

If you work at a trauma center, then you’re bound to see your fair share of abdominal stab wounds. Though civilian penetrating trauma has declined over recent decades and is less common than blunt trauma, penetrating trauma represents ~10% of all trauma evaluations in the U.S. and of those, ~50% are caused by stab wounds.
In 2018, the Western Trauma Association (WTA) published a clinical decision algorithm outlining the diagnosis, investigation, and management of abdominal penetrating injuries from stab wounds. This algorithm focuses on adult patients with abdominal stab wounds and acknowledges the relative paucity of prospective randomized clinical trials, and thus, recommendations were based primarily on observational studies and expert opinion. The algorithm, instead of prescribing rigid recommendations, provides several equally acceptable management pathways that can be selected based on the details of the case, setting, resources, and local expertise/preference. The WTA encourages the algorithm as a general framework to be customized/adapted to each center.
In this post, we will summarize these recommendations using both visual and text formats followed by a more detailed description of the steps involved.
For other topics related to Military Medicine, please see our posts on Damage Control Resuscitation, TCCCand Recent Updates, Prolonged Field Care, Blast Injuries, Inhalation Injuries, and Resuscitative Thoracotomy.
The Algorithm: Abdominal Stab Wounds
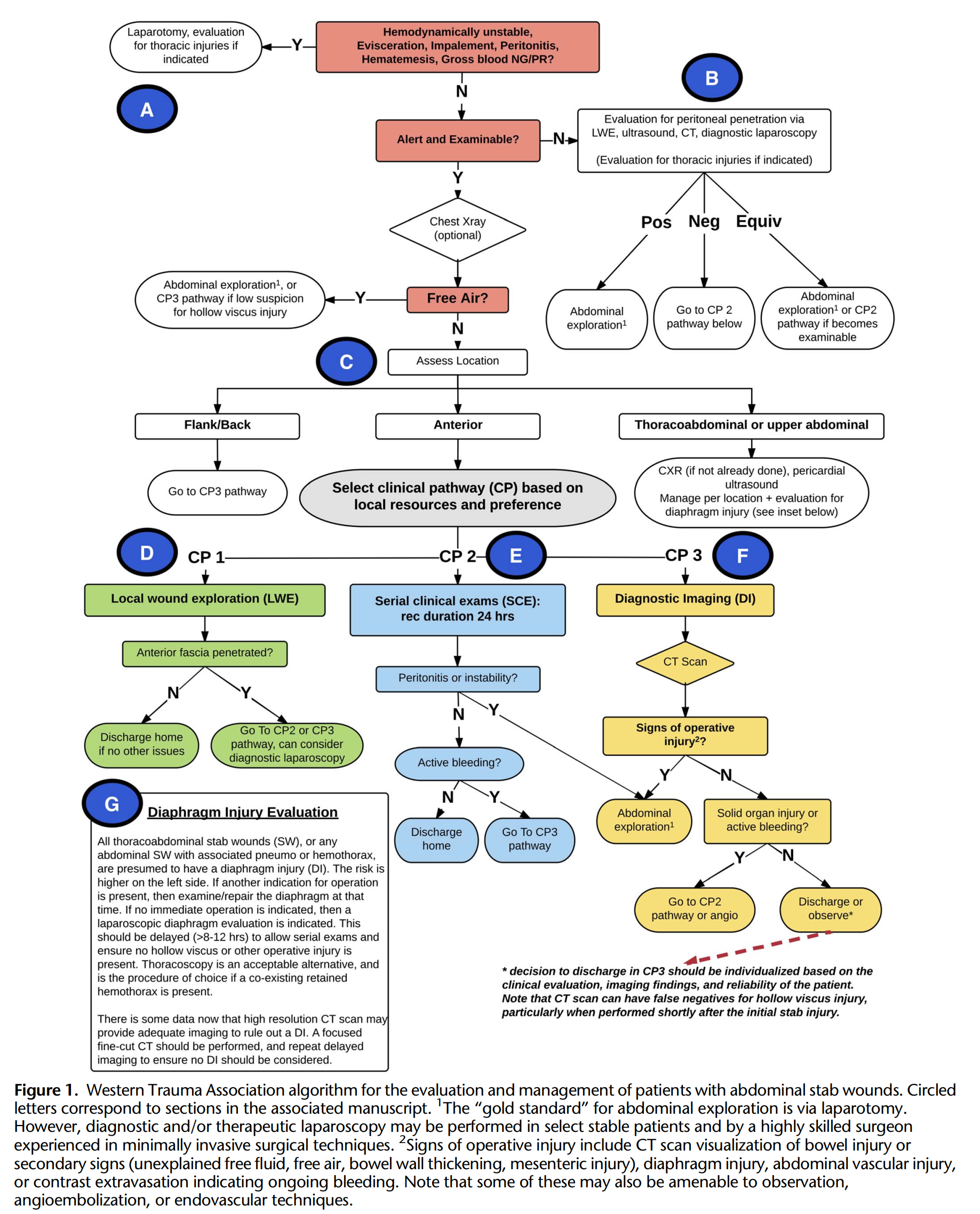
Diagnostic Questions to Ask in Abdominal Stab Wounds
Let’s break down the algorithm in text format.
First, consider thoracic injuries if indicated and investigate/manage concurrently if appropriate…
- Does this patient require immediate abdominal exploration? Yes, if:
- Hemodynamically unstable
- Evisceration
- Impalement / Implement in situ
- Peritonitis
- Hematemesis
- Gross blood NG/PR
- Does the stab wound penetrate the peritoneum?
- If alert and examinable – is there free air on CXR?
- Yes – abdominal exploration or Serial Clinical Examinations (SCE) if low suspicion for hollow viscus injury
- No – assess location (below)
- If not alert or examinable – perform Local Wound Exploration (LWE), PoCUS, Diagnostic Imaging (DI), Diagnostic Peritoneal Lavage/Aspirate, or Diagnostic Laparoscopy
- Positive – abdominal exploration
- Negative – SCE once patient is examinable
- Equivocal – abdominal exploration or SCE if patient becomes examinable
- If alert and examinable – is there free air on CXR?
- Where is the stab wound?
- Flank / Back – requires DI
- Anterior – LWE, SCE, or DI depending on local resources / preference
- Thoracoabdominal / Upper Abdominal – CXR, PoCUS for pericardial effusion, manage any thoracic injury, evaluate for diaphragm injury
Possible Management Pathways in Abdominal Stab Wounds
- Abdominal Exploration
- Gold standard is laparotomy, though laparoscopy may be performed in select stable patients
- Local Wound Exploration
- Is the anterior fascia penetrated?
- Yes – SCE or DI, can consider Diagnostic Laparoscopy
- No – DC home if no other issues
- Is the anterior fascia penetrated?
- Serial clinical exams / Observation for ~24h
- Peritonitis or instability?
- Yes – abdominal exploration
- No – Active bleeding?
- Yes – DI
- No – DC Home
- Peritonitis or instability?
- Diagnostic Imaging
- CT scan shows signs of operative injury?
- Yes – abdominal exploration
- No – Any solid organ injury or active bleeding?
- Yes – SCE or Angiography
- No – DC home or observation
- CT scan shows signs of operative injury?

A Deeper Dive into the Abdominal Stab Wound Algorithm
A. Initial Evaluation and Indications for Immediate Operation
The initial evaluation focuses on identifying immediate life-threats and injuries requiring prompt surgical repair (e.g. massive hemorrhage, hollow viscus perforation with intra-abdominal contamination). The following indications portend a high likelihood of life-threat or injury requiring surgical repair:
- Hemodynamic instability with signs of shock
- Clear warning sign for ongoing massive hemorrhage; initiate immediate exploratory laparotomy, damage control resuscitation
- No consensus for “unstable”, though majority of studies use sBP <90-100
- Evisceration – high predictor of operative injuries
- Impalement – requires removal of object under operative conditions
- Peritonitis
- Hematemesis or gross blood in the gastric aspirate / per rectum
The above factors together are 80-90% predictive of the need for therapeutic laparotomy. The factors with the best PPVs for need for laparotomy were:
- Development of hypotension after initial normotension (86%),
- Shock on presentation (83%), and
- Generalized peritonitis (81%)
For thoracoabdominal or upper abdominal stab wounds, perform immediate:
- CXR (upright or reverse trendelenburg)
- Can determine presence of intraperitoneal air, PTX/HTX
- Free air under the diaphragm should prompt consideration for immediate surgical exploration (vs. imaging or close observation if stable)
- PoCUS for pericardial effusion to r/o cardiac injury
Diagnostic Peritoneal Lavage
Though relatively sensitive for hollow viscus perforation, it has been shown to add little to the management of abdominal stab wounds in modern algorithms. Though primarily of historic interest, likely still a role for selective DPL in resource-constrained settings.
B. The Unreliable or Unexaminable Patient
- Multiple factors interfere with clinical examination (e.g. intoxication, psychiatric illness, spinal cord injury, intubated, etc.) and there is little scientific evidence for this specific cohort
- Though, routine surgical exploration in these patients is acceptable and preferable to significant diagnosis delays, the WTA (who’ve previously shown that selective radiologic imaging was safe and effective) recommend liberal use of diagnostic studies to identify peritoneal penetration and/or operative abdominal injury (e.g. FAST, LWE, CT, diagnostic laparoscopy)in these patients
- Positive findings lead to surgical exploration
- For equivocal or positive LWE (to evaluate the anterior rectus fascia for penetration), the decision for operative exploration vs serial clinical exams must be based on degree of patient impairment, duration of impairment, available resources
- In general, GCS <13 should be considered unexaminable
C. Assessing Injury Location and Location-Specific Management
- Anatomic divides are:
- Anterior
- Thoracoabdominal / Upper abdominal
- Flank / Back
- Anterior
- Costal margins to groin crease, anterior axillary lines laterally
- If no indications for immediate surgical exploration, then depending on the case, can perform LWE, SCE, or DI
- Flank / Back
- Though more subtle initial findings, there is potential for major morbidity/mortality as there is risk to retroperitoneal structures (vessels, solid organs, bowel, etc.) and colon/duodenum
- Recommend diagnostic imaging with CT abdo/pelvis
- In regards to Triple-contrast (PO, PR, IV) vs Double-contrast – final consensus was that this decision should be made at the discretion of the surgeon and radiologist
- Thoracoabdominal / Upper abdominal
- Thoracoabdominal – nipple line to costal margins
- Upper abdomen – costal margins to umbilicus
- In addition to evaluation for abdominal injuries, these also require evaluation for thoracic injuries (e.g. PTX, HTX, cardiac injury)
- pCXR, eFAST, CT Chest
- Positive findings should be managed appropriately in the context of other ongoing injuries and priorities
- Evaluation for diaphragmatic injury
- Any upper abdominal stab wound with associated PTX/HTX should be assumed to have a diaphragm injury and managed appropriately
- If another indication for surgical exploration exists, then inspect the diaphragm at that time, if not, then diagnostic laparoscopy should be performed to r/o diaphragm injury (delayed 8-12 h to allow serial examinations to ensure no other operative injury presents, requiring OR)
D. Local Wound Exploration
- Exploration to determine if the anterior fascia was penetrated; fascial penetration is a proxy for peritoneal penetration
- Important points:
- Clearly negative LWE can rule out intra-abdominal injury; safely DC home
- Positive LWE in an examinable patient should NOT be considered an immediate indication for laparotomy
- Positive LWE should prompt further diagnostic imaging or admission for serial clinical examinations
- 30–50% incidence of non-therapeutic laparotomy even with positive LWE; significantly higher false positive rates with a benign abdo exam
- Know when the patient/wound is NOT amenable to LWE:
- Small puncture wounds (i.e., ice pick)
- Long tangential stab wounds
- Flank / Back wounds – difficult to predict or follow tract due to musculature
- Significant obesity with very deep subcutaneous fat layer
- Thoracoabdominal wounds – high risk of iatrogenic PTX
- Multiple stab wounds
- Patient cooperation is required, can be difficult if intoxicated, combative, etc.
- Positive LWE should prompt further diagnostic imaging or admission for serial clinical examinations
E. Serial Clinical Examinations
- SCE is: serial abdominal exams, VS monitoring, and laboratory assessments
- Focused on identifying peritonitis (hollow viscus perforation), serious hemorrhage, or other operative injury
- Best performed in a well-resourced setting where frequent reassessments are possible
- If not, can perform routine CT imaging or diagnostic laparoscopy
- SCE is safe and reduces rates of non-therapeutic laparotomy
- When can SCE be applied:
- Abdominal stab wound
- Examinable (can consider if only short term impairment of examination)
- No indication for immediate laparotomy OR positive LWE but no immediate indications for abdominal exploration
- Though SCE is well validated, the optimal duration of observation remains unclear
- Majority of published protocols are 24-48h
- WTA recommends minimum 24h observation
F. Diagnostic Imaging
- CT scan lower chest, abdomen, and pelvis
- High resolution, 3D multiplanar reconstructions, experienced trauma radiologist
- Direct signs of operative injury = immediate surgery
- Secondary signs of possible operative injury = operative exploration vs admission for close SCE
- Any positive finding related to the stab wound, no matter how minor, should prompt admission and observation
- Negative CT scan = may allow for safe DC if examinable, reliable, low-risk vs. admission for SCE
- Considerations:
- CT can be helpful to identify signs of intra-abdominal injury, but 10-20% of injuries can be missed
- CT should not be used as the sole determinant of disposition, it should be combined with other modalities, most often SCE
G. Traumatic Diaphragm Injury (TDI) Evaluation
- TDI secondary to stab wounds is most commonly diagnosed on the left side (75% of cases)
- Right-sided TDI is diagnosed less frequently and associated with lower morbidity and mortality
- Some have recommended evaluation only for left-sided wounds. However, the liver should not be considered as reliable protection against a diaphragm injury
- These injuries are typically small and not easily identified on standard CT scan in the absence of herniated contents, therefore it is critical to adequately evaluate all patients at risk of TDI
- Some series have reported up to a 40% incidence of TDI with penetrating trauma to the left thoracoabdominal region, many of which are clinically silent
- There is some data suggesting that high resolution CT may provide adequate imaging to r/o diaphragm injury
- Focused, fine cut CT with experienced trauma radiologist should be performed
- Repeat delayed imaging to ensure no missed injury should be considered
- TDI can be diagnosed and repaired via laparoscopy; there is a role for thoracoscopy as an alternative; VATS has been used as well
References
Helman, A. Austin, E. Sayal, A. Petrosoniak, Swaminathan, A. May, N. EM Quick Hits 2 – Organophosphate Poisoning, TXA for Hemoptysis, Metacarpal Fracture Rotation, Abdominal Stab Wounds and Pediatric IV Cannulation. Emergency Medicine Cases. February, 2019. https://emergencymedicinecases.com/em-quick-hits-february-2019/. Accessed 2019/09/19.
Martin, M.J.; Brown, C.V.R.; Shatz, D.V.; Alam, H.B.; Brasel, K.J.; Hauser, C.J.; de Moya, M.; Moore, E.E.; Rowell, S.E.; Vercruysse, G.A.; Baron, B.J.; Inaba, K. Evaluation and management of abdominal stab wounds: A Western Trauma Association critical decisions algorithm. J Trauma Acute Care Surg. 2018;85: 1007–1015.
Poggio, J.L. and Schragga, E.D. Abdominal Stab Wound Exploration. [Updated 2018 May 04]. Medscape. https://emedicine.medscape.com/article/82869. Accessed 2019/08/18
Waheed A, Burns B. Penetrating Abdominal Trauma. [Updated 2019 Feb 17]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK459123/
