

Emergency Resuscitative Thoracotomy (ERT) is a potentially lifesaving intervention. It is a true salvage procedure, without which survival is essentially zero, even in indicated scenarios. After reading this post, you’ll be slightly more comfortable should you ever find yourself in a situation where you need to “crack the chest” (i.e. ERT is indicated and the appropriate surgical and resuscitative supports exist).
In this post, we will review the Joint Trauma System’s Clinical Practice Guideline on ERT and cover the background, evidence, indications, and procedure of ERT.
For a broad review of other controversies in Traumatic Cardiac Arrest, please see Dr. Nicholas Costain’s Grand Rounds Summary on the topic.
For other topics related to Military Medicine, please see our posts on Damage Control Resuscitation, TCCC and Recent Updates, Prolonged Field Care, Inhalation Injuries, Abdominal Stab Wounds, and Blast Injuries.
Background: Survival and Alternatives to Emergency Resuscitative Thoracotomy
What is the Purpose of Emergency Resuscitative Thoracotomy?
ERT identifies and allows treatment of life threats such as cardiac tamponade, penetrating cardiac injury, great vessel injury, and massive pulmonary injury. ERT allows treatment of potential sources of hemorrhage and restoration of cardiac output through these CRITICAL STEPS:
- Identification and release of cardiac tamponade
- Control of major thoracic hemorrhage
- Initiation of open/internal cardiac massage
- Cross-clamping the descending aorta to control infra-diaphragmatic hemorrhage to maximize cerebral and coronary perfusion
What are the survival rates of casualties undergoing Emergency Resuscitative Thoracotomy?
- In the Civilian literature:
- Patients undergoing ERT have high mortality rates, largely due to the nature of the injuries leading ERT
- Overall survival: 5%
- Penetrating truncal injuries: 10-30%
- Patients arriving with vital signs: 10-30%
- Patients with blunt trauma: <5%
- Patients who arrest in the field or during transport: <1%
- Likelihood of survival with intact neurologic function is significantly lower, particularly for blunt trauma and for pre-hospital arrest
- Patients undergoing ERT have high mortality rates, largely due to the nature of the injuries leading ERT
- In a combat or operational environment: several factors must be considered as studies of wartime ERT indicate reasonable probability of long-term survival in appropriately selected casualties
What are the alternatives to Emergency Resuscitative Thoracotomy?
- Surgery: For impending arrest, if immediate transfer to the OR is available, strongly consider this versus performing an ERT in the resuscitation area
- Resuscitative Endovascular Balloon Occlusion of the Aorta (REBOA) can be an alternative in the absence of thoracic bleeding
- REBOA achieves aortic occlusion, therefore, control of abdominal and pelvic hemorrhage
- Meta-analysis comparing REBOA and ERT showed that though REBOA seemed to be associated with lower mortality, there was no significant difference in survival after risk adjustment, mostly because ERT patients were more critically ill on presentation
- This suggests that REBOA is not a comparable intervention to ERT but rather may be utilized to prevent hemodynamic collapse in non-agonal unstable patients
- For more information on REBOA, see Dr. Noam Katz’s Grand Rounds on REBOA
Indications for ERT – Civilian Environment
In general, when should Emergency Resuscitative Thoracotomy be performed?
Consider ERT in patients who:
- Develop impending traumatic cardiovascular collapse or cardiac arrest…
- From a potentially reversible cause…
- That precludes immediate transport to an operating room
It is important to note that these patients (i.e. exsanguinated patients with profound hypotension or in hemorrhagic shock) do NOT improve with external chest compressions.
ERT should only be performed at a medical treatment facility with surgical and resuscitation capability by individuals familiar with and trained in this procedure.
For further information on Damage Control Resuscitation (DCR), see our summary of the JTS’s CPG on DCR
What is meant by Signs of Life (SOL)?
The indications for thoracotomy often include an assessment for “signs of life.” In this context these include:
- Pupillary response
- Spontaneous ventilation
- Presence of carotid pulse
- Measurable or palpable blood pressure
- Extremity movement
- Organized cardiac activity
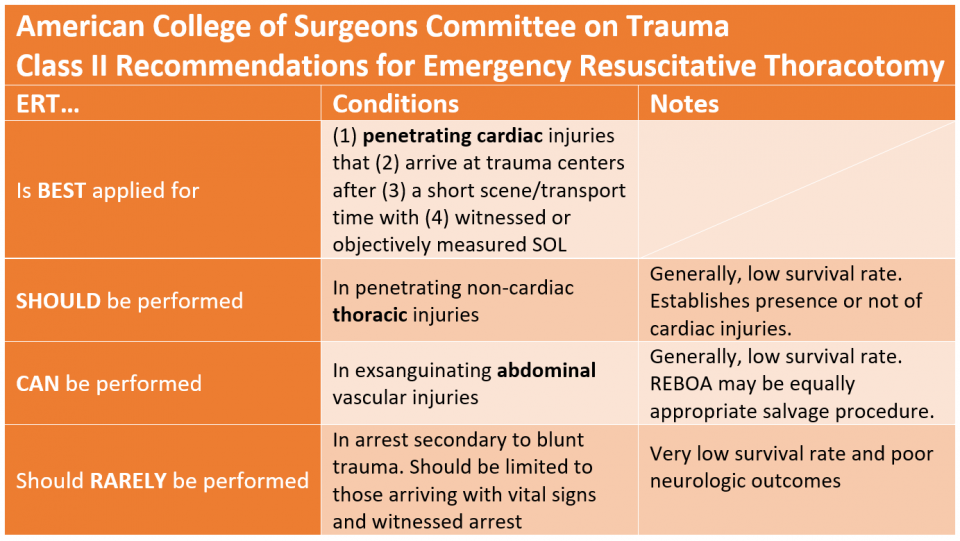
What are the CIVILIAN indications for Emergency Resuscitative Thoracotomy?
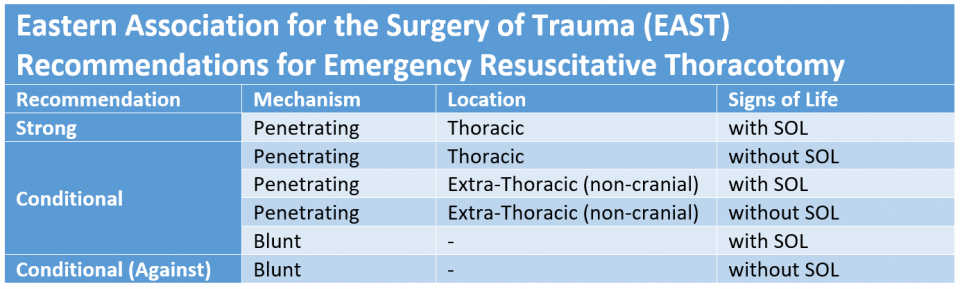
ERT is generally indicated only for penetrating trauma with either witnessed cardiac arrest or recent loss of vital signs. Below are the recommendations for ERT as put forth by the American College of Surgeons, the Western Trauma Association, and the Eastern Association for the Surgery of Trauma.
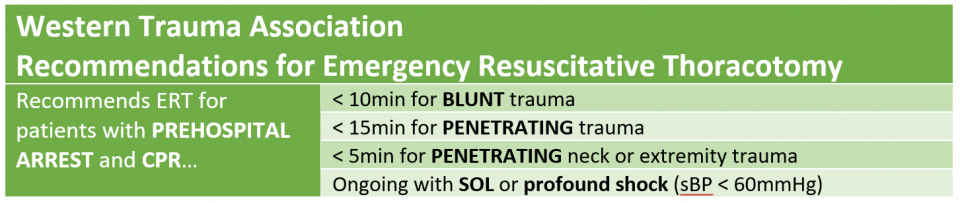
WTA’s recommendation in blunt trauma is more liberal than other associations that recommend against ERT in this cohort
Eastern Association for the Surgery of Trauma (EAST) identified 6 pre-defined patient categories depending on 3 conditions in pulseless patients:
- Penetrating vs Blunt
- Thoracic vs Extra-thoracic
- Presence/Absence of SOL
Indications for ERT – Military Environment
What are the Specific Considerations for performing Emergency Resuscitative Thoracotomy in the Military context?
- Major differences in the epidemiology of patients
- Younger and healthier
- Penetrating or combined blast/penetrating mechanisms
- Local tactical environment and the impact on critical resources may supersede clinical factors
- ERT is resource-intensive
- Considering the low overall yield of ERT, the decision to proceed must consider the impact on the medical treatment facility’s overall capabilities
- g. ERT should NOT be performed during mass casualty events
- ERT should only be performed in a setting with surgical capabilities, proper equipment, and an adequate supply of blood products
What is the available literature for Emergency Resuscitative Thoracotomy in the Military context?
Case series of 101 patients based on four-year data from a Role 3 facility in Iraq examined outcomes after ERT in the context of combat trauma
-
- Return of perfusing rhythm in HALF, with 46% survival to OR, and 12% survival to evacuation
- All survivors reported to have good functional outcomes and neurologically intact
- No reported difference in survival based on injury mechanism, location, or injury pattern
- Primary mechanisms were explosive injury and gunshot wounds
- This case series suggests similar or better survival after combat trauma ERT compared with civilian results of ERT
- A previous study limited to wartime penetrating thoracic trauma with cardiac injuries showed, among 17 patients undergoing ERT, a 24% survival rate
- These results were confirmed in a more recent study examining 65 patients at a Role 3 facility in Afghanistan. The mechanisms were again all blast and gunshot wounds.
- Overall survival: 22%
- Traumatic arrest in the field: No survival
- Survival rate if:
- Vital signs in the field, arrest during transport: 10% 30-day survival
- Arrest at treatment facility: 42% 30-day survival
- Demonstrated time sensitive nature of ERT; the average time from arrest to ERT was:
- 6 min in survivors
- 18 min in non-survivors
- A recent retrospective 8-year study of Operations Enduring and Iraqi Freedom ERTs showed 9.9% survival rate among 81 patients
What are the Indications for Emergency Resuscitative Thoracotomy in the Military environment?
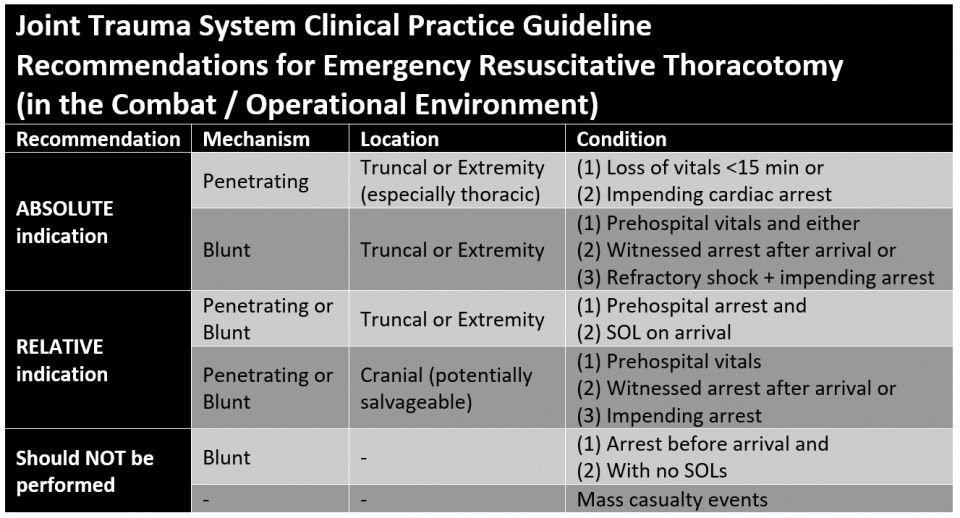
Note that for penetrating truncal/extremity trauma (especially thoracic) with loss of vitals < 15 min or impending cardiac arrest, up to 25% can be salvaged with acceptable neurological outcomes.
ERT should NOT be performed in multiple or mass casualty events or when performance will expend critical resources (such as blood products/surgeons/ORs) needed for more salvageable patients.
What are some special considerations for the Military context?
- Patients with low likelihood of salvage (e.g. severe TBI, high total BSA burns), should be either declared expectant or (at most) managed with nonoperative resuscitation and interventions (intubation, chest tubes, fluid/blood resuscitation) and then reassessed
- In arrested or peri-arrest patients with severe blunt or penetrating TBI, ERT is generally contraindicated unless there is:
- Evidence of preserved neurologic function and
- Potentially salvageable and survivable brain injury
How do you Perform an Emergency Resuscitative Thoracotomy?
What are the CRITICAL ADJUNCTS required for successful Emergency Resuscitative Thoracotomy?
- Adequate IV, IO or central line access
- Endotracheal intubation
- Initiation of damage control resuscitation and massive transfusion protocol
- Placement of OG/NG
What are the 7 STEPS of an Emergency Resuscitative Thoracotomy?
- Left anterior-lateral thoracotomy incision
- Opening the pericardium
- Control of cardiac injury
- Temporary control of active lung bleeding
- Cross-clamping of the descending aorta
- Internal cardiac massage and defibrillation
- Repair of other thoracic, abdominal, or peripheral injuries
When is extension to a bilateral thoracotomy (“CLAM SHELL”) or simultaneous right anterolateral thoracotomy indicated?
- Evidence of right thoracic or mediastinal injury not reached from the left side
Steps to Perform Emergency Resuscitative Thoracotomy in Detail
Preparation
- Don appropriate PPE; effective suction should be available
- Sterile preparation is not required
- If possible, obtain definitive airway control prior (but do not delay ERT)
- Simultaneous IV and IO access for blood product infusion
- Strongly consider right chest tube placement if there is any possibility of injury on the right side
- Alternatively, perform an extended thoracotomy or clamshell incision
Incision and Exposition
- Generous curvilinear left anterolateral thoracotomy (from sternum to table) at
~ 4th ICS (nipple line in males, inframammary crease in females; if in doubt, err superiorly)- If a left chest tube was previously performed, this can be the starting point
- Exposure is improved by placing a towel/roll under the left back to elevate the left chest
- NOTE: One of the most common technical errors in ERT is poor exposure due to inadequate length of the skin incision and lack of complete division of the subcutaneous and muscle layers
- Initial incision should travel to/through the chest wall muscles
- Then use heavy scissors to rapidly open the remaining tissue layers by sliding the partially opened scissors along the superior rib border
- The internal mammary artery is 1-2cm lateral to the sternal border and will be cut
- Control of bleeding (only after ROSC) with suture or clips will be necessary
- If after initial left ERT, additional right-sided thoracic, cardiac, or pulmonary hilar exposure is needed, the incision should rapidly be extended across the sternum (with a Lebsche knife or simple trauma shears) and continued on the right side (bilateral thoraco-sternotomy or “clamshell” incision)
- Once incision is complete, place a rib retractor (with handle downward), spread the ribs, and pack the lung posteriorly or have an assistant manually retract it
- This can be facilitated by incision of the inferior pulmonary ligament
- After evacuating blood and/or formed clot from the left pleural space, the pericardium is visualized to assess for cardiac activity and for hemopericardium.
Cardiac Procedures
- Pericardotomy:
- Open the pericardium longitudinally at least one fingerbreadth anterior to the
phrenic nerve- To do this, grasp the pericardium with forceps and cut using scissors (note: tension from a large hemopericardium can make grasping the pericardium with forceps difficult)
- This cut should extend from the thoracic inlet superiorly to the diaphragm inferiorly
- Partially deliver the heart out of the pericardium to inspect for injury and facilitate open cardiac massage if needed
- To do this, grasp the pericardium with forceps and cut using scissors (note: tension from a large hemopericardium can make grasping the pericardium with forceps difficult)
- Open the pericardium longitudinally at least one fingerbreadth anterior to the
- Control of Cardiac Injury:
- If cardiac injury is identified, initial temporary control may be achieved with digital pressure, a large side-biting clamp, a Foley catheter, or a skin stapler
- Open Cardiac Massage:
- Rapidly institute open cardiac massage in the absence of effective cardiac activity
- Use a two-handed technique (less traumatic, better cardiac output)
- Internal Defibrillation
- Defibrillation must be attempted early in cardiac arrest
- If internal paddles are available, a shock is delivered at 20 Joules
- If there is no cardiac injury and no cardiac activity (asystole), resuscitative efforts should be terminated after a reasonable time (5-10 minutes)
- In case of successful restoration of cardiac activity, injuries should be more definitively repaired and exploration completed
Aortic Cross-Clamping
- If there is known or suspected hemorrhage below the diaphragm, initial attention after
thoracotomy should be focused on clamping the descending thoracic aorta- Retract the lung, pack it anteriorly and superiorly to identify the aorta
- To facilitate moving the lung, incise the inferior pulmonary ligament
- Open the mediastinal pleura and perform limited blunt dissection to expose the aorta
- Occlude the aorta with a large, atraumatic DeBakey vascular clamp just above the diaphragm to maximize collateral flow and spinal cord perfusion
- Note that in exsanguinated or asystolic patients, the esophagus is easily
mistaken for the aorta - If there is confusion, place an OG or NG to identify the esophagus
- Note that in exsanguinated or asystolic patients, the esophagus is easily
- Retract the lung, pack it anteriorly and superiorly to identify the aorta
- After the clamp is placed, aggressively resuscitate and make immediate plans made for direct surgical control
- If a patient remains severely hypotensive despite fluid resuscitation after aortic clamping, it is unlikely that they have a survivable injury
- Duration of cross clamping should be carefully monitored
- Maximum tolerated duration in hemorrhagic shock is 30-40 minutes
- The clamp should be removed at the earliest possible time
- The clamp can be moved inferiorly to the abdominal aorta or iliac vessels if proximal control of abdominal, pelvic, or extremity vascular injuries is still required
- When the clamp is removed, be prepared for rapid hemodynamic shifts, hyperkalemia, and/or metabolic acidosis (ischemia-reperfusion injury or “reperfusion syndrome”)
Thoracic Injury
- If there is direct injury to the lung or hilar vessels, direct pressure is generally sufficient for temporary control of bleeding (low pressure system)
- Some major pulmonary injuries may require hilar cross-clamping to control bleeding
- Once temporary control is in place, resuscitate and plan for immediate definitive lung repair
- Large pulmonary injuries create a risk for air embolism
- Early hilar clamping, rapid direct control of lung lacerations, or temporarily submerging the area in irrigation fluid can help prevent this risk
- Thoracic great vessel injury can be temporarily controlled with digital pressure or atraumatic vascular clamps
- If this is insufficient, this likely represents a non-survivable injury
- Intercostal and chest wall bleeding (arterial) will require more focal and firm pressure for initial control, followed by mass suture ligatures and/or clip
References
- Lt Col Tristan Monchal, French Army MC; COL Matthew J. Martin, MC, USA; Maj Stephanie Streit, USAF, MC; CDR Jared L. Antevil, MC, USN; CAPT Donald R. Bennett, USAF, MC; COL(ret) William C. DeVries, MC, USA; Lt Col Scott Zakaluzny, USAF, MC; CDR Robert L. Ricca, MC, USN; COL Homer Tien, Canadian Forces Health Services; LTC Philip S. Mullenix, MC, USA; CAPT Zsolt T. Stockinger, MC, USN. Emergency Resuscitative Thoracotomy. Joint Trauma System Clinical Practice Guideline. 2018.
- Mattox KL, Feliciano DV. Role of external cardiac compression in truncal trauma. J Trauma 1982;22:934-6.
- Rhee PM, Acosta J, Bridgeman A, Wang D, Jordan M, Rich N. Survival after emergency department thoracotomy: review of published data from the past 25 years. J Am Coll Surg 2000;190:288-98.
- Working Group AHSoOACoSCoT. Practice management guidelines for emergency department thoracotomy. Working Group, Ad Hoc Subcommittee on Outcomes, American College of Surgeons-Committee on Trauma. J Am Coll Surg 2001;193:303-9.
- Seamon MJ, Fisher CA, Gaughan JP, Kulp H, Dempsey DT, Goldberg AJ. Emergency department
thoracotomy: survival of the least expected. World J Surg 2008;32:604-12. - Moore EE, Knudson MM, Burlew CC, et al. Defining the limits of resuscitative emergency department thoracotomy: a contemporary Western Trauma Association perspective. J Trauma 2011;70(2):334-9.
- DiGiacomo JC, Odom JW, Swan KG, Salant M. Resuscitative thoracotomy and combat casualty care. Mil Med 1991;156:406-8.
- MacFarlane C. Emergency thoracotomy and the military surgeon. ANZ J Surg 2004;74:280-4
- Edens JW, Beekley AC, Chung KK, et al. Longterm outcomes after combat casualty emergency department thoracotomy. J Am Coll Surg 2009;209:188-97.
- Morrison JJ, Poon H, Rasmussen TE, et al. Resuscitative thoracotomy following wartime injury. J Trauma Acute Care Surg 2013;74:825-9.
- Mitchell TA, Waldrep KB, Sams VG, Wallum TE, Blackbourne LH, White CE. An 8-year review of operation enduring freedom and operation iraqi freedom resuscitative thoracotomies. Mil Med 2015;180(3 Suppl):33-6.
- Burlew CC, Moore EE, Moore FA, et al. Western Trauma Association critical decisions in trauma: resuscitative thoracotomy. J Trauma Acute Care Surg 2012;73:1359-63.
- Seamon MJ, Haut ER, Van Arendonk K, et al. An evidence-based approach to patient selection for emergency department thoracotomy: A practice management guideline from the Eastern Association for the Surgery of Trauma. J Trauma Acute Care Surg 2015;79:159-73.
- Davies GE, Lockey DJ. Thirteen survivors of prehospital thoracotomy for penetrating trauma: a prehospital physician-performed resuscitation procedure that can yield good results. J Trauma 2011;70:E75-8.
- Coats TJ, Keogh S, Clark H, Neal M. Prehospital resuscitative thoracotomy for cardiac arrest after
penetrating trauma: rationale and case series. J Trauma 2001;50:670-3. - DuBose J, Fabian T, Bee T, Moore LJ, Holcomb JB, Brenner M, Skarupa D, Inaba K, Rasmussen TE, Turay D, Scalea TM; and the AAST AORTA Study Group. Contemporary Utilization of Resuscitative Thoracotomy: Results from the AAST Aortic Occlusion for Resuscitation in Trauma and Acute Care Surgery (AORTA) Multicenter Registry. Shock 2017. doi: 10.1097/SHK.0000000000001091.
- Aso S, Matsui H, Fushimi K, Yasunaga H. Resuscitative endovascular balloon occlusion of the aorta or resuscitative thoracotomy with aortic clamping for noncompressible torso hemorrhage: A retrospective nationwide study. J Trauma Acute Care Surg 2017;82:910-4.
- DuBose JJ, Scalea TM, Brenner M, Skiada D, Inaba K, Cannon J, Moore L, Holcomb J, Turay D, Arbabi CN, Kirkpatrick A, Xiao J, Skarupa D, Poulin N; AAST AORTA Study Group. The AAST prospective Aortic Occlusion for Resuscitation in Trauma and Acute Care Surgery (AORTA) registry: Data on contemporary utilization and outcomes of aortic occlusion and resuscitative balloon occlusion of the aorta (REBOA). J Trauma Acute Care Surg 2016;81:409-19.
- Moore LJ, Brenner M, Kozar RA, Pasley J, Wade CE, Baraniuk MS, Scalea T, Holcomb JB. Implementation of resuscitative endovascular balloon occlusion of the aorta as an alternative to resuscitative thoracotomy for noncompressible truncal hemorrhage. J Trauma Acute Care Surg 2015;79:523-30; discussion 530-2.
- Manzano Nunez R, Naranjo MP, Foianini E, Ferrada P, Rincon E, García-Perdomo HA, Burbano P, Herrera JP, García AF, Ordoñez CA. A meta-analysis of resuscitative endovascular balloon occlusion of the aorta (REBOA) or open aortic cross-clamping by resuscitative thoracotomy in non-compressible torso hemorrhage patients. World J Emerg Surg 2017;12:30.
- Joint Trauma System, REBOA for Hemorrhagic Shock CPG, 06 Jul 2017. https://jts.amedd.army.mil/assets/docs/cpgs/JTS_Clinical_Practice_Guidelines_(CPGs)/REBOA_for_Hemorrhagic_Shock_06_Jul_2017_ID38.pdf. Accessed Mar 2018
- Morrison JJ, Mellor A, Midwinter M, Mahoney PF, Clasper JC. Is pre-hospital thoracotomy necessary in the military environment? Injury 2011;42:469-73.
- Jebara VA, Saade B. Penetrating wounds to the heart: a wartime experience. Ann Thor Surg 1989;47:250-3.
- Martin MJ, Beekley A. Front Line Surgery: A Practical Approach (Second edition). New York: Springer Publishing Inc.; 2017.
- Joint Trauma System, Infection Prevention in Combat-Related Injuries, 08 Aug 2016. http://jts.amedd.army.mil/assets/docs/cpgs/JTS_Clinical_Practice_Guidelines_(CPGs)/Infection_Prevention_in_Combat-Related_Injuries_08_Aug_2016_ID24.pdf. Accessed Jun 2018.
- Joint Trauma System, Damage Control Resuscitation. 03 Feb 2017. http://jts.amedd.army.mil/assets/docs/cpgs/JTS_Clinical_Practice_Guidelines_(CPGs)/Damage_Control_Resuscitation_03_Feb_2017_ID18.pdf. Accessed Jun 2018.
- Borden Institute, US Army Medical Department and School, Office of the Surgeon General (US Army). Emergency War Surgery. Fourth United States Revision. 2013. http://www.cs.amedd.army.mil/FileDownloadpublic.aspx?docid=80035d1a-f208-473d-993b-6debfb17db91 Accessed Jun 2018.
