
I think we’re all pretty much ready for the end of 2020, what a year it has been. It seems fitting that our most viewed article here at EMOttawa this year was on the management of hemorrhoids. Taking a walk down memory lane, we present our 10 most popular posts this year. Click on the title of each post to read more! We’d like to thank everyone who has contributed to the blog over the past year, and all of our readers ! Now, without further ado:
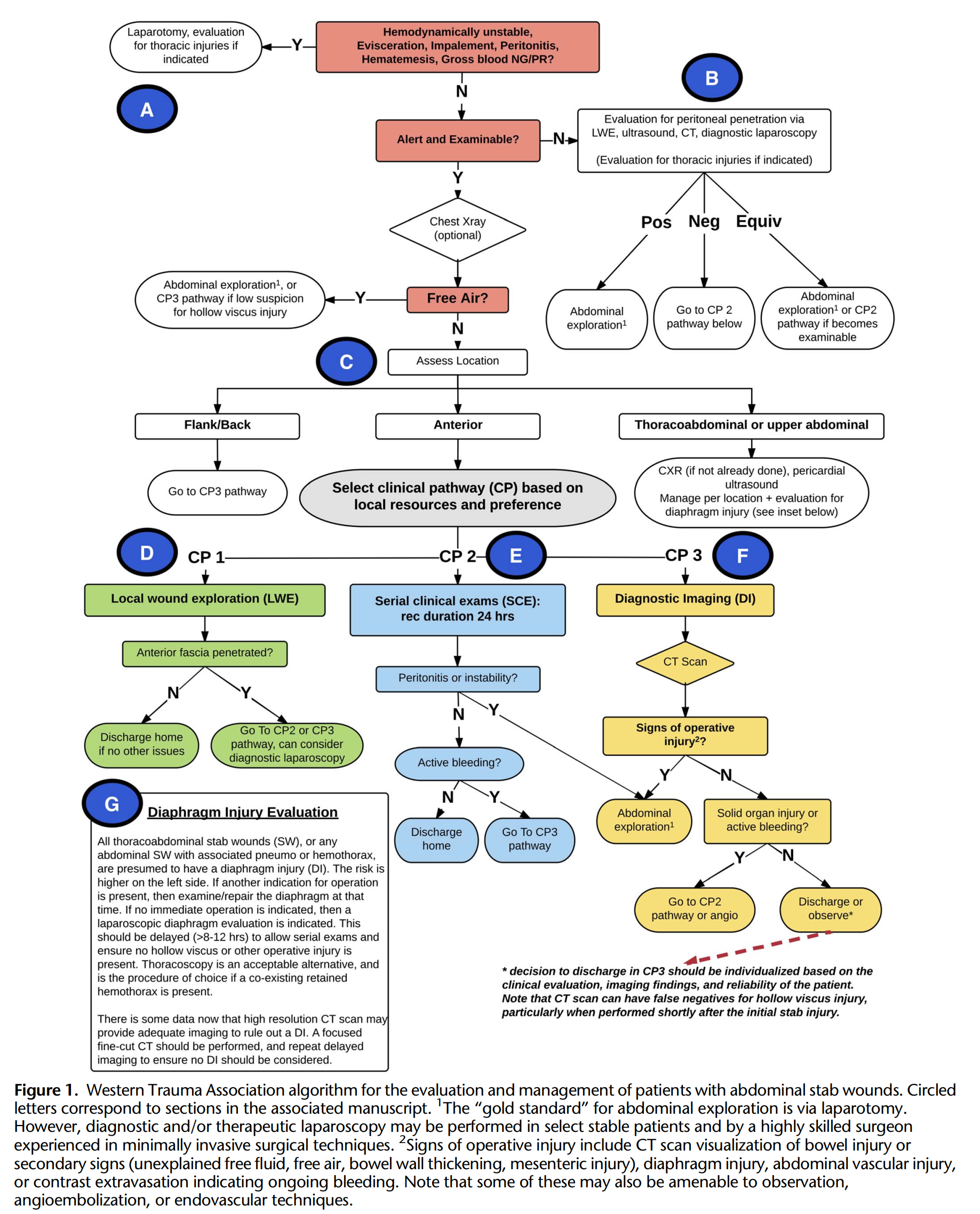
10. An Algorithmic Approach to Abdominal Stab Wounds
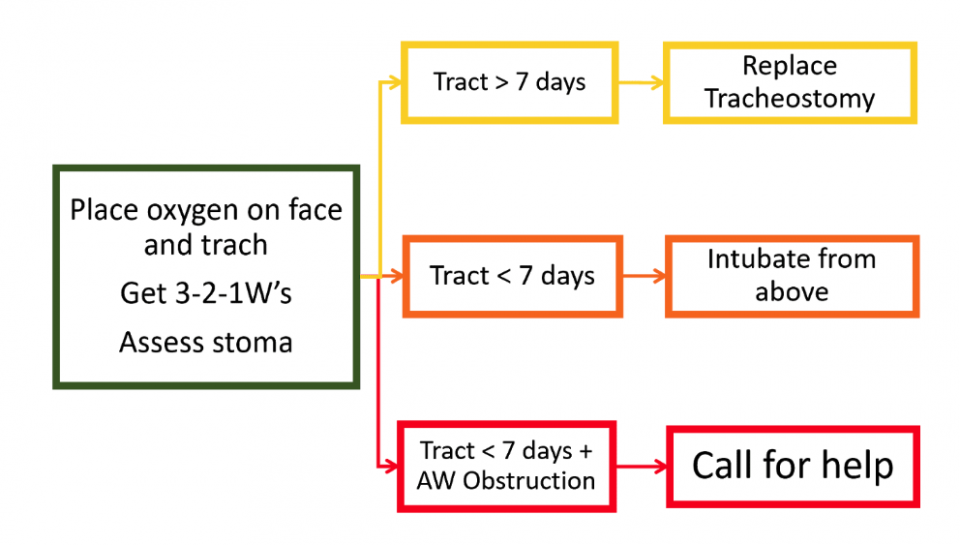
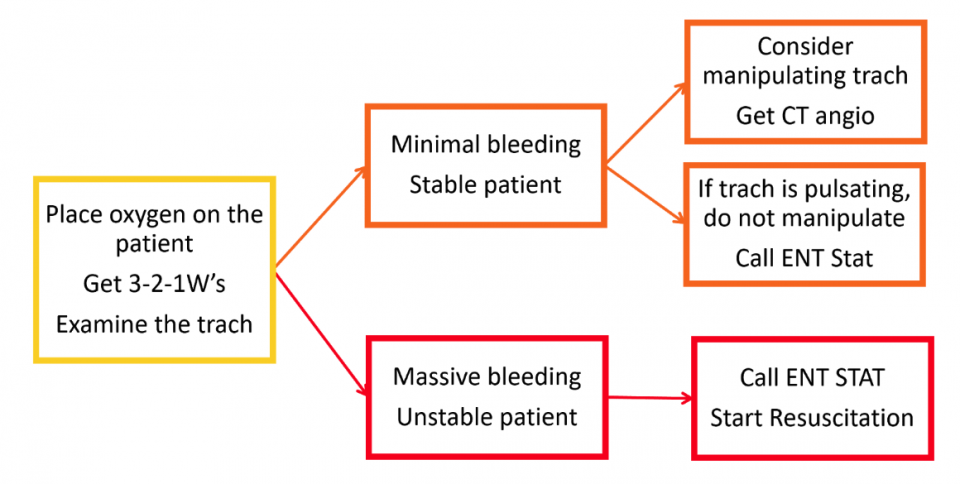
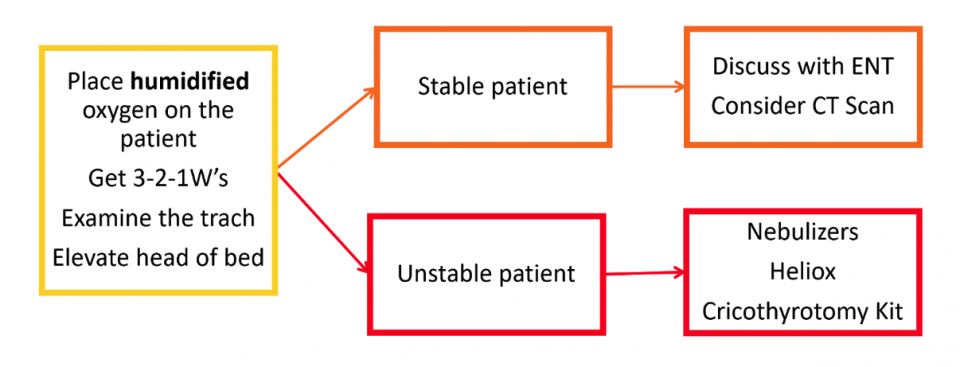
9. Tricks of the Trach’
Providing an approach to tracheostomy’s in the ED, and common presenting complaints.
Obstruction
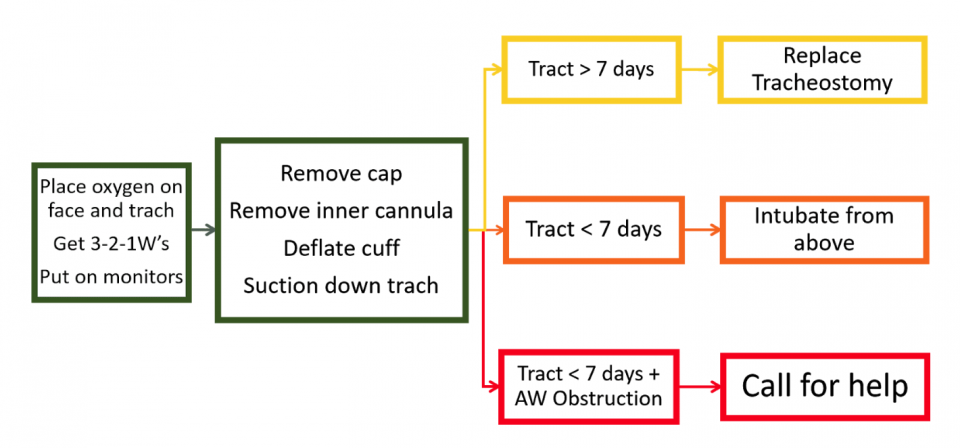
Decannulation
Bleeding
Tracheal Stenosis
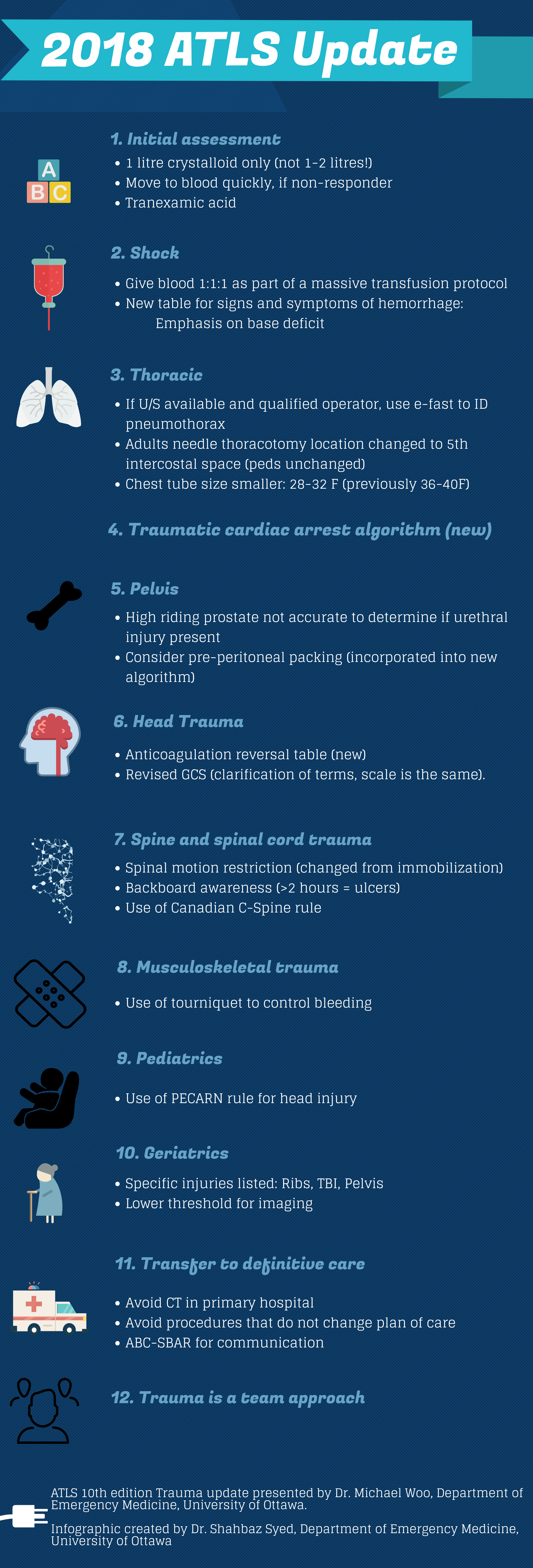
8. ATLS Trauma Update
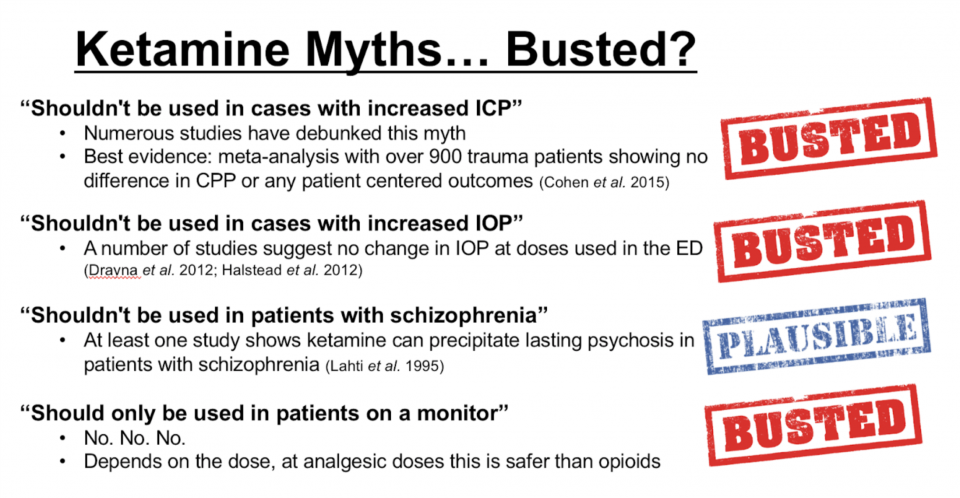
7. Update From the K-Hole: Ketamine in the ED
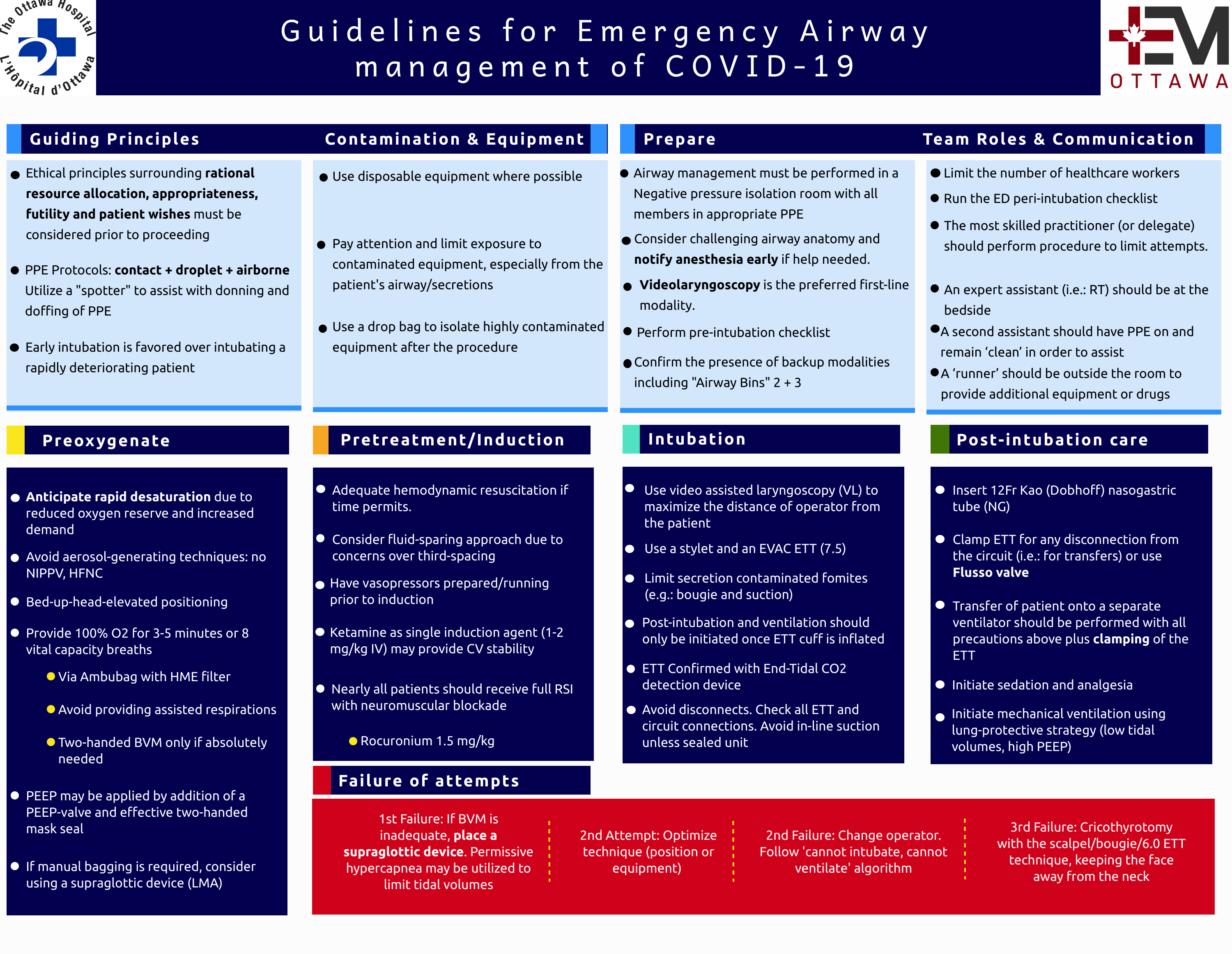
6. Guidelines for Emergency Airway Management of COVID-19
5. EMOttawa Handbook of Emergency Medicine
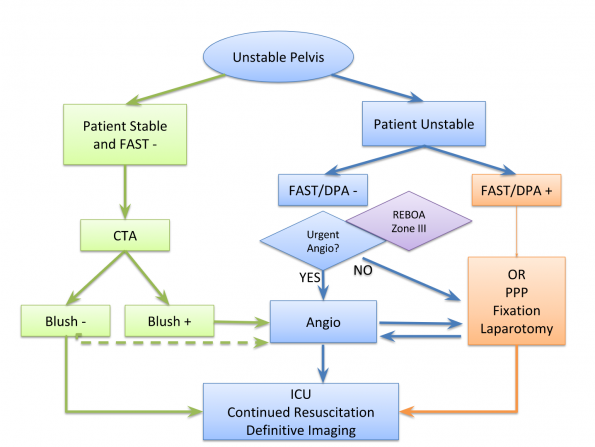
4. Pelvic Trauma in the ED
3. Managing Stress and Anxiety Related to COVID-19
- Knowledge is power – but reduce the noise
- COVID-19: Facts vs Fear
- Hope fo the best but plan for the worst
- Now is the time for self-care
- Talk it out, dont completely self-isolate
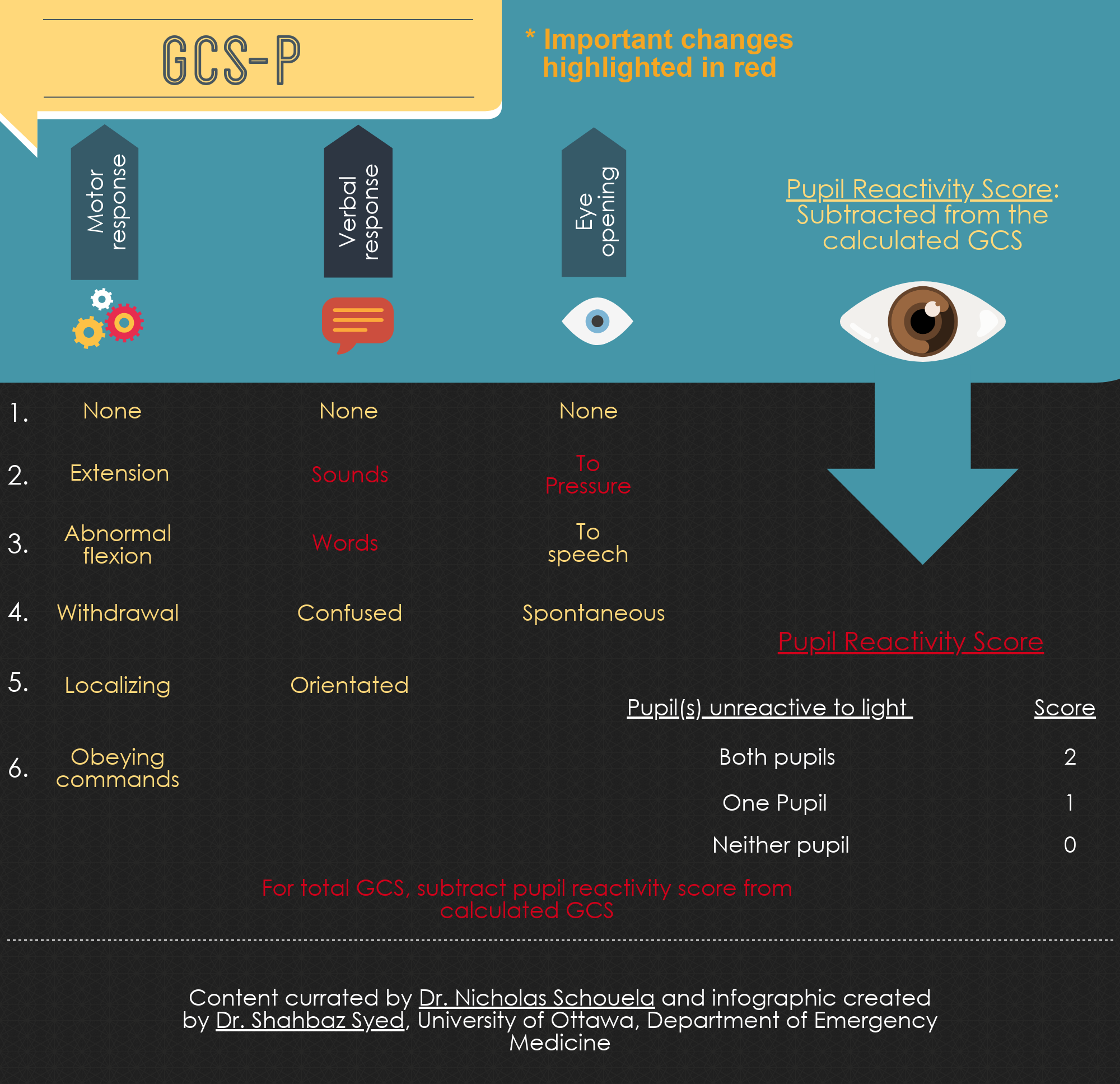
2. GCS Remastered: Recent updates to the Glasgow Coma Scale (GCS-P)
1. The Bottom Line: Hemorrhoids and Anal Fissures in the ED
Management – Internal Hemorrhoids
The American Society of Colon and Rectal Surgeons (ASCR) suggests warm water (“sitz”) immersion, oral analgesia, stool softener, and high fibre as first-line management of hemorrhoids.4 However, of these therapies, only fibre has any literature surrounding its use. A systematic review in 20065 identified 7 studies with a total of 378 patients looking at fibre for hemorrhoids: the most recent was performed in 1996 and overall there were concerns with blinding, concealment, and loss to follow-up. Overall, however, the meta-analysis showed fibre having statistically significant benefit for bleeding (RR=0.5) and overall improvement (RR=0.53) with a minimal side effect profile. Local practice at The Ottawa Hospital (TOH) is to recommend 25-30g of fibre a day.16
Of note, the ASCR does not recommend topical preparations for hemorrhoid therapy as there are no studies evincing benefit and these medications carry the risk of sensitization and contact dermatitis.4
Phlebotonics
Phlebotonics are a diverse family of plant-derived and semisynthetic compounds whose proposed method of action is to strengthen blood vessel walls, increase venous tone, improve lymphatic drainage, and normalize capillary permeability. Though not common in Canada, they can be used to treat varicose veins and symptomatic hemorrhoids. A Cochrane meta-analysis and systematic review of phlebotonics for hemorrhoids6 found 24 studies involving 2334 patients. Multiple formulations, variable quality, multiple endpoints, and multiple confounders mean that results should be interpreted with caution. However, there was a statistically significant benefit for the reduction of bleeding (OR=0.12), discharge (OR=0.12), and overall benefit (OR=15.98), with a beneficial trend for pain and pruritis. There was a minimal side effect profile involving gastrointestinal discomfort. The only phlebotonic approved for sale in Canada is MPFF (micronized purified flavonoid fraction) under the trade name VenixxaTM, which was used in 13 of the 24 studies included in the Cochrane review. It is sold over the counter. A single box costs approximately 32$ and contains a full course of treatment (1500mg BID for 4 days, then 1000mg BID for 3 days).7
Management – External Hemorrhoids
Much of the literature around hemorrhoids focuses specifically on internal hemorrhoid management. Regarding external hemorrhoids, and specifically thrombosed external hemorrhoids, there is significant practice variation around incision and expression of clot. A single systematic review without meta-analysis8 identified only two papers comparing surgical and supportive therapy for thrombosed external hemorrhoid: while surgical outcomes were promising (significant difference in resolution of symptoms after four days), the procedures performed were overwhelmingly excision of clot and hemorrhoid, as opposed to incision. Given the real risk of bleeding, wound infection, prolonged pain, and poor wound healing, incision and expression of clot is not recommended in the ED, and surgical consultation should be considered if immediate pain relief is desired.16
