common meme about thrombolytics: it is inappropriate to compare the rate of intracranial hemorrhage with the rate of neurologic improvement. Long term functional outcomes include those patients who had head bleeds, so if there is a true benefit, it is a benefit that outweighs the harm from head bleeds, and those bleeds actually become somewhat irrelevant.”
Ultimately, this point of discussion seems to highlight a difference in our respective confidence in the underlying data, which is totally okay. Full disclaimer: I don’t think the literature for tPA is amazing.
I DO however think it’s good enough to justify using it as a treatment for certain patients, to provide modest benefit from a disabling disease. Moreover, while further study may ease that burden of uncertainty, I don’t know that it could be done ethically, given reasonably compelling evidence supporting the benefit this therapy provides.
Argument 7
I completely agree that the Alper paper highlights that we should be less certain in the data ECASS III generated. That is the conclusion the authors of the Alper paper provide.
ECASS III was a borderline paper. The FDA rejected it’s findings in the context of approving tPA for administration up to 4.5h. If you ask most stroke neurologists they acknowledge that this paper was limited. I’m not debating that!
ECASS III added momentum to a 4.5h window, but it is not the base of support for it. The support for it comes from the aggregate data from all of the existing tPA trials.
The follow up point is probably the one presented by Dr. Morgenstern that I agree with most – and that is that the pooling of data in the individual patient data meta-analyses is limited because negative trials were stopped early and thus weighted less heavily. I am certain that this has impacted the data to some extent.
The evidence which reassures me that we haven’t been wildly led astray by these meta-analyses however, is the existing registry data which corroborates the observed benefit and harm profile of tPA. The functional improvements, rates of intracranial hemorrhage and rates of mortality observed in the SITS-MOST, CASES and STARS registries have all been concordant with the existing RCT data.
Is this perfect? No, not at all.
It does however reassure me that the existing tPA literature translates acceptably to the real world, and that we probably aren’t too far off the mark of whatever the actual “universal” truth is. Moreover, it emphasizes why as emergency physicians practicing in Canada we’re privileged to be able to have neurologists available in consultation, either in person or via telestroke, to help us navigate the nuance of this disease entity and its treatments.
Cheers,
Doran

Here is the SGEM blog with Dr. Morgenstern that discusses our downgrading of tPA for acute ischemic stroke to “yellow” https://www.thesgem.com/2021/05/sgem-xtra-the-nnt-is-mellow-yellow-for-tpa-in-acute-ischemic-stroke/