

Patients with both burn and inhalation injuries have significantly increased morbidity and mortality compared to those with just burn injuries alone, as there are multiple toxic industrial chemicals that act on the respiratory tract.
In this post, we review inhalational injuries and the most common Toxic Industrial Chemicals leading to pulmonary injury through summarizing the JTS’ CPG on the subject.
For other topics related to Military Medicine, please see our posts on Damage Control Resuscitation, TCCC and Recent Updates, Prolonged Field Care, Blast Injuries, Abdominal Stab Wound, and Resuscitative Thoracotomy.
The Basics: Smoke Inhalation
- The primary initial insults from smoke inhalation are (1) thermal injury and (2) chemical injury; systemic toxicity can also occur (toxic substances or immune responses to injury)
- Thermal injury occurs primarily in the upper airways
- Chemical injury occurs secondary to products of combustion and pyrolysis
- These can include pulmonary irritants and asphyxiants
- The pulmonary irritants involved can be categorized according to water-solubility:
- Higher water-solubility = more proximal airway damage; less water-solubility = slower onset of injury, more distal airway damage
- Highly water-soluble irritants: acrolein, sulfur dioxide, hydrogen chloride, ammonia
- Intermediate water-soluble irritants: chlorine, isocyanates
- Poorly water-soluble irritants: oxides of nitrogen and phosgene
- An asphyxiant reduces the amount of oxygen available to an individual
- Simple asphyxiants displace oxygen; e.g. carbon dioxide, methane
- Chemical asphyxiants inhibit mitochondrial activity and reduce hemoglobin carrying capacity; e.g. CO, CN, hydrogen sulfide
- Smoke inhalation itself is treated with supportive care (with a focus on airway management; definitive control if required), though some exposures may require antidotes (discussed below)
- Most critically ill patients require lung-protective ventilation as used for ARDS
The Basics: Toxic Industrial Chemical Inhalation Injury
As with smoke inhalation, care is supportive with a focus on:
Airway Management:
- Lung protective ventilation strategies
- Aggressive pulmonary toilet, and
- Avoidance of volume overload that might worsen pulmonary edema secondary to capillary leak
Note that patients requiring mechanical ventilation secondary to toxic industrial chemical inhalation, in particular, chlorine, are at a higher risk of developing ventilator-associated pneumonia and should be monitored closely.
Common Inhalation Injuries
Here is a quick summary, see the accompanying text below for more details.
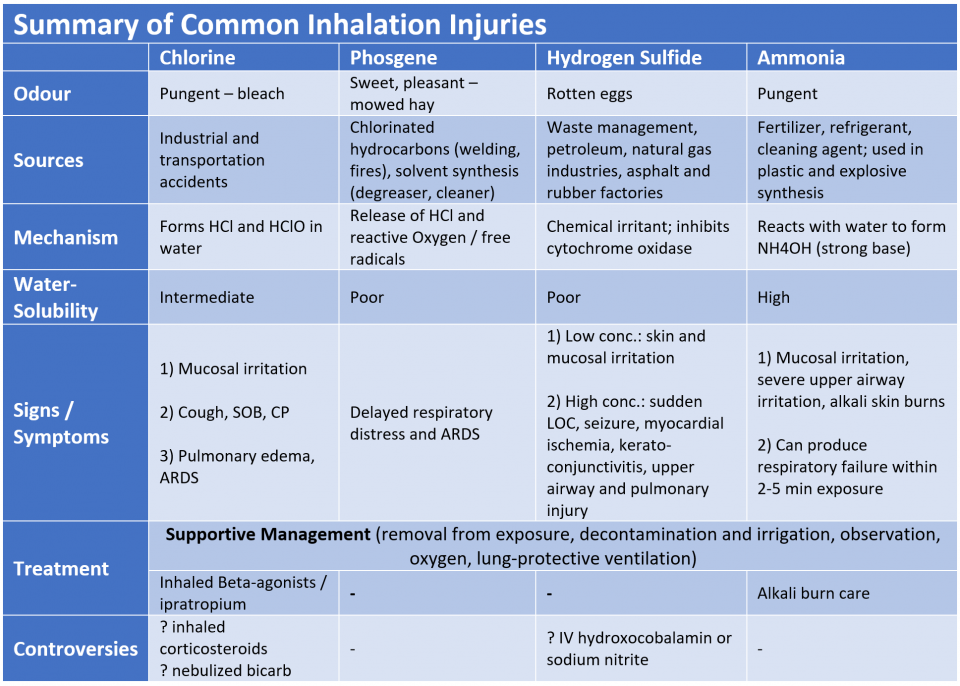
Chlorine
- Odour: pungent smell similar to bleach
- Sources: used commonly in industry; commonly found in industrial and transportation accidents, sometimes used in IEDs; WW1 as a weapon
- Mechanism: dissolves in water to form hydrochloric and hypochlorous acids
- Water-solubility: intermediate
- Signs/Symptoms:
- Initial: mucosal irritation (tearing, skin burning, drooling)
- Then: cough, shortness of breath, and chest pain due to alveolar injury
- If pulmonary toxicity then pulmonary edema may worsen over days, ARDS may develop
- Treatment: skin decontamination, supplemental oxygen, inhaled beta agonists, lung-protective ventilation
- Controversies:
- Inhaled corticosteroids (e.g. fluticasone) improved secondary outcomes in severely toxic animal models but clinical data in humans are inconclusive
- Prone position mechanical ventilation may be effective
- Nebulized bicarb has not reliably improved outcomes
Chlorine toxic patients should be stratified based on symptoms severity into asymptomatic, mild, moderate, and severe symptoms. Treatment and observation periods can be tailored based on these categories.
- Asymptomatic
- Diagnosis: no symptoms
- Management: none
- Disposition: discharge if normal assessment (respiratory exam, vital signs, and pulse ox)
- Mild
- Diagnosis: minimal symptoms, coughing, normal pulse oximetry, and no increased respiratory effort
- Management: CXR, inhaled beta agonists
- Disposition: observe up to 6 hours, most can be discharged
- Moderate
- Diagnosis: hypoxia, increased respiratory effort
- Management: CXR, inhaled beta agonists
- Consider inhaled steroids (fluticasone 200 mcg BID or similar), early intubation, inhaled ipratropium
- Disposition: Admission (observation for at least 12 hours)
- Severe
- Diagnosis: hypoxia, severe respiratory distress, often require intubation
- Management: as Moderate, humidified oxygen and early intubation with 8.0 tube to allow bronchoscopy
- Consider inhaled steroids as above, inhaled ipratropium if no improvement, if unable to administer inhaled medications or significant bronchoconstriction then consider IV steroids
- ARDS: lung protective ventilation strategy; increased PEEP, low TdV, observe for barotrauma, may require high dose sedatives to maintain ventilator synchrony
- Disposition: Admission to ICU
Important Caveats
- Decontaminate all symptomatic skin surfaces
- Remove all exposed clothing
- Examine for eye, mucosal, and skin contamination; corneal burns/abrasions, mucosal swelling, and skin erythema, blister, or burns
- Trauma evaluation and treatment take priority over the chlorine toxicity
- Consideration of early intubation for progressive upper airway edema is required if the casualty:
- Was in close proximity to large, dense chlorine exposure (e.g. IED detonated chlorine tank) or
- Had a sustained exposure (e.g. unconscious in a chlorine filled room)
Post Discharge Follow-up
- If available, obtain PFTs with lung volume assessment and DLCO
- If PFT abnormal, obtain high resolution pulmonary CT to assess for pulmonary fibrosis
Phosgene (Carbonyl chloride, COCl2)
- Odour: sweet, pleasant smell of mowed hay (not noxious, does not prompt escape from exposure by the casualty)
- Sources: combustion of chlorinated hydrocarbons (welding, fires), synthesis of solvents (degreasers, cleaners); WW1 as a chemical weapon
- Mechanism: release of hydrochloric acid and reactive oxygen species and free radicals in the lung epithelial layers
- Water-solubility: Poor
- Signs/Symptoms: delayed ARDS (up to a day after exposure), can be very severe
- Treatment:
- Decontamination: typically not needed once clear from the exposure.
- Supportive: observation, supplemental oxygen, lung protective ventilation if required
Hydrogen Sulfide (H2S)
- Odour: rotten eggs
- Sources: waste management, petroleum, natural gas industries, and asphalt and rubber factories
- Mechanism: chemical irritant; acts like cyanide and inhibits cytochrome oxidase, preventing mitochondrial oxygen use and cellular respiration
- Water-solubility: poor
- Signs/Symptoms:
- Low concentration: skin and mucous membrane irritation
- High concentration: sudden LOC, seizure, myocardial ischemia, keratoconjunctivitis, upper airway and pulmonary injury
- Treatment:
- Supportive: removal from exposure, skin irrigation, supplemental oxygen
- Controversies:
- Consider IV hydroxocobalamin or sodium nitrite (traditional CN antidotes; some evidence in animal models)
- Note that sodium nitrite is associated with methemoglobinemia and hypotension. Infuse over 5-7 min.
- Consider IV hydroxocobalamin or sodium nitrite (traditional CN antidotes; some evidence in animal models)
Ammonia (NH3)
- Odour: pungent odour
- Sources: common industrial and household chemical used as a fertilizer, refrigerant, cleaning agent; used in plastic and explosive synthesis
- Mechanism:
- NH3 is transported under pressure in liquid form at sub-zero temperatures
- Reacts with water to form ammonium hydroxide (NH4OH), a strong base
- Water-solubility: high
- Signs/Symptoms:
- Mucosal irritation (tearing, skin irritation, eye pain and burns), severe upper airway irritation, alkali skin burns
- High concentrations or prolonged exposure: tracheobronchial and pulmonary inflammation; can produce respiratory failure within 2-5 min exposure
- Treatment:
- Supportive: skin and eye irrigation, supplemental oxygen, lung protective ventilation
- Alkali burn care
Other Common Chemical Toxins Related to Inhalation Exposures
Here is a quick summary, see the accompanying text below for more details.
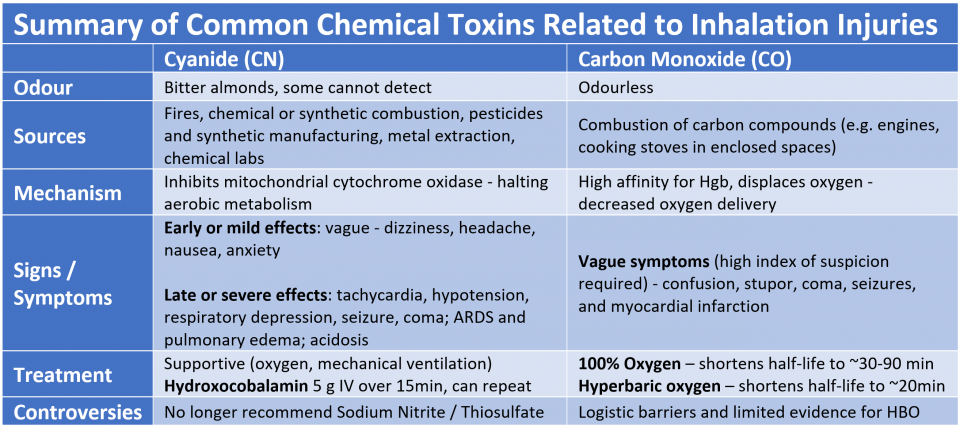
Cyanide (CN)
- Odour: bitter almonds, some cannot detect this smell
- Sources: structural and vehicle fires, chemical or synthetic material combustion, manufacturing of pesticides and synthetic materials, metal extraction, chemical laboratories
- Mechanism: inhibits mitochondrial cytochrome oxidase thereby halting cellular respiration and aerobic metabolism
- Water-solubility: high
- Signs/Symptoms:
- Early or mild effects: vague – dizziness, headache, nausea, anxiety
- Late or severe effects: tachycardia, hypotension, respiratory depression, seizure, coma; ARDS and pulmonary edema can occur
- Generally, coma precedes apnea, and then hypotension develops
- Triad of severe toxicity:
- Hypotension
- Altered mental status
- Lactic acidosis (commonly lactate > 8 mM)
- Treatment:
- Supportive: Oxygen, mechanical ventilation if required
- Rapid administration of Antidote:
- Hydroxocobalamin
- Most commonly available antidote (sold as Cyanokit®)
- Binds to CN to form cyanocobalamin (nontoxic, excreted via urine)
- 5 g IV over 15 min; 2nd dose of 5 g can be given for severe toxicity or poor clinical response
- Red discoloration of skin and urine may interfere with colorimetric assays
- Sodium Nitrite (300 mg) and Sodium Thiosulfate (12.5 g)
- Inferior to Hydroxocobalamin (superior efficacy, less toxicity)
- No longer recommended
- Nitrites have significant risk of hypotension and methemoglobinemia, which can further jeopardize tissue oxygen delivery
- Hydroxocobalamin
Carbon Monoxide (CO)
- Odour: odourless
- Sources: combustion of carbon containing compounds (e.g. combustion engines, cooking stoves in enclosed spaces)
- Mechanism:
- CO has a high affinity for hemoglobin and displaces oxygen when present which leads to decreased oxygen delivery at the tissue and mitochondrial level
- Water-solubility: poor
- Signs/Symptoms: confusion, stupor, coma, seizures, and myocardial infarction
- Treatment:
- 100% Oxygen – shortens half-life of CO to ~30-90 min (half-life normally ~3-4 hours)
- Hyperbaric oxygen – shortens half-life of CO to ~20min
- Controversies:
- Logistical factors have limited the utilization of HBO and a systematic review found insufficient evidence to determine whether HBO reduces adverse neurologic outcomes
Note: CO levels can be measured using a co-oximeter, in a blood gas; however, this may not always be available in a timely fashion. A high index of suspicion for CO poisoning is required as elevated CO may be present despite normal PaO2 and oxygen saturations
Fire Suppressants
- Chemical fire suppressants are released in military vehicle fires
- The most common is HFC227 (HFC-227EA, heptafluoropropane)
- Inert, simple asphyxiant; no cases of combustion related toxicity have been published or reported
- Can convert to hydrogen fluoride in small amounts during a fire
- Treatment is supportive
- Hydrogen fluoride (HF) as a byproduct of combustion with standard fire suppression systems may cause severe inhalation injury
- Exposure may result in rapidly progressive respiratory failure despite minimal external evidence of injury
- Present with SOB, cough, or hypoxia
- There must be a high level of suspicion
- Treatment is supportive
- If hypocalcemia: nebulized calcium gluconate (1.5 ml of 10% Ca Gluconate in 4.5 ml water) every 4 hours until normalization of serum calcium
- In the absence of significant burns, consider steroids if symptoms do not improve
- Bronchopneumonia can develop within the first week
References
- LCDR Omar Saeed, MC, USN; CPT Nathan Boyer, MC, USA; LTC Jeremy Pamplin, MC, USA; MAJ Ian Driscoll, MC, USA; MAJ Jeff DellaVolpe, USAF, MC; LtCol Jeremy Cannon, USAFR, MC; COL (ret) Leopoldo Cancio, MC, USA. Joint Trauma System Clinical Practice Guideline: Inhalation Injury and Toxic Industrial Chemical Exposure. 2016. Joint Trauma System. https://deployedmedicine.com/market/29/content/165
- Albright JM, Davis CS, Bird MD, Ramirez L, Kim H, Burnham EL et al. The acute pulmonary inflammatory response to the graded severity of smoke inhalation injury. Critical care medicine. 2012;40 (4):1113-21.
- Holstege CP, Kirk MA. Smoke inhalation. In: Goldfrank LR, ed. Goldfrank’s toxicologic emergencies. 7th ed New York: McGraw-Hill, Medical Pub. Division; 2002:1469-1477.
- Nelson LS. Simple asphyxiants and pulmonary irritants. In: Goldfrank LR, ed. Goldfrank’s toxicologic emergencies. 7th ed ed. New York: McGraw-Hill, Medical Pub. Division; 2002:1453-1468.
- Wang J, Zhang L, Walther SM. Administration of aerosolized terbutaline and budesonide reduces chlorine gas-induced acute lung injury. J Trauma. Apr 2004;56(4):850-862.
- DeLange DW, Meulenbelt J. Do Corticosteroids have a role in preventingor reducing acute toxic lung injury caused by inhalation of chemical agents? Clinical Toxicology. Vol 49, no 2. February 2011. pp 61-71
- Wang J, Abu-Zidan FM, Walther SM. Effects of prone and supine posture on cardiopulmonary function after experimental chlorine gas lung injury. Acta Anaesthesiol Scand. Oct 2002;46 (9):1094-1102.
- Vinsel PJ. Treatment of acute chlorine gas inhalation with nebulized sodium bicarbonate. J Emerg Med. 1990 May-Jun 1990;8(3):327-329.
- Pascuzzi TA, Storrow AB. Mass casualties from acute inhalation of chloramine gas. Mil Med. 1998 Feb 1998;163(2):102-104.
- Baud FJ, Borron SW, Megarbane B, et al. Value of lactic acidosis in the assessment of the severity of acute cyanide poisoning. Crit Care Med. 2002;30 (9):2044-2050.
- Bebarta VS, Pitotti RL, Dixon P, Lairet JR, Bush A, Tanen DA. Hydroxocobalamin versus sodium thiosulfate for the treatment of acute cyanide toxicity in a swine (Sus scrofa) model. Annals of emergency medicine. 2012;59 (6):532-9.
- Kealey GP. Carbon monoxide toxicity. Journal of burn care & research: official publication of the American Burn Association. 2009;30(1):146-7.
- Henry CR, Satran D, Lindgren B, Adkinson C, Nicholson CI, Henry TD. Myocardial injury and long-term mortality following moderate to severe carbon monoxide poisoning. JAMA. 2006;295 (4):398-402.
- Hampson NB. Noninvasive pulse CO-oximetry expedites evaluation and management of patients with carbon monoxide poisoning. The American journal of emergency medicine. 2012;30 (9):2021-4.
- Weaver LK. Hyperbaric oxygen therapy for carbon monoxide poisoning. Undersea & hyperbaric medicine : journal of the Undersea and Hyperbaric Medical Society, Inc. 2014;41(4):339-54.
- Bebarta VS, Tanen DA, Lairet J, Dixon PS, Valtier S, Bush A. Hydroxocobalamin and sodium thiosulfate versus sodium nitrite and sodium thiosulfate in the treatment of acute cyanide toxicity in a swine (Sus scrofa) model. Ann Emerg Med. Apr;55 (4):345-351.
- Mcdougal JN, Dodd DE. Air Force approach to risk assessment for Halon replacements. Toxicology Letter. 1993;68 (1-2):31-35.
- Emmen HH, Hoogendijk EM, Klopping-Ketelaars WA, et al. Human saftey and pharmacokinetics of the CFC alternative propellants HFC 134a (1,1,1,2- tetrafluoroethane) and HFC227 (1,1,1,2,3,3,3-heptafluoropropane) following whole-body exposure. Regul Toxicol Pharmacol. 2000;31 (1):22-35.
- Robin ML. Review of thermal decomposition product formation from halocarbon fire suppression agents: suppression of class A fires. West Lafayette, IN1999.
- Chung KK, Wolf SE, Renz EM, Allan PF, Aden JK, Merrill GA et al. High-frequency percussive ventilation and low tidal volume ventilation in burns: a randomized controlled trial. Critical care medicine. 2010;38 (10):1970-7.
